📋 Key Information Summary
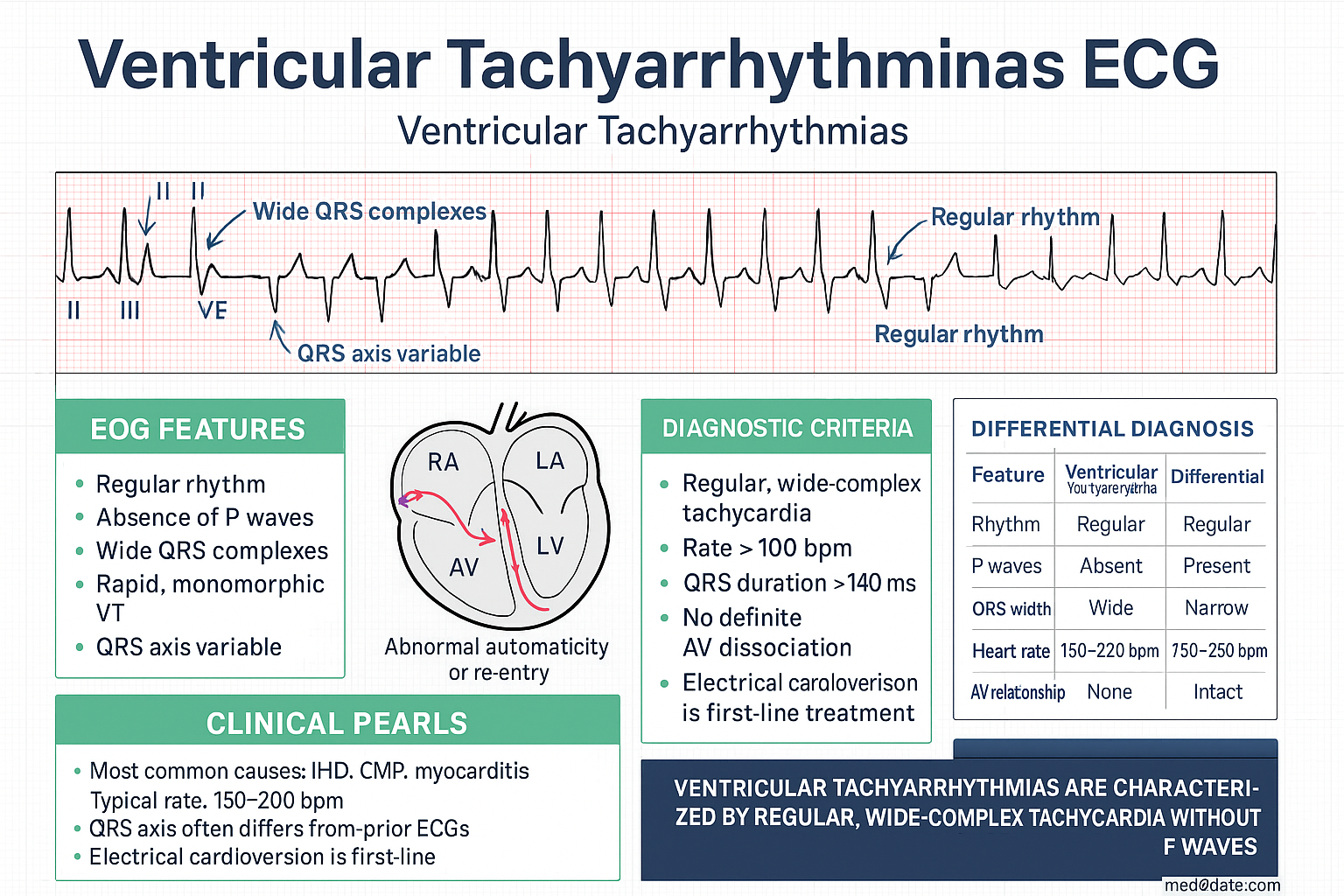
- Ventricular tachyarrhythmias encompass sustained monomorphic VT, polymorphic VT, torsades de pointes (TdP), ventricular fibrillation (VF), and inherited arrhythmia syndromes — all carry significant mortality risk in the Australian population.
- Sustained monomorphic VT most commonly arises from structural heart disease (ischaemic cardiomyopathy, dilated cardiomyopathy, valvular disease); echocardiography and cardiac MRI are essential baseline investigations.
- Catheter ablation is first-line for recurrent idiopathic VT and an important adjunct for VT in structural heart disease; refer to an electrophysiology centre (available in all Australian capital cities and select regional centres).
