📋 Key Information Summary
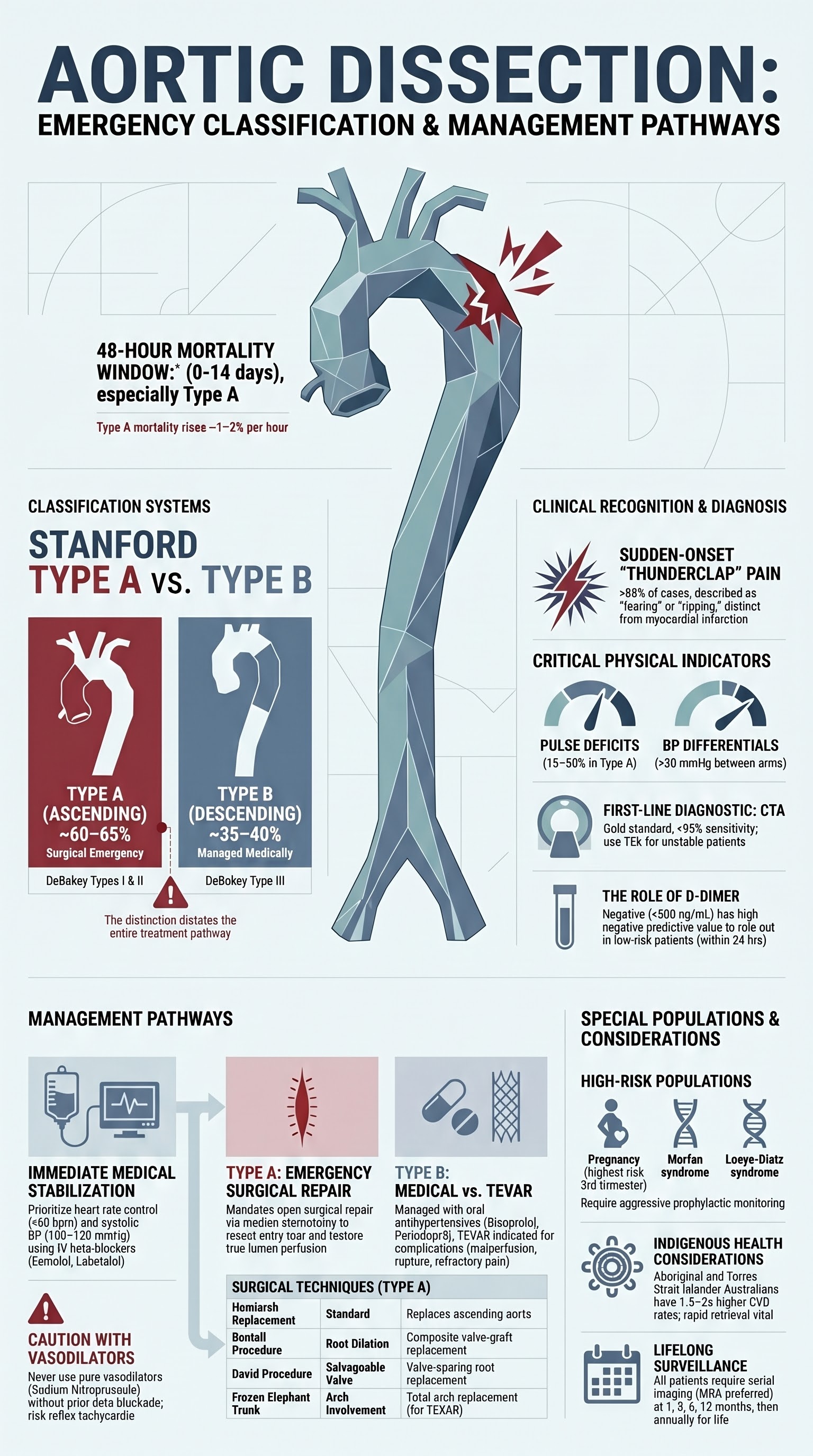
- Aortic dissection is the most common acute aortic syndrome, with an incidence of approximately 3–4 per 100,000 person-years in Australia; mortality rises ~1–2% per hour if untreated in Type A.
