📋 Key Information Summary
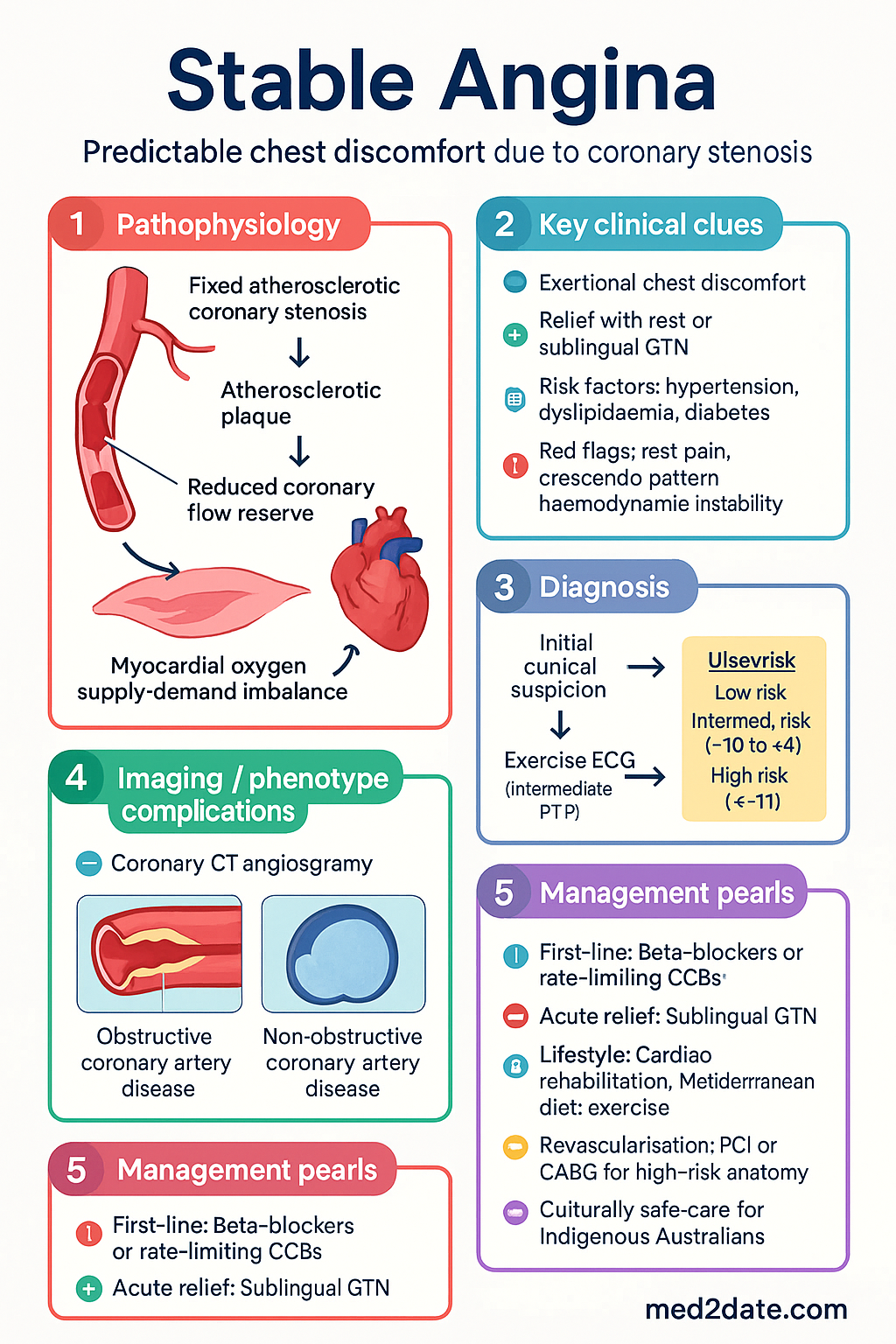
- Stable angina is caused by fixed atherosclerotic coronary stenosis producing predictable exertional chest discomfort relieved by rest or sublingual GTN; it affects approximately 1.2 million Australians and is a leading cause of GP presentations and hospital admissions.