- Antiarrhythmic drugs — amiodarone, sotalol, and flecainide are PBS-listed; mexiletine is available under Special Access Scheme. Beta-blockers are first-line for nearly all ventricular arrhythmia substrates.
- Polymorphic VT in the setting of normal QT is managed as per VT with structural heart disease; torsades de pointes requires immediate IV magnesium sulphate and correction of QT-prolonging factors.
- All QT-prolonging medications must be reviewed and ceased — use the CredibleMeds database and Australian Adverse Drug Reaction Advisory Committee (ADRAC) lists.
- Ventricular fibrillation is the most common initial rhythm in out-of-hospital cardiac arrest (OHCA); early defibrillation and bystander CPR are the most impactful interventions per ANZCOR guidelines.
- Targeted temperature management (TTM) at 32–36°C for ≥24 hours is recommended for all comatose post-cardiac-arrest patients per ANZCOR and ILCOR consensus.
- ICD implantation is indicated for secondary prevention after cardiac arrest or sustained VT (with reduced LVEF) and for primary prevention when LVEF ≤35% despite ≥3 months of optimal medical therapy (NHFA/CSANZ guidelines).
- ICD programming should use high-rate detection zones (≥188–200 bpm) and prolonged detection intervals to reduce inappropriate shocks; all Australian patients should be enrolled in remote monitoring (e.g., Medtronic CareLink, Abbott Merlin).
- Electrical storm (≥3 VT/VF episodes in 24 hours) requires emergent management with IV amiodarone, beta-blockade, sedation, and urgent electrophysiology referral for consideration of catheter ablation.
- Inherited arrhythmia syndromes — Brugada syndrome, catecholaminergic polymorphic VT (CPVT), and arrhythmogenic right ventricular cardiomyopathy (ARVC) require specialised genetic counselling, family screening, and risk-stratified management at dedicated inherited arrhythmia clinics.
- Aboriginal and Torres Strait Islander peoples have higher rates of rheumatic heart disease, cardiomyopathy, and sudden cardiac death, with significant barriers to electrophysiology services in remote and regional areas.
Introduction & Australian Epidemiology
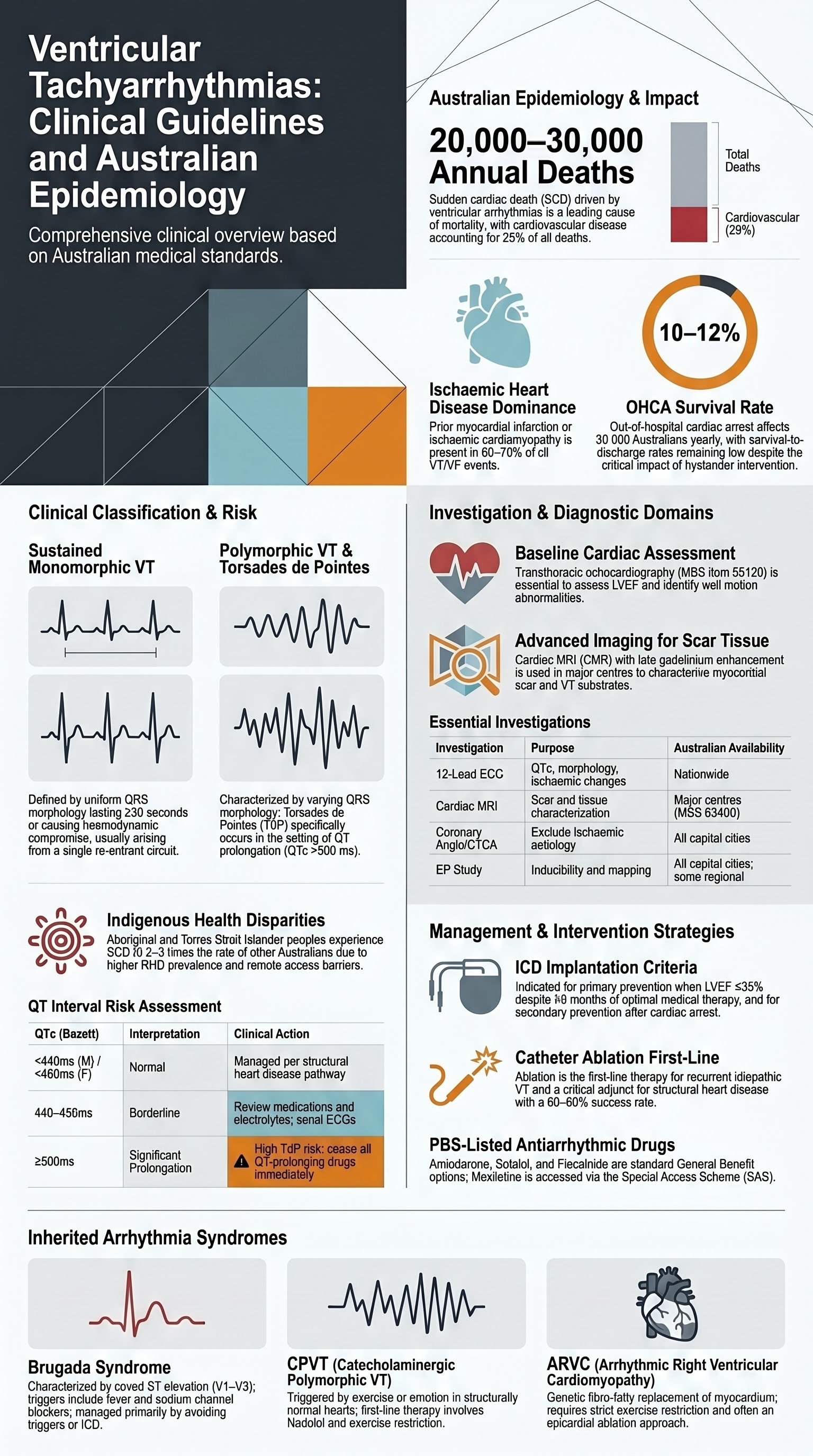
Ventricular tachyarrhythmias are a heterogeneous group of rapid heart rhythms originating below the bundle of His, ranging from relatively benign idiopathic ventricular tachycardia (VT) to immediately life-threatening ventricular fibrillation (VF). They are a leading cause of sudden cardiac death (SCD), which accounts for approximately 20,000–30,000 deaths annually in Australia.
The epidemiology of ventricular tachyarrhythmias in Australia reflects the broader cardiovascular disease burden. Ischaemic heart disease remains the leading predisposing condition, with an estimated 60–70% of VT/VF events occurring in patients with prior myocardial infarction or ischaemic cardiomyopathy. The Australian Institute of Health and Welfare (AIHW) reports that cardiovascular disease accounts for approximately 25% of all deaths, with arrhythmias contributing significantly to out-of-hospital cardiac arrest (OHCA) mortality.