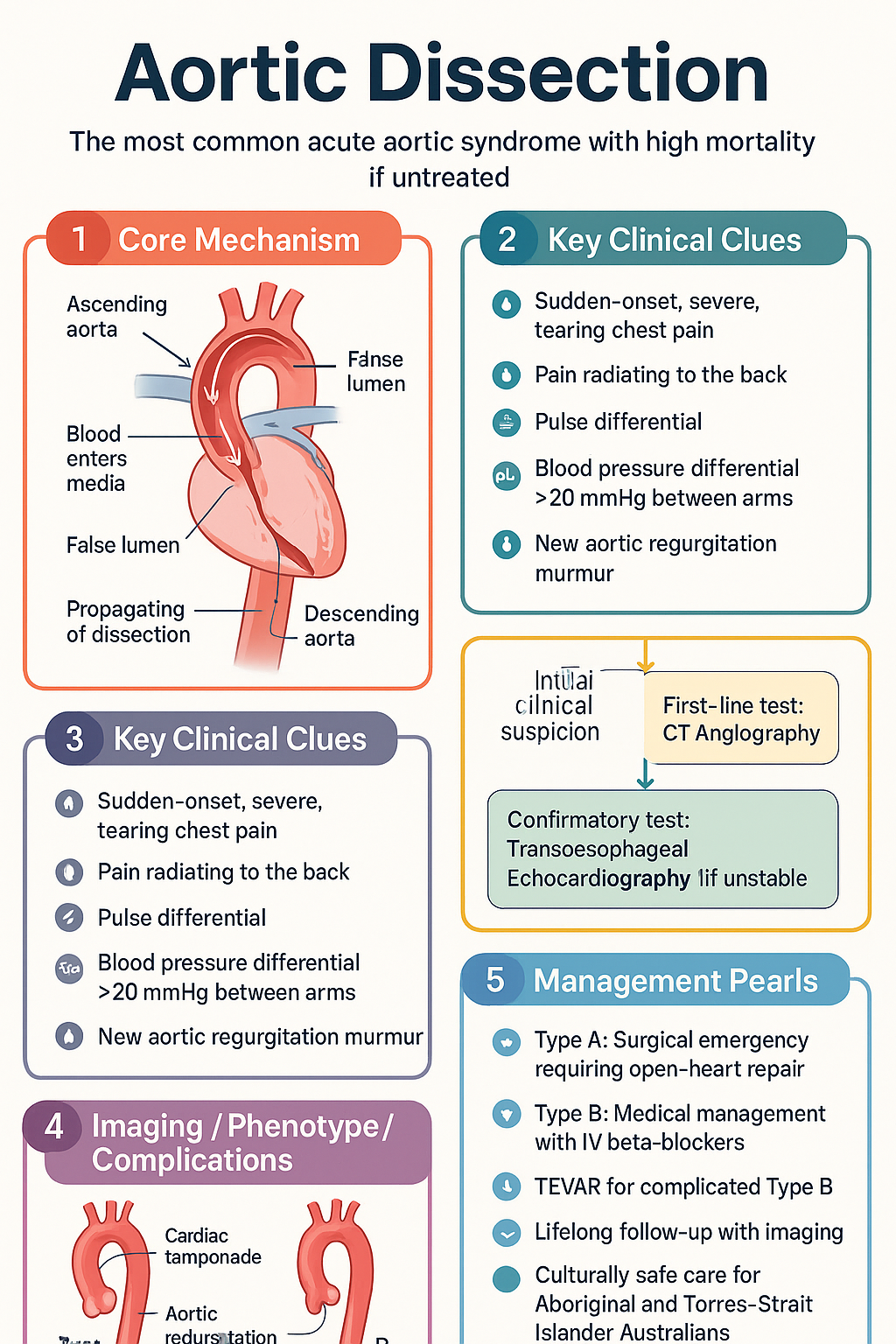
- Stanford classification divides dissections into Type A (involving the ascending aorta) and Type B (distal to the left subclavian artery); DeBakey types I, II, and III provide further anatomical detail.
- Type A dissection is a surgical emergency — all confirmed cases require emergent open-heart repair at a cardiothoracic centre.
- Type B dissection is managed medically in the first instance with strict heart rate (<60 bpm) and systolic BP (<120 mmHg) targets using IV beta-blockers (esmolol, labetalol).
- CT angiography of the entire aorta is the first-line diagnostic investigation (sensitivity and specificity >95%); D-dimer has a high negative predictive value and can assist in ruling out dissection in low-risk patients.