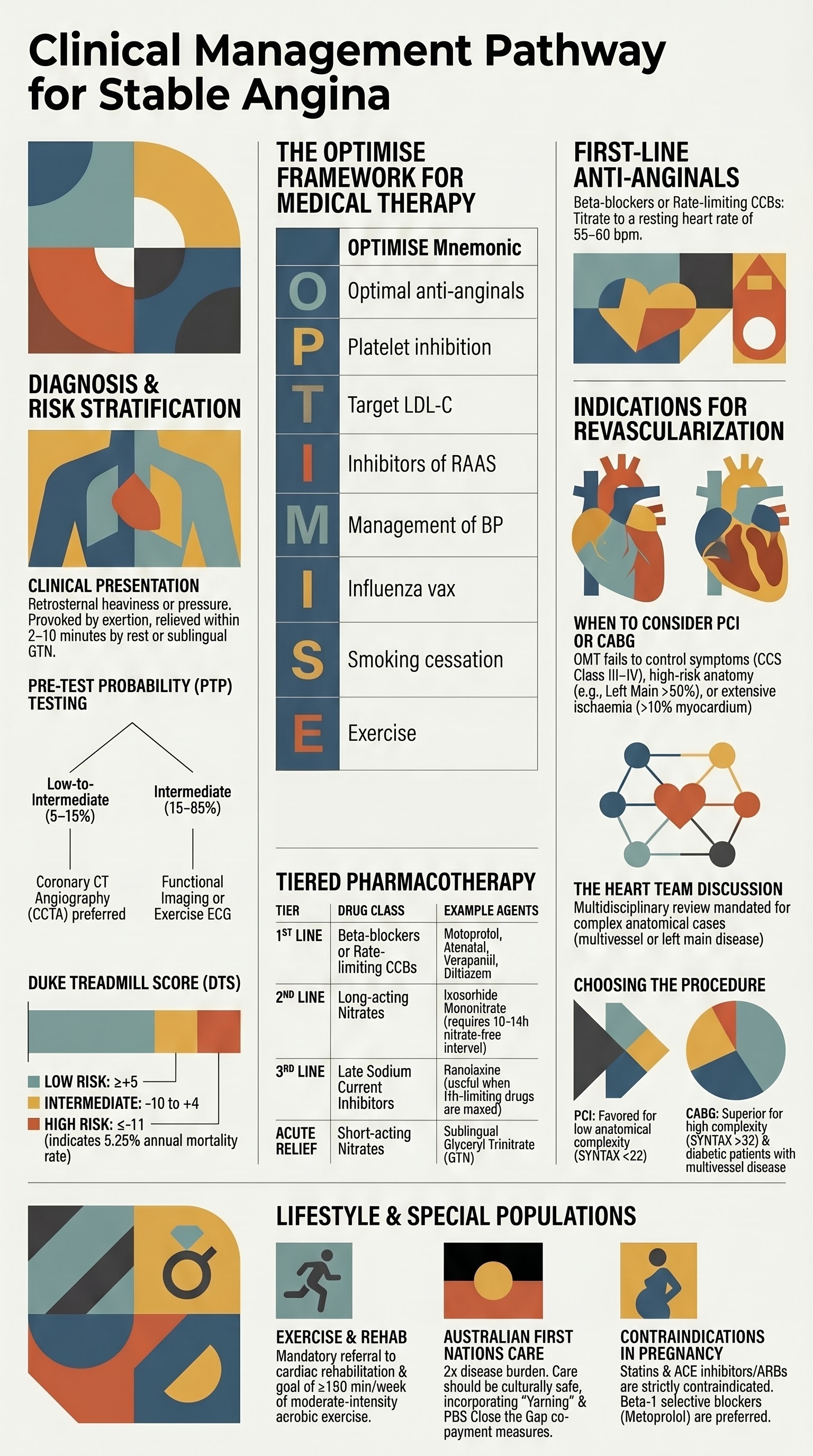
- Diagnosis is guided by pre-test probability (PTP) estimation incorporating age, sex, symptom typicality, and risk factors; exercise ECG remains first-line for intermediate PTP (15–65%), while functional imaging or coronary CT angiography (CCTA) is preferred for low-to-intermediate PTP or inconclusive exercise ECG.
- The Duke Treadmill Score stratifies exercise ECG results into low, intermediate, and high risk for major adverse cardiovascular events.