Out-of-hospital cardiac arrest affects approximately 30,000 Australians annually, with an overall survival-to-discharge rate of approximately 10–12%. The Aus-ROC (Australasian Registry of Cardiac Arrest) consortium has demonstrated that VF/pulseless VT as initial rhythm occurs in approximately 20–25% of OHCA cases, and these patients have significantly better outcomes when bystander CPR and early defibrillation are provided.
Implantable cardioverter-defibrillator (ICD) therapy has transformed outcomes for patients at high risk of SCD. In Australia, approximately 5,000–6,000 ICDs are implanted annually, with increasing utilisation of cardiac resynchronisation therapy defibrillators (CRT-D). However, significant geographic variation in implantation rates exists, with lower rates in regional and remote areas.
Inherited arrhythmia syndromes, while less common, are increasingly recognised as important causes of SCD in young Australians. National genetic testing programmes and specialised inherited arrhythmia clinics in major cities (Royal Prince Alfred Hospital Sydney, Royal Melbourne Hospital, The Prince Charles Hospital Brisbane, Royal Adelaide Hospital) provide diagnostic and family screening services.
Sustained Monomorphic VT
Sustained monomorphic ventricular tachycardia (SMVT) is defined as VT lasting ≥30 seconds or requiring termination due to haemodynamic compromise. The QRS complex is uniform from beat to beat, reflecting a single re-entrant circuit or focal source. SMVT is the most common sustained ventricular tachyarrhythmia encountered in clinical practice and carries a significant risk of sudden cardiac death.
Structural Heart Disease Assessment
The evaluation of SMVT must systematically identify underlying structural heart disease, as the aetiology fundamentally determines prognosis and management strategy.
| Assessment Domain | Investigation | Key Findings | Australian Availability |
|---|---|---|---|
| Left ventricular function | Transthoracic echocardiography (TTE) | LVEF assessment, wall motion abnormalities, valvular disease | Available nationwide; MBS item 55120 |
| Myocardial scar/fibrosis | Cardiac MRI (CMR) with late gadolinium enhancement | Scar localisation, extent, and VT substrate characterisation | Major centres; MBS item 63400 series |
| Coronary disease | Coronary angiography or CT coronary angiogram | Exclude ischaemic aetiology, guide revascularisation | Angiography: all capital cities; CTA: MBS item 57360 |
| VT mechanism | Electrophysiology (EP) study | Inducibility, circuit mapping, ablation target identification | EP-capable centres in all capitals and select regional hospitals |
| Infiltrative/inflammatory | CMR, endomyocardial biopsy, genetic testing | Sarcoidosis, ARVC, amyloid, myocarditis | Referral to specialist centres |
Catheter Ablation
Catheter ablation has become a cornerstone of VT management, with evolving indications from last-resort to early-intervention therapy.