- Classic presentation is sudden-onset, severe, tearing chest pain radiating to the back, but presentations vary widely; always consider dissection in patients with acute chest pain and neurological deficits, pulse differentials, or new aortic regurgitation.
- Pain character and location help differentiate Type A (anterior chest) from Type B (interscapular, back, abdomen).
- Complications include cardiac tamponade, aortic regurgitation, malperfusion syndromes (stroke, mesenteric ischaemia, limb ischaemia), and rupture.
- TEVAR (thoracic endovascular aortic repair) is indicated for complicated Type B dissections — malperfusion, rupture, refractory pain, or rapid aortic expansion.
- Lifelong follow-up with serial cross-sectional imaging (CT or MRA) is essential for both Type A (post-surgical) and Type B patients to detect aneurysmal degeneration and late complications.
- Aboriginal and Torres Strait Islander Australians have higher rates of cardiovascular disease and may present later; culturally safe care and access to tertiary centres are critical considerations.
Classification Systems
Accurate classification of aortic dissection guides immediate management decisions and determines whether surgical or medical therapy is appropriate. Two complementary classification systems are used in clinical practice: the Stanford and DeBakey systems.
Stanford Classification
The Stanford system is the most widely used in contemporary practice and is directly linked to management pathways. It divides dissections based on whether the ascending aorta is involved.
| Type | Involvement | Approximate Frequency | Management |
|---|---|---|---|
| Stanford Type A | Ascending aorta (with or without descending involvement); any dissection involving the ascending aorta | ~60–65% | Surgical emergency |
| Stanford Type B | Descending aorta only — origin distal to the left subclavian artery | ~35–40% | Medical management ± TEVAR |
DeBakey Classification
The DeBakey system provides finer anatomical granularity and is often cited alongside the Stanford system in surgical literature.
| Type | Anatomy | Stanford Equivalent |
|---|---|---|
| DeBakey I | Originates in the ascending aorta, extends to the aortic arch and beyond (descending aorta) | Type A |
| DeBakey II | Confined to the ascending aorta only | Type A |
| DeBakey III | Originates distal to the left subclavian artery (IIIa: limited to descending; IIIb: extends below diaphragm) | Type B |
Timing Classification
The temporal classification is critical for prognosis, as operative risk and mortality differ significantly by timing of presentation.
Clinical Presentation
Aortic dissection is often called "the great masquerader" because of its protean manifestations. A high index of clinical suspicion is essential, particularly in patients presenting with acute chest pain and any high-risk features.
Pain Characteristics
Pain is the presenting symptom in >85% of cases. Its character and location provide important diagnostic clues:
- Onset: Sudden, maximal intensity at onset ("thunderclap") — this distinguishes dissection from myocardial infarction, where pain typically crescendos over minutes to hours.
- Character: Classically described as tearing or ripping; may also be sharp, stabbing, or pressure-like.
- Type A location: Anterior chest pain, often radiating to the neck, jaw, or arms. May mimic acute coronary syndrome.
- Type B location: Interscapular back pain, often radiating to the abdomen, flank, or lower extremities.
- Migrating pain: Pain that migrates distally along the path of dissection propagation is highly suggestive but present in only ~15–20% of cases.
Physical Examination Findings
A systematic cardiovascular examination is critical and may reveal:
| Finding | Mechanism | Significance |
|---|---|---|
| Pulse deficit | Dissection flap occluding branch vessel origin | Present in 15–30% of Type A; associated with malperfusion and worse prognosis |
| Blood pressure differential (>20 mmHg between arms) | Involvement of the brachiocephalic or left subclavian artery | Highly specific for dissection when present; measure in both arms |
| Wide mediastinum (CXR) | Enlarged aorta or haematoma | Suggestive but not diagnostic; normal CXR does not exclude dissection |
| New diastolic murmur | Aortic regurgitation from Type A dissection distorting the aortic root | Present in 30–50% of Type A; indicates need for concomitant valve surgery |
| Cardiac tamponade | Rupture of the ascending aorta into the pericardial space | Major cause of early death in Type A; Beck's triad (hypotension, muffled heart sounds, JVD) |
| Neurological deficits | Carotid artery malperfusion (stroke); spinal cord ischaemia | Stroke in ~5–10% of Type A; paraplegia in ~2–5% of Type B |
| Malperfusion syndromes | Branch vessel obstruction by false lumen expansion | Mesenteric (abdominal pain, lactic acidosis), renal (anuria, acute kidney injury), limb (ischaemia) |
Complications by Type
- Cardiac tamponade (leading cause of death)
- Acute aortic regurgitation (30–50%)
- Acute coronary syndrome (right coronary ostium most common)
- Stroke / transient ischaemic attack
- Superior vena cava obstruction
- Aortic rupture (into pleural space or mediastinum)
- Mesenteric ischaemia (high mortality)
- Renal ischaemia / acute kidney injury
- Lower limb ischaemia
- Spinal cord ischaemia / paraplegia
- Aortic rupture
- Aneurysmal degeneration (late)
Diagnostic Imaging
Rapid and accurate diagnostic imaging is the cornerstone of aortic dissection management. The choice of modality depends on patient stability, local availability, and the clinical question.