- First-line anti-anginal therapy is a beta-blocker (e.g. metoprolol, atenolol) or rate-limiting calcium channel blocker (e.g. verapamil, diltiazem); combination therapy is common and should be guided by heart rate, blood pressure, and left ventricular function.
- Sublingual glyceryl trinitrate (GTN) is used for acute symptom relief; long-acting nitrates are second-line add-on when beta-blockers or CCBs are inadequate or contraindicated.
- Ranolazine (Ranexa®) is a useful third-line agent for refractory angina, particularly when heart rate–limiting drugs are maximised or contraindicated.
- All patients require optimal medical therapy (OMT) including antiplatelet (aspirin or clopidogrel), statin, ACE inhibitor/ARB, and antihypertensive therapy before revascularisation is considered.
- Revascularisation (PCI or CABG) is indicated when OMT fails to control symptoms (Canadian Cardiovascular Society Class III–IV), when high-risk anatomy is identified (left main >50%, proximal LAD >70%, three-vessel disease with reduced EF), or when prognostic benefit exceeds OMT alone.
- The SYNTAX score and Heart Team discussion guide the choice between PCI and CABG; CABG is preferred for high SYNTAX scores (>32) and diabetes with multivessel disease.
- Structured cardiac rehabilitation, ≥150 min/week of moderate-intensity exercise, Mediterranean-style diet, smoking cessation, and weight management (target BMI 20–25 kg/m²) are mandatory lifestyle interventions.
- Aboriginal and Torres Strait Islander Australians have 1.7–2.0 times the burden of coronary heart disease; culturally safe care, opportunistic cardiovascular screening, and use of Indigenous health workers are essential.
- In pregnancy, beta-1–selective blockers (metoprolol) are preferred; statins are contraindicated; nitrates and low-dose aspirin may be continued with specialist input.
Introduction & Australian Epidemiology
Stable angina pectoris is the clinical manifestation of chronic, flow-limiting coronary artery disease (CAD) characterised by predictable episodes of chest discomfort provoked by exertion or emotional stress and relieved by rest or sublingual glyceryl trinitrate. It is the most common initial presentation of ischaemic heart disease in primary care and carries significant morbidity if not promptly identified and optimally managed.
In Australia, ischaemic heart disease remains the leading single cause of disease burden, responsible for an estimated 5.1% of total disability-adjusted life years (DALYs) in 2023. The Australian Institute of Health and Welfare (AIHW) reports that approximately 580,000 Australians aged ≥18 years have been diagnosed with coronary heart disease, with stable angina accounting for a substantial proportion of those with preserved left ventricular function. Hospital admissions for chronic ischaemic heart disease (ICD-10 I25) exceed 90,000 episodes annually, and stable angina generates over 2 million GP encounters per year.
Prevalence increases with age and is higher in males, Aboriginal and Torres Strait Islander peoples, and those with conventional cardiovascular risk factors (hypertension, dyslipidaemia, diabetes mellitus, smoking, obesity, and family history of premature CAD). The 2022–2023 National Health Survey estimated that 1 in 14 Australian adults self-report having heart disease, with regional and remote areas showing 20–40% higher hospitalisation rates than major cities.
This guideline covers the diagnosis, pharmacological management, revascularisation indications, and lifestyle modification strategies for stable angina, aligned with the National Heart Foundation of Australia / Cardiac Society of Australia and New Zealand (CSANZ) 2023 position statement, the ESC 2019 Chronic Coronary Syndromes guidelines (updated 2024), and current Therapeutic Guidelines (Cardiovascular) recommendations for Australian practice.
Pathophysiology
Stable angina results from an imbalance between myocardial oxygen supply and demand, typically driven by fixed atherosclerotic narrowing of one or more epicardial coronary arteries. Understanding the pathophysiology is essential for rational anti-anginal therapy.
Atherosclerotic Plaque and Flow Limitation
Chronic stable plaques consist of a fibrous cap overlying a lipid-rich necrotic core. Unlike acute coronary syndromes, these plaques are not prone to rupture under resting conditions. Symptoms occur when the stenosis exceeds approximately 50–70% of the vessel lumen diameter on angiography, reducing coronary flow reserve (CFR). During exercise or stress, tachycardia shortens diastolic filling time and increases myocardial oxygen demand (determined by heart rate × systolic blood pressure, i.e. rate-pressure product), precipitating ischaemia.