Key procedural considerations in the Australian context:
- Access: Electrophysiology and catheter ablation services are available in all Australian capital cities. Regional patients may require interstate transfer. Royal Flying Doctor Service (RFDS) facilitates transfers from remote areas.
- Techniques: Contemporary VT ablation utilises high-density mapping catheters (e.g., Advisor HD Grid, PentaRay), impedance-based electroanatomical mapping (CARTO 3, EnSite Precision), and integration with pre-procedural CMR/CT imaging.
- Complications: Major complication rate approximately 3–7% including cardiac perforation/tamponade (1–2%), vascular access complications, stroke (<1%), and death (<1%).
- Medicare rebates: MBS items for EP study (38220–38226) and ablation procedures; out-of-pocket costs may apply in private settings.
Antiarrhythmic Drug Therapy for Monomorphic VT
Polymorphic VT & Torsades de Pointes
Polymorphic ventricular tachycardia (PVT) is defined as VT with continuously varying QRS morphology, typically rotating around the baseline. Torsades de pointes (TdP) is a specific form of PVT occurring in the setting of QT prolongation (QTc >500 ms), characterised by the twisting of QRS complexes around the isoelectric line. The distinction between PVT with normal QT and TdP is critical, as management differs substantially.
QT Interval Assessment
Systematic QT interval assessment is essential in all patients presenting with polymorphic VT.
| QTc (Bazett) | Interpretation | Clinical Action |
|---|---|---|
| <440 ms (males) / <460 ms (females) | Normal | PVT managed as per structural heart disease pathway |
| 440–499 ms (males) / 460–499 ms (females) | Borderline prolongation | Review medications, electrolytes; serial ECGs; consider genetic testing |
| ≥500 ms | Significant prolongation | HIGH RISK of TdP — cease all QT-prolonging drugs, correct electrolytes, IV magnesium, continuous telemetry |
| ≥500 ms + syncope or TdP | Critical | Emergent management — MgSO₄, isoprenaline/temporary pacing if recurrent, genetic referral |
Drug-Induced Torsades de Pointes
Drug-induced TdP is the most common acquired cause and is preventable. Risk factors include female sex (2–3× risk), hypokalaemia, hypomagnesaemia, bradycardia, recent cardioversion, high drug concentrations, and congenital subclinical long QT.
Congenital Long QT Syndrome
Congenital long QT syndrome (LQTS) affects approximately 1 in 2,000 Australians and is caused by mutations in cardiac ion channel genes. Key subtypes:
| Subtype | Gene | Trigger | First-Line Therapy |
|---|---|---|---|
| LQT1 (30–35%) | KCNQ1 | Exercise (swimming), emotional stress | Beta-blockers (nadolol preferred); avoid competitive sport |
| LQT2 (25–30%) | KCNH2 (hERG) | Auditory stimuli (alarm clocks), emotional stress, QT-prolonging drugs | Beta-blockers; avoid QT drugs; supplement K⁺ |
| LQT3 (5–10%) | SCN5A | Rest/sleep, bradycardia | Beta-blockers + mexiletine; consider LCSD or ICD |
Left cardiac sympathetic denervation (LCSD) — thoracoscopic sympathectomy (T2–T4 ganglionectomy) — is available at selected Australian centres and is indicated for LQTS patients with recurrent syncope on maximal beta-blockade who refuse or are unsuitable for ICD implantation.
Magnesium Sulphate Therapy
Polymorphic VT with normal QT interval is most commonly associated with acute myocardial ischaemia and is managed with anti-ischaemic therapy (including emergency coronary angiography), beta-blockers, and amiodarone if ongoing. Lidocaine (lignocaine) 1–1.5 mg/kg IV is an alternative agent in ischaemia-related VT.
Ventricular Fibrillation
Ventricular fibrillation (VF) is a chaotic, disorganised ventricular rhythm that results in immediate loss of cardiac output and, without intervention, death within minutes. VF is the initial rhythm in approximately 20–25% of out-of-hospital cardiac arrests in Australia and is the most treatable cardiac arrest rhythm — survival rates of 30–50% are achievable with early defibrillation.