Imaging Modalities
- Sensitivity: 95–100%; Specificity: 95–100%
- Fast, widely available in Australian EDs 24/7
- Provides complete aortic assessment from arch to bifurcation — identifies entry tear, false lumen, branch vessel involvement, and pericardial effusion
- MBS Item 57354 (CT aorta — thoracic) and 57355 (abdominal) — Medicare-rebatable
- Limitation: IV contrast (renal impairment), radiation exposure; not suitable for unstable patients who cannot be transported to CT
- Sensitivity: 98–99%; Specificity: 95–97% for Type A
- Can be performed at the bedside in the ICU — ideal for haemodynamically unstable patients
- Excellent for identifying aortic regurgitation, pericardial effusion, and proximal (Type A) dissection
- Limitation: Operator-dependent; limited views of the distal ascending aorta and proximal arch (blind spot); not reliable for Type B dissection involving the distal aorta
- Requires sedation/intubation — not always feasible in unstable patients
- Sensitivity: 98–100%; Specificity: 98–100%
- Gold-standard for chronic dissection surveillance — no radiation, excellent soft-tissue contrast
- NOT suitable for acute diagnosis — scan time is long (30–60 min), limited availability out-of-hours, and many patients cannot tolerate prolonged scanning
- MBS Item 63501 (MRA thoracic aorta) — available at major tertiary centres
- Contraindicated with certain metallic implants (pacemakers, older sternal wires); requires screening
- Rapid bedside assessment — can identify pericardial effusion, aortic regurgitation, and proximal ascending aorta dilation
- Sensitivity for dissection flap: Only 60–70% (limited acoustic windows)
- A normal TTE does NOT exclude aortic dissection
- Useful as an initial screening tool in the resuscitation bay while arranging definitive CTA
Role of D-dimer
D-dimer (fibrin degradation product) is elevated in >95% of acute aortic dissections. A negative D-dimer (<500 ng/mL using standard assay) has a high negative predictive value (~95–98%) and may be used to help rule out dissection in low-risk patients presenting within 24 hours of symptom onset.
Important caveats:
- D-dimer should NOT be used as a standalone test to exclude dissection — it must be interpreted in the context of clinical pre-test probability.
- D-dimer is non-specific — elevated in PE, MI, sepsis, malignancy, surgery, pregnancy, and many other conditions.
- Sensitivity decreases with chronic dissection and with presentation >24 hours after onset.
- A positive D-dimer in a patient with chest pain should prompt urgent cross-sectional imaging, not further D-dimer serial testing.
Diagnostic Algorithm
Type A Management — Emergency Surgical Repair
Immediate Medical Stabilisation
While arranging emergency surgical transfer, aggressive medical management to reduce aortic wall stress must be initiated simultaneously. The dual goals are heart rate control (<60 bpm) and systolic blood pressure reduction (100–120 mmHg), achieved primarily with IV beta-blockers.
Emergency Surgical Repair
The definitive treatment for Type A dissection is open surgical repair, performed via median sternotomy with cardiopulmonary bypass and often hypothermic circulatory arrest. The goals of surgery are to resect the primary entry tear and restore true lumen perfusion.