Coronary Microvascular Dysfunction
Up to 40% of patients with symptoms of stable angina have non-obstructive coronary arteries on angiography. Coronary microvascular dysfunction (CMD) — impaired vasodilatation of pre-arteriolar and arteriolar vessels — may be the underlying mechanism. CMD is more prevalent in women, patients with diabetes, and those with systemic inflammatory conditions. Functional testing with adenosine or regadenoson and measurement of coronary flow reserve (CFR) or index of microcirculatory resistance (IMR) can identify CMD.
Supply–Demand Mismatch Mechanisms
| Mechanism | Examples | Clinical Relevance |
|---|---|---|
| Reduced supply | Fixed epicardial stenosis, coronary spasm, anaemia, hypoxia, hypotension | Most common; angiographic severity correlates imperfectly with symptoms |
| Increased demand | Tachycardia, hypertension, LVH, thyrotoxicosis, catecholamine excess | Heart rate control is the cornerstone of anti-anginal therapy |
| Combined | Exercise in a patient with moderate stenosis and anaemia | Addressing reversible supply/demand factors improves symptoms |
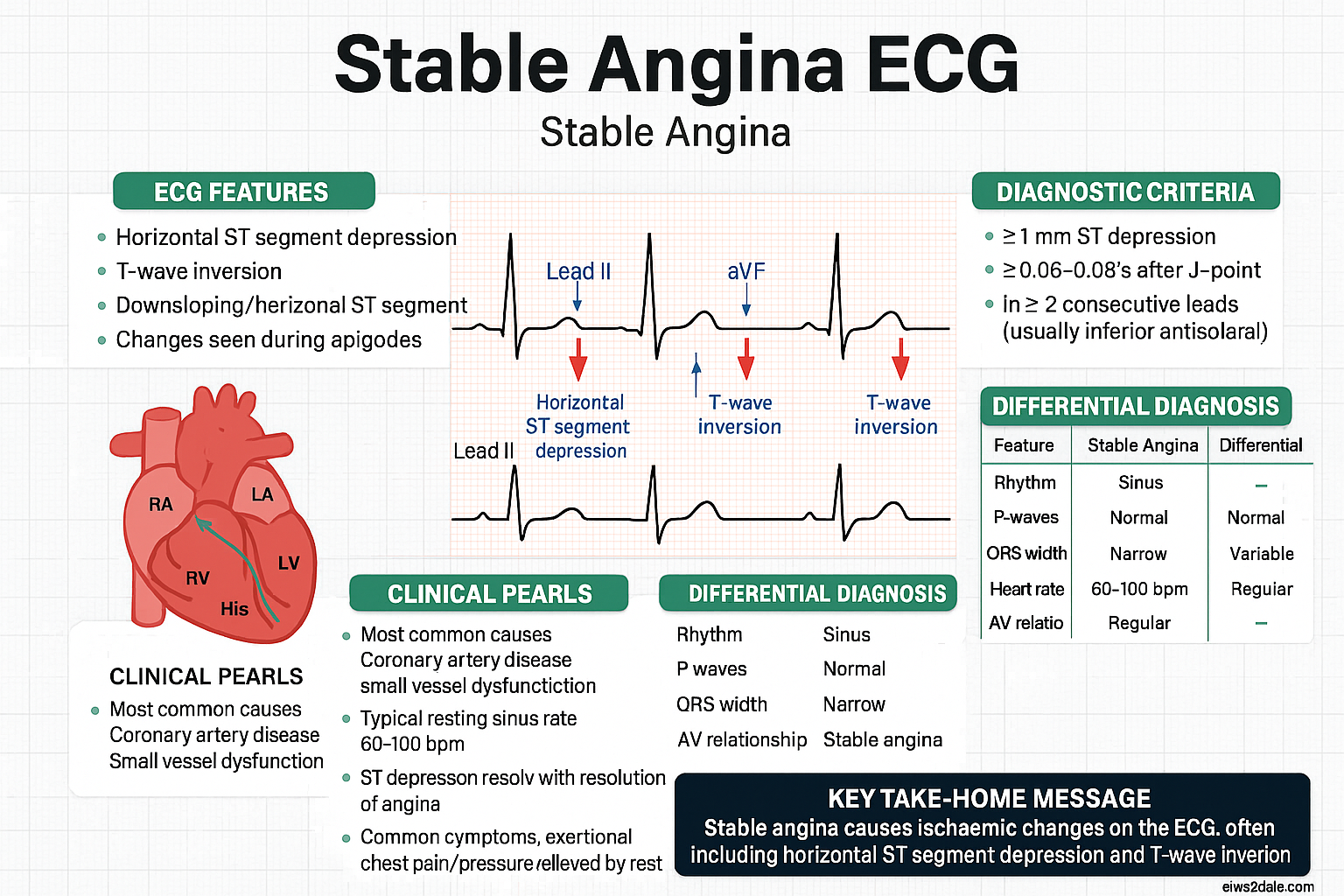
Ischaemic Cascade
The ischaemic cascade describes the sequential events: perfusion abnormality → diastolic dysfunction → regional wall motion abnormality → ECG changes → chest pain. This explains why functional imaging (detecting perfusion or wall motion changes) may be more sensitive than exercise ECG in identifying ischaemia, particularly in single-vessel or left circumflex territory disease.