Cardiac Arrest Management (ANZCOR / ILCOR)
ICD Therapy for VF Survivors
All survivors of VF cardiac arrest without a clearly reversible cause (e.g., acute ST-elevation myocardial infarction with successful primary PCI and recovery of LVEF >50%) should undergo evaluation for ICD implantation as secondary prevention. Per NHFA/CSANZ guidelines, ICD is indicated when:
- VF arrest survivor with LVEF ≤50% after revascularisation and optimal medical therapy (≥4–6 weeks reassessment)
- Sustained VT causing haemodynamic compromise with LVEF ≤50%
- Unexplained syncope with inducible VT at EP study in the setting of structural heart disease
Targeted Temperature Management (TTM)
Targeted temperature management is recommended for all comatose patients following cardiac arrest with an initial shockable rhythm (VF/pulseless VT).
| Parameter | Recommendation |
|---|---|
| Target temperature | 32–36°C (constant target; ANZCOR/ILCOR 2020 — avoid active fever >37.7°C) |
| Duration | ≥24 hours of controlled temperature |
| Initiation | As soon as possible after ROSC (pre-hospital cooling with cold IV fluids no longer routinely recommended) |
| Methods | Surface cooling (Arctic Sun, blankets) or endovascular cooling catheter. Routine pre-hospital rapid infusion of cold fluids not recommended (TAME trial — no benefit with TTM at 33°C). |
| Monitoring | Continuous core temperature (oesophageal, bladder, or intravascular); avoid overshoot <31°C |
| Rewarming | Controlled at 0.25–0.5°C/hour; maintain normothermia (<37.7°C) for 72 h post-arrest |
| Australian availability | All tertiary ICUs; retrieval services (adult and paediatric) provide TTM during interhospital transfer |
ICD Therapy
Implantable cardioverter-defibrillators (ICDs) are the cornerstone of sudden cardiac death prevention in high-risk patients. In Australia, approximately 5,000–6,000 new ICDs and 1,500–2,000 replacement generators are implanted annually. Both transvenous (TV-ICD) and entirely subcutaneous (S-ICD) systems are available.
ICD Indications (NHFA/CSANZ)
| Indication | Criteria | Evidence Level |
|---|---|---|
| Primary prevention — ischaemic CMP | LVEF ≤35%, NYHA II–III, ≥40 days post-MI, ≥3 months optimal medical therapy (including GDMT and CRT where appropriate) | Class I (MADIT-II, SCD-HeFT) |
| Primary prevention — non-ischaemic CMP | LVEF ≤35%, NYHA II–III, ≥3 months optimal medical therapy including GDMT (ACEi/ARB/ARNi, beta-blocker, MRA, SGLT2i) | Class I (DANISH — NHFA concordant with Class I for specific patients) |
| Secondary prevention | Survived cardiac arrest (VF/pVT) without reversible cause; sustained VT with haemodynamic compromise and LVEF ≤50% | Class I (AVID, CIDS, CASH) |
| Inherited arrhythmia syndromes | High-risk Brugada, CPVT, ARVC, LQTS with cardiac arrest or recurrent syncope on beta-blockers | Class I–IIa depending on risk score |
ICD Programming
Contemporary ICD programming should minimise inappropriate therapies and reduce painful shocks. Evidence from MADIT-RIT, ADVANCE III, and PROVIDE trials supports the following principles:
- Single-zone programming (primary prevention): Monitor zone with ATP (anti-tachycardia pacing) before shock at ≥200 bpm (cycle length ≤300 ms). No therapy zone for rates <200 bpm.
- Dual-zone programming: VT zone 170–200 bpm (ATP × 8 bursts → shock); VF zone >200 bpm (ATP during charging → shock at 36 J if ATP fails).
- Detection duration: Prolong detection to 30/40 intervals (or ≥6–12 seconds) to allow self-termination before therapy delivery.
- ATP before shocks: Burst ATP (8 pulses at 88% of VT cycle length) is effective for VT up to 200 bpm and should be delivered even in the VF zone during capacitor charging.
- S-ICD programming: Subcutaneous ICD cannot deliver ATP; uses a conditional zone (typically 200–250 bpm with morphology discrimination) to reduce inappropriate shocks.
Appropriate vs Inappropriate Shocks
| Type | Aetiology | Management |
|---|---|---|
| Appropriate shock | True VT/VF detected and treated correctly | Optimise antiarrhythmic therapy, consider catheter ablation, reassess programming |
| Inappropriate shock — SVT | Atrial fibrillation, atrial flutter, AVNRT, sinus tachycardia | Rate control, SVT ablation, reprogram discriminators (sudden onset, stability, morphology) |
| Inappropriate shock — T-wave oversensing | Tall T-waves detected as R-waves (double-counting) | Reprogram sensitivity; adjust sensing vector (S-ICD); correct hyperkalaemia |
| Inappropriate shock — lead fracture/noise | Lead insulation breach, connector problem | Lead revision or replacement; impedance monitoring on remote follow-up |
Electrical Storm Management
Electrical storm (arrhythmic storm) is defined as ≥3 episodes of VT/VF within 24 hours, each requiring intervention. It carries a mortality rate of 15–25% in-hospital and requires emergent, multidisciplinary management.