Surgical Techniques
| Procedure | Indication | Description |
|---|---|---|
| Ascending aortic replacement (hemiarch) | Most Type A dissections — standard operation | Replace ascending aorta with a Dacron graft; open distal anastomosis during hypothermic circulatory arrest (18–28°C); reimplant coronary buttons |
| Root replacement (Bentall procedure) | Aortic root dilation or severe aortic regurgitation | Composite valve-graft replacement of the aortic root; mechanical or bioprosthetic valve |
| Valve-sparing root replacement (David procedure) | Aortic regurgitation with salvageable native valve (young patients) | Reimplant the native aortic valve into a Dacron graft — avoids lifelong anticoagulation |
| Total arch replacement ± frozen elephant trunk | Arch involvement, DeBakey I with extensive arch tear | Replace the aortic arch with a branched graft; frozen elephant trunk provides a landing zone for future TEVAR if needed |
Surgical Outcomes (Australian and International Data)
- Operative mortality: 15–25% at 30 days in high-volume centres (lower in experienced aortic centres); up to 30–40% in patients presenting with pre-operative malperfusion or tamponade.
- Australian centres: Major aortic surgery is concentrated in tertiary hospitals in capital cities (Royal Prince Alfred, Royal Melbourne, Alfred Hospital, St Vincent's Sydney, Princess Alexandra Brisbane, Royal Adelaide). Transfer protocols exist via state retrieval services (e.g., NSW Health Critical Care, Ambulance Victoria MICA).
- 5-year survival: 70–85% after successful Type A repair in contemporary series.
- Reintervention rate: 10–20% at 10 years — often for residual arch or descending aortic disease requiring TEVAR.
Special Considerations in Type A
Malperfusion syndrome in Type A: Up to 30% of Type A dissections present with malperfusion (coronary, cerebral, mesenteric, renal, or limb). Some centres advocate a "stent-first" approach — TEVAR to restore branch vessel perfusion followed by open ascending repair — though evidence is evolving.
Stroke with Type A: Patients with pre-operative stroke have higher surgical mortality but should generally still proceed to surgery. The stroke is often worsened by untreated dissection rather than by surgery itself. Decisions should be made in conjunction with neurology and neurosurgery.
Tamponade: Pericardiocentesis is generally contraindicated in Type A dissection with tamponade — decompression may worsen bleeding by relieving tamponade physiology. Emergency surgical repair is definitive treatment. Use cautious volume resuscitation and vasopressors as a bridge.
Type B Management
Type B aortic dissection (distal to the left subclavian artery) is managed differently from Type A. The initial approach is medical management with aggressive antihypertensive and heart rate control. Endovascular or open surgical intervention is reserved for complicated presentations.
Uncomplicated Type B — Medical Management
IV Antihypertensive Agents for Acute Type B
Transition to Oral Medications
Once the patient is stabilised (typically 24–48 hours), transition to oral long-acting agents for lifelong blood pressure control:
Complicated Type B — Indications for TEVAR
Thoracic endovascular aortic repair (TEVAR) has transformed the management of complicated Type B dissection. It involves deployment of a covered stent-graft across the primary entry tear to redirect flow into the true lumen and promote false lumen thrombosis.
- Malperfusion syndrome: Mesenteric, renal, spinal cord, or lower limb ischaemia
- Aortic rupture: Contained (periaortic haematoma) or free rupture
- Refractory pain: Ongoing severe pain despite optimal medical therapy — suggests impending rupture or expansion
- Rapid aortic expansion: Increase in aortic diameter ≥5 mm during the index admission
- Periaortic haematoma: CT evidence of contained leak
TEVAR Procedure
- Performed via femoral artery access (percutaneous or cutdown) under general anaesthesia in a hybrid operating theatre.
- A covered stent-graft (e.g., Gore TAG®, Medtronic Valiant Captivia®) is deployed across the primary entry tear, typically covering the left subclavian artery origin if necessary.
- Left subclavian artery coverage may require prior or concurrent revascularisation (carotid-subclavian bypass or chimney stent) if there is a patent left internal mammary artery graft or vertebrobasilar insufficiency.
- Australian availability: TEVAR is available at major tertiary vascular/ cardiothoracic centres in all Australian state capitals. Case volume and outcomes are reported through the Australasian Vascular Audit (AVA).
TEVAR Outcomes
- 30-day mortality for TEVAR in complicated Type B: 10–15% (compared with 30–40% for open surgical repair).
- Spinal cord ischaemia risk: 3–5% — mitigated by cerebrospinal fluid drainage in high-risk cases.
- False lumen thrombosis achieved in 70–90% at 1 year.