Diagnosis & Risk Assessment
Clinical History and Symptom Characterisation
The clinical history remains the cornerstone of diagnosis. Chest discomfort characteristic of stable angina is described as retrosternal heaviness, tightness, pressure, or squeezing provoked by exertion (e.g. walking uphill, carrying shopping) and relieved within 2–10 minutes by rest or sublingual GTN. Atypical features include radiation to the left arm, jaw, neck, or epigastrium; associated dyspnoea, nausea, or diaphoresis; and provocation by cold weather or heavy meals.
Pre-test Probability (PTP) Estimation
The 2019 ESC guidelines recommend estimating PTP of significant CAD using the updated clinical prediction model incorporating age, sex, and symptom typicality. This stratification guides the selection of diagnostic testing.
| PTP Category | Probability (%) | Recommended Initial Test |
|---|---|---|
| Very low | <5% | No further cardiac testing; consider alternative diagnoses |
| Low | 5–15% | Coronary CT angiography (CCTA) preferred; functional imaging if CCTA contraindicated or equivocal |
| Intermediate | 15–65% | Exercise ECG (if baseline ECG normal and patient able to exercise) or functional imaging (stress echocardiography, myocardial perfusion scintigraphy, cardiac MRI stress) |
| High | 65–90% | Invasive coronary angiography; functional imaging acceptable if high PTP is driven by risk factors rather than typical angina |
| Very high | >90% | Direct invasive coronary angiography |
Stress Testing — Exercise ECG
The Bruce protocol exercise ECG test is widely available across Australian hospitals and private cardiology practices (MBS Item 11712). It is the initial test of choice for patients with intermediate PTP who have a normal resting ECG and can exercise adequately. Sensitivity is approximately 68% and specificity 77%, but the test provides additional prognostic information via the Duke Treadmill Score.
Functional Imaging
Functional testing is preferred when exercise ECG is uninterpretable (left bundle branch block, ventricular pacing, digoxin use, resting ST depression >1 mm, inability to exercise) or when localisation and quantification of ischaemia are needed to guide management.
Coronary CT Angiography (CCTA)
CCTA has emerged as a first-line non-invasive anatomical test for low-to-intermediate PTP. It has high sensitivity (~97%) and excellent negative predictive value (~99%), making it highly effective for ruling out obstructive CAD. The SCOT-HEART and PROMISE trials demonstrated that CCTA alters clinical management in 25–40% of patients and reduces myocardial infarction rates compared with standard care.
Functional CT — CT-derived fractional flow reserve (CT-FFR or HeartFlow®) — is available at select Australian centres and may reduce the need for downstream invasive angiography when moderate stenoses (40–70%) are detected on CCTA.
Invasive Coronary Angiography
Indicated for high/very-high PTP, high-risk non-invasive test results (DTS ≤−11, extensive ischaemia on imaging, ejection fraction <50%), or when non-invasive testing is inconclusive and clinical suspicion remains high. It is the gold standard for defining coronary anatomy and enables physiological assessment (FFR, iFR) to guide revascularisation decisions. MBS Item 38218 (diagnostic coronary angiography).