Remote Monitoring
Remote monitoring of ICDs and CRT-D devices is the standard of care in Australia, enabling early detection of device alerts, arrhythmias, and heart failure decompensation.
- Platforms available in Australia: Medtronic CareLink™, Abbott Merlin.net™, Boston Scientific Latitude™, Biotronik Home Monitoring™.
- Frequency: Daily automatic transmissions for alerts; routine follow-up every 3–6 months remote, with in-clinic review every 6–12 months.
- Benefits: Reduced time to clinical action for atrial fibrillation detection, lead alerts, battery depletion, and heart failure parameters. IN-TIME trial showed mortality benefit with remote monitoring.
- Regional and remote access: Remote monitoring is particularly valuable for patients in regional and remote Australia. Mobile phone coverage and satellite connectivity in remote NT, WA, and QLD may require alternative transmission methods — contact device manufacturer for solutions.
- Medicare: MBS items for remote monitoring (MBS items 55124, 55125 for device interrogation); some private health funds cover additional telehealth consultations.
Inherited Arrhythmia Syndromes
Inherited arrhythmia syndromes (also known as channelopathies or primary electrical diseases) are genetic conditions that predispose to ventricular tachyarrhythmias and sudden cardiac death, typically in the setting of a structurally normal or minimally abnormal heart. They are increasingly recognised as important causes of SCD in young Australians, often presenting as sudden infant death syndrome (SIDS), unexplained drowning, sudden unexpected death in epilepsy (SUDEP), or death during exercise.
Brugada Syndrome
Brugada syndrome is characterised by distinctive ST-segment elevation in the right precordial leads (V1–V3) with risk of VF and SCD, predominantly in males aged 20–50 years. It is caused primarily by loss-of-function mutations in SCN5A (sodium channel), though the genetic basis is identifiable in only 20–30% of cases.
| Feature | Detail |
|---|---|
| ECG pattern | Type 1 (coved) ST elevation ≥2 mm in V1–V3 followed by negative T-wave — spontaneous or provoked by sodium channel blocker (ajmaline/flecainide test) |
| Prevalence | Estimated 1:2,000–1:5,000; higher in Southeast Asian populations; variable in Australian population |
| Risk factors for events | Spontaneous Type 1 pattern, history of syncope, male sex, SCN5A-positive mutation, fever |
| Provocation test | Ajmaline (1 mg/kg IV over 10 min) — available at major Australian EP centres via TGA Special Access Scheme. Flecainide 2 mg/kg IV (max 150 mg) is an alternative. |
| Management | ICD for cardiac arrest survivors and high-risk patients (syncope with spontaneous Type 1). Avoid fever (aggressive antipyretics). Avoid alcohol excess, large meals, QT-prolonging drugs. Isoproterenol for electrical storm. Quinidine (oral) for recurrent VF/ICD storms. |
| Australian clinics | Inherited arrhythmia clinics at Royal Prince Alfred (Sydney), Royal Melbourne, Prince Charles Hospital (Brisbane), Royal Adelaide, Royal Perth |
Catecholaminergic Polymorphic VT (CPVT)
CPVT is a highly malignant inherited arrhythmia syndrome characterised by exercise- or emotion-triggered bidirectional or polymorphic VT, typically presenting in childhood or adolescence with a structurally normal heart and normal resting ECG. It is caused by mutations in RYR2 (ryanodine receptor — autosomal dominant, ~60% of cases) or CASQ2 (calsequestrin — autosomal recessive).
Arrhythmogenic Right Ventricular Cardiomyopathy (ARVC)
ARVC (also termed arrhythmogenic cardiomyopathy, ACM) is a genetic cardiomyopathy characterised by fibro-fatty replacement of the myocardium — predominantly the right ventricle but increasingly recognised with biventricular or left-dominant forms. It is an important cause of SCD in young athletes and is caused by mutations in desmosomal genes (PKP2, DSP, DSG2, DSC2, JUP).
| Diagnostic Category | Criteria (2010 Task Force / 2020 Padua Criteria) |
|---|---|
| Definite diagnosis | 2 major, OR 1 major + 2 minor, OR 4 minor from different categories |
| Borderline | 1 major + 1 minor, OR 3 minor |
| Possible | 1 major OR 2 minor |
Diagnostic domains include: (1) Global/regional dysfunction and structural alterations (echo, CMR); (2) Tissue characterisation (endomyocardial biopsy — fibrofatty replacement); (3) Depolarisation/conduction abnormalities (epsilon waves, terminal QRS duration ≥55 ms in V1–V3); (4) Repolarisation abnormalities (T-wave inversion V1–V3 in adults >14 years); (5) Arrhythmias (non-sustained VT with LBBB morphology, >500 PVCs/24 h); (6) Family history (confirmed ARVC or SCD with ARVC at autopsy).