- Reintervention rate: 10–30% at 5 years — most commonly for endoleak or distal stent-induced new entry tears.
Routine Surveillance for Uncomplicated Type B
All patients with Type B dissection — whether managed medically or with TEVAR — require lifelong surveillance for aneurysmal degeneration of the false lumen.
Special Populations
Pregnancy
- Aortic dissection risk is highest in the third trimester and early postpartum period due to haemodynamic changes and hormonal effects on vascular connective tissue.
- Patients with Marfan syndrome, Loeys-Dietz syndrome, or bicuspid aortic valve are at particularly elevated risk.
- Diagnosis: CTA involves ionising radiation but should NOT be delayed — the risk of missed dissection outweighs fetal radiation risk. TEE is a reasonable alternative. MRA without gadolinium is the preferred follow-up modality.
- Type A in pregnancy: Emergency surgery is indicated regardless of gestational age. Caesarean section may be performed immediately before or concurrently with aortic repair if the fetus is viable (≥28 weeks).
- Type B in pregnancy: Medical management as per non-pregnant patients. Labetalol is the preferred beta-blocker in pregnancy. Avoid ACE inhibitors and ARBs (teratogenic). Avoid atenolol (fetal growth restriction concerns). Nitroprusside is contraindicated (fetal cyanide toxicity).
- Multidisciplinary team: cardiothoracic surgery, obstetrics, neonatology, anaesthesia, and cardiology.
Paediatrics
- Aortic dissection in children is rare and almost always associated with underlying conditions: Marfan syndrome, Turner syndrome, Ehlers-Danlos syndrome, bicuspid aortic valve, or prior cardiac surgery.
- Diagnosis is often delayed due to low clinical suspicion — maintain a high index in children with connective tissue disorders presenting with acute chest pain.
- Management principles mirror adults: Type A → emergency surgery; Type B → medical management with TEVAR reserved for complicated cases.
- Beta-blocker doses should be weight-adjusted. Esmolol 100–500 µg/kg/min infusion. Labetalol 0.2–1 mg/kg/hr IV.
- Referral to a paediatric cardiothoracic centre is mandatory. In Australia: Royal Children's Hospital Melbourne, Children's Hospital Westmead, Queensland Children's Hospital.
Elderly
- Patients >70 years have significantly higher operative mortality for Type A repair (30–50% vs 15–20% in younger patients). However, conservative management carries near-universal mortality — surgery should still be offered unless significant comorbidities preclude survival.
- TEVAR for complicated Type B may be preferred over open repair in the elderly due to lower perioperative morbidity.
- Beta-blocker therapy: start at lower doses; increased risk of bradycardia and hypotension. Renally adjust all medications.
- Consider frailty assessment, advance care planning, and goals-of-care discussions as part of shared decision-making.
Renal Impairment
- Contrast-induced nephropathy is a significant risk with CTA. Use low-osmolar contrast, pre-hydrate with IV normal saline (1 mL/kg/hr for 6–12 h pre- and post-scan), and minimise contrast volume.
- MRA (without gadolinium) is preferred for follow-up imaging in CKD.
- Sodium nitroprusside: risk of thiocyanate accumulation with prolonged use in CKD — monitor levels; prefer esmolol (renally independent metabolism).
- Malperfusion of the renal arteries from the dissection itself may cause acute kidney injury — this is an indication for intervention (TEVAR or renal artery stenting).
Hepatic Impairment
- Labetalol: use with caution in severe hepatic impairment — reduced first-pass metabolism and risk of hypotension. Reduce dose and monitor closely.
- Sodium nitroprusside: metabolised to cyanide then thiocyanate — impaired hepatic cyanide metabolism increases toxicity risk. Avoid in severe liver disease.
- Esmolol (metabolised by RBC esterases) is preferred in hepatic impairment.
- Coagulopathy from liver disease increases surgical bleeding risk — optimise coagulation pre-operatively with FFP, cryoprecipitate, and platelets as indicated.
Connective Tissue Disorders
- Marfan syndrome: Highest lifetime risk of dissection. Prophylactic aortic root replacement recommended when diameter ≥45 mm (with risk factors) or ≥50 mm. Lifelong beta-blockade or losartan (emerging evidence for TGF-β inhibition).
- Loeys-Dietz syndrome: Aggressive aortopathy — dissection at smaller diameters. Prophylactic surgery at ≥40–42 mm depending on variant.