Risk Assessment and Prognostic Stratification
Once CAD is confirmed, risk stratification guides intensity of therapy and timing of revascularisation:
- Low risk: Normal LV function, single- or two-vessel disease without proximal LAD involvement, negative exercise ECG at high workload, DTS ≥+5. Manage with OMT; revascularisation for symptom control only.
- Intermediate risk: Moderate LV dysfunction (EF 35–50%), two-vessel disease with proximal LAD, positive stress test at moderate workload, DTS −10 to +4. Heart Team discussion recommended.
- High risk: Severe LV dysfunction (EF <35%), left main stenosis ≥50%, three-vessel disease, proximal LAD stenosis ≥70% with additional vessel disease, high DTS (≤−11), extensive ischaemia (>10% myocardium on imaging). Revascularisation strongly recommended with prognostic benefit.
Medical Therapy
All patients with stable angina require optimal medical therapy (OMT) comprising: (1) anti-anginal agents to improve symptoms and quality of life, and (2) disease-modifying agents to reduce cardiovascular events and mortality. Anti-anginal therapy should be titrated to achieve freedom from symptoms or to reach resting heart rate 55–60 bpm before adding additional agents or considering revascularisation.
First-line Anti-anginal Agents
Beta-Adrenoceptor Blockers
Beta-blockers reduce myocardial oxygen demand by decreasing heart rate, myocardial contractility, and blood pressure. They prolong diastolic filling time, improving coronary perfusion. They are first-line therapy for stable angina, particularly in patients with prior myocardial infarction, reduced ejection fraction, hypertension, or tachyarrhythmias.
Rate-limiting Calcium Channel Blockers (CCBs)
Non-dihydropyridine CCBs (verapamil, diltiazem) reduce heart rate and myocardial contractility. They are first-line alternatives to beta-blockers, or can be used in combination when beta-blocker monotherapy is insufficient. Dihydropyridine CCBs (amlodipine, nifedipine) are vasodilators without significant rate-lowering effect and are combined with beta-blockers when additional blood pressure control or coronary vasodilatation is needed.
Second-line Anti-anginal Agents
Nitrates
Sublingual glyceryl trinitrate (GTN) is used for immediate relief of angina. Long-acting nitrates (isosorbide mononitrate, isosorbide dinitrate) reduce preload and afterload and provide coronary vasodilatation. A nitrate-free interval of 10–14 hours (typically overnight) is essential to prevent tolerance. Long-acting nitrates are second-line add-on therapy when beta-blockers or CCBs are inadequate.
Ranolazine
Ranolazine is a piperazine derivative that inhibits the late sodium current (INa) in myocardial cells, reducing intracellular calcium overload during ischaemia. It reduces angina frequency without significantly affecting heart rate or blood pressure, making it a valuable third-line agent or add-on when rate-lowering drugs are maximised or contraindicated.
Anti-anginal Combination Strategy
When monotherapy is insufficient, combinations should be chosen based on mechanism, haemodynamic profile, and comorbidities:
| Combination | Indication | Cautions |
|---|---|---|
| Beta-blocker + Dihydropyridine CCB (amlodipine) | Inadequate symptom control with beta-blocker alone; hypertension comorbidity | Generally safe; monitor for hypotension and peripheral oedema |
| Beta-blocker + Diltiazem or Verapamil | Refractory angina despite maximised monotherapy; normal EF | Avoid if EF <50%, PR interval >240 ms, or 2nd/3rd degree AV block. Requires specialist supervision. |
| Beta-blocker + Long-acting nitrate | Add-on for persistent exertional or vasospastic symptoms | Avoid with PDE-5 inhibitors. Maintain nitrate-free interval. |
| Beta-blocker (or CCB) + Ranolazine | Refractory angina on dual anti-anginal therapy | Check CYP2D6 interaction with metoprolol; adjust doses accordingly. |
Disease-Modifying Therapy (Secondary Prevention)
All patients with confirmed CAD require the following regardless of symptom severity:
Revascularisation Indications
Revascularisation by percutaneous coronary intervention (PCI) or coronary artery bypass grafting (CABG) should be considered in the context of a Heart Team discussion that weighs symptom burden, anatomical complexity, left ventricular function, comorbidities, and patient preference. It is broadly indicated for: (1) failure of optimal medical therapy to control symptoms, (2) high-risk anatomy where revascularisation offers prognostic benefit over OMT alone, and (3) patient preference after informed shared decision-making.