Management of ARVC:
- Exercise restriction: Avoid competitive sport and high-intensity endurance exercise. Exercise accelerates disease progression and arrhythmia risk.
- Pharmacotherapy: Beta-blockers (sotalol or nadolol), antiarrhythmic drugs (sotalol preferred, amiodarone for refractory cases).
- Catheter ablation: For recurrent VT despite medical therapy. Epicardial approach frequently required (available at major Australian EP centres). Substrate-based ablation. Recurrence rates are higher than in ischaemic VT.
- ICD: For cardiac arrest survivors, sustained VT, haemodynamically tolerated VT, and progressive RV/LV dysfunction. Primary prevention ICD in high-risk patients (significant ventricular dysfunction, syncope, non-sustained VT).
- Heart transplantation: For refractory heart failure or arrhythmias unresponsive to all therapies. Refer to transplant centres (St Vincent's Sydney, Alfred Melbourne, Prince Charles Brisbane).
Investigations
Risk Stratification & Severity Scoring
Risk stratification for ventricular arrhythmias and SCD is essential for guiding ICD implantation decisions, activity restrictions, and follow-up intensity. The approach varies by underlying substrate.
Ischaemic Cardiomyopathy — SCD Risk Stratification
Inherited Arrhythmia — Risk Stratification Tools
| Condition | Risk Score / Tool | High-Risk Features |
|---|---|---|
| LQTS | Schwartz score (clinical); LQT1/2/3 genotype | QTc >500 ms, syncope on therapy, LQT3, infancy events, male LQT2 |
| Brugada | Shanghai score (2016) | Spontaneous Type 1 ECG, history of syncope, VF, male sex, SCN5A + |
| CPVT | Clinical (genotype, exercise test response) | Prior cardiac arrest, syncope on beta-blockers, supraventricular arrhythmias, young age at diagnosis |
| ARVC | Risk factors (no validated score) | Prior sustained VT/VF, significant RV dilation, LV involvement, male sex, compound desmosomal mutations, competitive sport history |
Monitoring
Ongoing monitoring is essential for patients with ventricular tachyarrhythmias, encompassing arrhythmia surveillance, medication safety, device function, and psychosocial wellbeing.
| Monitoring Domain | Frequency | Tests / Assessments |
|---|---|---|
| ECG monitoring | Every visit (3–6 monthly); continuous after drug initiation | 12-lead ECG (QTc, QRS duration, HR, arrhythmia recurrence); Holter/loop recorder for symptom correlation |
| Amiodarone toxicity | TFTs every 6 months; LFTs, PFTs annually; ophthalmology annually; chest X-ray at baseline and annually | TSH, fT4, fT3; ALT, AST, GGT; DLCO; slit-lamp examination |
| Sotalol monitoring | After every dose change; then every 6 months | ECG (QTc <500 ms), renal function, electrolytes |
| ICD device follow-up | Remote: daily transmissions (alerts), routine 3–6 monthly. In-clinic: every 6–12 months | Battery status, lead impedance, sensing thresholds, arrhythmia episodes, shock/ATP appropriateness, heart failure diagnostics |
| LVEF reassessment | 3–6 monthly until stable; then annually | TTE — guide medical therapy optimisation and CRT/ICD decisions |
| Genetic/family screening | At diagnosis and when new family members identified | Cascade genetic testing; clinical screening (ECG, exercise test, echo) for genotype-positive/phenotype-negative family members |
| Psychological wellbeing | Every visit — validated screening | PHQ-9 (depression), GAD-7 (anxiety), ICD-specific anxiety scales. Referral to cardiac psychology. SADS Australia support groups. |
Special Populations
Aboriginal and Torres Strait Islander Health Considerations
Aboriginal and Torres Strait Islander peoples experience significantly higher rates of cardiovascular disease, sudden cardiac death, and ventricular tachyarrhythmias compared to non-Indigenous Australians. Rheumatic heart disease (RHD), cardiomyopathy, and ischaemic heart disease are major contributors to this disparity.