- Vascular Ehlers-Danlos syndrome (type IV): High surgical morbidity due to tissue fragility. Celiprolol (not PBS-listed in Australia) has evidence for reducing vascular events. TEVAR may be considered but vessel access complications are common.
- Turner syndrome: Bicuspid aortic valve and aortic dilation are common — regular imaging surveillance from adolescence.
- Genetic aortopathy screening: first-degree relatives of patients with non-traumatic Type A dissection should be offered screening (aortic imaging ± genetic testing).
Aboriginal and Torres Strait Islander Health Considerations
📚 References
- 1. Nienaber CA, Clough RE. Management of acute aortic dissection. Lancet. 2015;385(9970):800–811. doi:10.1016/S0140-6736(14)61005-9
- 2. Erbel R, Aboyans V, Boileau C, et al. 2014 ESC Guidelines on the diagnosis and treatment of aortic diseases. Eur Heart J. 2014;35(41):2873–2926. doi:10.1093/eurheartj/ehu281
- 3. Hiratzka LF, Bakris GL, Beckman JA, et al. 2010 ACCF/AHA/AATS/ACR/ASA/SCA/SCAI/SIR/STS/SVM guidelines for the diagnosis and management of patients with thoracic aortic disease. Circulation. 2010;121(13):e266–e369. doi:10.1161/CIR.0b013e3181d4739e
- 4. Mussa FF, Horton JD, Moridzadeh R, et al. Acute aortic dissection and intramural hematoma: a systematic review. JAMA. 2016;316(7):754–763. doi:10.1001/jama.2016.10026
- 5. Pape LA, Awais M, Woznicki EM, et al. Presentation, diagnosis, and outcomes of acute aortic dissection: 17-year trends from the International Registry of Acute Aortic Dissection. J Am Coll Cardiol. 2015;66(4):350–358. doi:10.1016/j.jacc.2015.05.029
- 6. Nienaber CA, Rousseau H, Eggebrecht H, et al. Randomized comparison of strategies for type B aortic dissection: the Investigation of Stent Grafts in Aortic Dissection (INSTEAD) trial. Circulation. 2009;120(25):2519–2528. doi:10.1161/CIRCULATIONAHA.109.886523
- 7. Fattori R, Cao P, De Rango P, et al. Interdisciplinary expert consensus document on management of type B aortic dissection. J Am Coll Cardiol. 2013;61(16):1661–1678. doi:10.1016/j.jacc.2012.11.072
- 8. Trimarchi S, Nienaber CA, Rampoldi V, et al. Contemporary results of surgery in acute type A aortic dissection: the International Registry of Acute Aortic Dissection experience. J Thorac Cardiovasc Surg. 2005;129(1):112–122. doi:10.1016/j.jtcvs.2004.09.005
- 9. Australasian Society for Cardiac and Thoracic Surgeons (ASCTS). ASCTS Annual Report — Cardiac Surgery Outcomes. Melbourne: ASCTS; 2023.
- 10. Australian Institute of Health and Welfare (AIHW). Cardiovascular disease in Aboriginal and Torres Strait Islander people. Cat. no. CVD 83. Canberra: AIHW; 2023.
- 11. Suzuki T, Distante A, Zizza A, et al. Diagnosis of acute aortic dissection by D-dimer: the International Registry of Acute Aortic Dissection Substudy on Biomarkers (IRAD-Bio) experience. Circulation. 2009;119(20):2702–2707. doi:10.1161/CIRCULATIONAHA.108.833004
- 12. Booher AM, Isselbacher EM, Nienaber CA, et al. The IRAD classification system for characterizing survival after aortic dissection. Am J Med. 2013;126(8):730.e19–730.e24. doi:10.1016/j.amjmed.2013.01.020
- 13. Heart Foundation of Australia. Guidelines for the management of absolute cardiovascular disease risk. Melbourne: National Heart Foundation of Australia; 2012 (updated 2023).
- 14. Goldfinger JZ, Halperin JL, Marin ML, et al. Thoracic aortic aneurysm and dissection. J Am Coll Cardiol. 2014;64(16):1725–1739. doi:10.1016/j.jacc.2014.08.025
- 15. Royal Australian College of General Practitioners (RACGP). Guidelines for preventive activities in general practice. 9th ed. East Melbourne: RACGP; 2016 (updated 2023).