Indications for Revascularisation
PCI vs. CABG — Decision Framework
| Factor | Favour PCI | Favour CABG |
|---|---|---|
| Anatomical complexity | SYNTAX score 0–22 (low) | SYNTAX score 23–32 (intermediate) or ≥33 (high) |
| Left main disease | Low SYNTAX score, ostial/shaft lesion | Distal bifurcation, high SYNTAX score, LV dysfunction |
| Diabetes | Single-vessel or simple two-vessel disease | Multivessel disease (FREEDOM trial: CABG superior for MACE reduction) |
| LV function | Preserved (EF >50%) | Reduced (EF <50%), especially with viable myocardium |
| Frailty / comorbidity | High surgical risk (STS score >5%), severe COPD, porcelain aorta | Low surgical risk, suitable conduit availability |
| Patient preference | Desires shorter recovery, less invasive approach | Accepts longer recovery for more durable revascularisation |
Key Trial Evidence
| Trial | Key Finding | Relevance to Practice |
|---|---|---|
| ISCHEMIA (2020) | Invasive strategy vs. OMT in stable CAD with moderate–severe ischaemia: no reduction in death or MI at median 3.2 years; improved angina-related quality of life in patients with baseline angina | Supports OMT as initial strategy; revascularisation primarily for symptom relief unless high-risk anatomy |
| COURAGE (2007) | PCI + OMT vs. OMT alone: no difference in death or MI; improved symptom control with PCI in CCS class III–IV | OMT is essential regardless of PCI; PCI for residual symptoms |
| FAME 2 (2014) | FFR-guided PCI + OMT vs. OMT alone in functionally significant stenosis (FFR ≤0.80): reduced urgent revascularisation | Physiological assessment (FFR/iFR) should guide PCI in intermediate stenoses |
| SYNTAX (2009, 10-year follow-up) | CABG superior to PCI for three-vessel and left main disease with high SYNTAX score | SYNTAX score calculation is mandatory for multivessel disease planning |
| FREEDOM (2012) | CABG superior to PCI in diabetic patients with multivessel CAD for composite death, MI, stroke | CABG is the preferred revascularisation strategy in diabetes with multivessel disease |
Australian Access and MBS Items
PCI is performed at over 60 cardiac catheterisation laboratories across Australia, including regional centres in major states (MBS Item 38300). CABG requires tertiary cardiac surgical services (available in all state capital cities). Access to PCI is generally within 24–48 hours for urgent cases; elective PCI wait times in the public system average 30–60 days. In remote areas, aeromedical retrieval to the nearest PCI-capable centre (primary PCI networks) ensures timely access.
Lifestyle & Risk Factor Modification
Lifestyle modification is a cornerstone of stable angina management and secondary prevention. The 2023 NHFA/CSANZ Position Statement on Cardiovascular Disease Prevention emphasises that lifestyle interventions are as important as pharmacotherapy and should be initiated at the time of diagnosis alongside OMT.
Exercise Prescription
Regular exercise improves exercise capacity, reduces angina frequency, improves endothelial function, and reduces cardiovascular mortality. The exercise prescription should be individualised based on exercise capacity, symptom threshold, and comorbidities.
Dietary Modifications
A Mediterranean-style dietary pattern has the strongest evidence base for secondary prevention (PREDIMED trial, Lyon Diet Heart Study). Key recommendations:
- Increase: Vegetables (≥5 serves/day), fruits (≥2 serves/day), whole grains, legumes, nuts, seeds, extra-virgin olive oil, oily fish (≥2 serves/week for omega-3 fatty acids).
- Reduce: Saturated fat (<7% of total energy), trans fats (avoid), sodium (<2,000 mg/day or <5 g salt/day), added sugars, processed and red meat.
- Limit alcohol: ≤10 standard drinks/week; no more than 4 on any single day (NHMRC 2020 Guidelines).
- Dietary patterns: Mediterranean diet, DASH diet, or plant-predominant dietary patterns are all associated with 25–30% reduction in major cardiovascular events.