📚 References
- 1. Priori SG, Blomström-Lundqvist C, Mazzanti A, et al. 2015 ESC Guidelines for the management of patients with ventricular arrhythmias and the prevention of sudden cardiac death. Europace. 2015;17(11):1601–1687.
- 2. Cronin EM, Bogun FM, Buxton AE, et al. 2019 HRS/EHRA/APHRS/LAHRS expert consensus statement on catheter ablation of ventricular arrhythmias. Heart Rhythm. 2020;17(1):e2–e154.
- 3. Al-Khatib SM, Stevenson WG, Ackerman MJ, et al. 2017 AHA/ACC/HRS guideline for management of patients with ventricular arrhythmias and the prevention of sudden cardiac death. J Am Coll Cardiol. 2018;72(14):e91–e220.
- 4. Australasian Resuscitation Council (ANZCOR). ANZCOR Guideline 11.2 – Protocols for Adult Advanced Life Support. ANZCOR. Updated 2021.
- 5. Nehme Z, Andrew E, Bernard S, et al. The Aus-ROC Australian and New Zealand out-of-hospital cardiac arrest Epistry. Emergency Medicine Australasia. 2021;33(3):461–468.
- 6. National Heart Foundation of Australia and Cardiac Society of Australia and New Zealand (NHFA/CSANZ). Guidelines for the prevention, detection, and management of heart failure in Australia. Heart Lung Circ. 2018;27(10):1123–1208.
- 7. Connolly SJ, Dorian P, Roberts RS, et al. Comparison of beta-blockers, amiodarone plus beta-blockers, or sotalol for prevention of shocks from implantable cardioverter defibrillators: the OPTIC Study — a randomized trial. JAMA. 2006;295(2):165–171.
- 8. Kusumoto FM, Bailey KR, Chaouki AS, et al. Systematic review for the 2017 AHA/ACC/HRS guideline for management of patients with ventricular arrhythmias and prevention of sudden cardiac death. Heart Rhythm. 2018;15(10):e250–e264.
- 9. Schwartz PJ, Ackerman MJ, George AL, Wilde AAM. Impact of genetics on the clinical management of channelopathies. J Am Coll Cardiol. 2013;62(3):169–180.
- 10. Corrado D, Wichter T, Link MS, et al. Treatment of arrhythmogenic right ventricular cardiomyopathy/dysplasia: an international task force consensus statement. European Heart Journal. 2015;36(46):3227–3237.
- 11. van der Werf C, Kannankeril PJ, Sacher F, et al. Flecainide therapy reduces exercise-induced ventricular arrhythmias in patients with catecholaminergic polymorphic ventricular tachycardia. J Am Coll Cardiol. 2011;57(22):2244–2254.
- 12. Dankner R, Shahar A, Novikov I, et al. MADIT-RIT — Inappropriate ICD therapy reduction with high-rate therapy and delayed ICD therapy. N Engl J Med. 2012;367(24):2275–2283.
- 13. Australian Institute of Health and Welfare (AIHW). Cardiovascular disease in Aboriginal and Torres Strait Islander people. AIHW Cat. No. CVD 87. Canberra: AIHW; 2023.
- 14. RHDAustralia (ARF/RHD writing group). The 2020 Australian guideline for prevention, diagnosis, and management of acute rheumatic fever and rheumatic heart disease (3rd edition). Menzies School of Health Research; 2020.
- 15. Austroads. Assessing Fitness to Drive — Medical Standards for Licensing and Clinical Management Guidelines. Sydney: Austroads; 2022.
- 16. Køber L, Thune JJ, Nielsen JC, et al. Defibrillator implantation in patients with nonischemic systolic heart failure. N Engl J Med. 2016;375(13):1221–1230.
- 17. Kirchhof P, Sipido KR, Cowie MR, et al. The continuum of personalized cardiovascular medicine: a position paper of the European Society of Cardiology. European Heart Journal. 2014;35(46):3250–3257.
- 18. Cosío FG, Aliot E, Botto GL, et al. Delayed rhythm control for atrial fibrillation may be a cause of harm: the EARLY-AF study. European Heart Journal. 2022;43(25):2379–2390.
- 19. Derval N, Simpson CS, Birnie DH, et al. Prevalence and characteristics of early repolarization in the CASPER registry. J Am Coll Cardiol. 2011;58(7):722–728.
- 20. Neumar RW, Shuster M, Callaway CW, et al. Part 1: Executive summary: 2015 American Heart Association guidelines update for cardiopulmonary resuscitation and emergency cardiovascular care. Circulation. 2015;132(18 Suppl 2):S315–S367.