Smoking Cessation
Smoking is the single most modifiable risk factor for CAD progression. Cessation reduces cardiovascular mortality by 36% within 2–5 years. A structured approach combining behavioural support (Quitline 13 7848) with pharmacotherapy is recommended:
Weight Management
Obesity (BMI ≥30 kg/m²) and central adiposity (waist circumference >94 cm in men, >80 cm in women) are independent risk factors for CAD progression. Target BMI 20–25 kg/m² (or ≥5% weight loss if obese). Management includes dietary counselling, structured exercise, and consideration of pharmacotherapy (e.g. semaglutide, liraglutide) or bariatric surgery in eligible patients with BMI ≥40 (or ≥35 with comorbidities).
Psychosocial Factors
Depression, anxiety, social isolation, and chronic psychosocial stress are common in CAD patients and are independently associated with worse cardiovascular outcomes. Routine screening (PHQ-9, GAD-7) is recommended. Management includes psychological support (cognitive behavioural therapy), social prescribing, and pharmacotherapy for moderate–severe depression (SSRIs are first-line; sertraline and citalopram have the most cardiac safety data).
Special Populations
Pregnancy
Beta-blockers: Metoprolol (Category B) and labetalol (Category C) are preferred. Avoid atenolol (associated with fetal growth restriction). Bisoprolol is Category C.
Statins: Contraindicated in pregnancy. Cease at least 1 month before conception (Category X — teratogenicity risk). Switch to ezetimibe if needed for lipid management.
Nitrates: GTN may be used; limited safety data for long-acting nitrates. Use with caution.
Aspirin: Low-dose aspirin (100–150 mg) is continued for secondary prevention; also indicated for pre-eclampsia prevention in high-risk women.
Ranolazine: Avoid — limited safety data.
ACE inhibitors / ARBs: Contraindicated in pregnancy (teratogenic: fetopathy, oligohydramnios). Switch to methyldopa, labetalol, or nifedipine for blood pressure control.
Coronary angiography with minimal fluoroscopy and shielding is acceptable if clinically indicated. PCI is preferred over CABG if revascularisation is required during pregnancy. Multidisciplinary management with obstetrics, cardiology, and maternal-fetal medicine is essential.
Paediatrics
Stable angina is exceedingly rare in the paediatric population. Consider coronary anomalies (anomalous left coronary artery from the pulmonary artery — ALCAPA), Kawasaki disease–associated coronary artery aneurysms, or inherited cardiomyopathies (hypertrophic cardiomyopathy) in children presenting with exertional chest pain.
Kawasaki disease follow-up: Children with coronary aneurysms (z-score ≥2.5) may develop flow-limiting stenoses and angina. Low-dose aspirin (3–5 mg/kg/day) is lifelong for those with persistent aneurysms.
Refer to paediatric cardiology for stress testing and imaging in children with suspected cardiac chest pain. Adult anti-anginal drug doses are not applicable; consult tertiary paediatric cardiology protocols.
Elderly (≥75 years)
The elderly have a higher prevalence of stable angina but are more likely to present with atypical symptoms (dyspnoea, fatigue, syncope rather than classic chest pain). Polypharmacy and multimorbidity necessitate careful medication review.
Beta-blockers: Start at half the usual dose (e.g. metoprolol 12.5–25 mg BD). Monitor for bradycardia, hypotension, fatigue, and falls. Avoid if resting HR <50 bpm or systolic BP <100 mmHg.
CCBs: Amlodipine is well tolerated; verapamil and diltiazem require cautious titration. Monitor for constipation (verapamil) and peripheral oedema (dihydropyridines).
Statins: High-intensity statins remain appropriate; however, consider frailty, life expectancy, and patient goals. Myopathy risk is increased — monitor CK and liver function.
Aspirin: Discuss bleeding risk (GI bleeding, intracranial haemorrhage). Consider concomitant PPI (e.g. esomeprazole 20 mg daily) for gastroprotection.
Revascularisation decisions in the elderly should incorporate frailty assessment (Clinical Frailty Scale), cognitive status, and patient values. CABG carries higher operative risk (EuroSCORE II, STS score); PCI may be preferred with Heart Team agreement.
Renal Impairment
Chronic kidney disease (CKD) is both a risk factor for CAD and a prognosticator of worse outcomes post-revascularisation. Prevalence of CKD in CAD patients is approximately 30–40%.
Beta-blockers: Metoprolol (hepatically cleared) — no adjustment. Atenolol — dose reduce or avoid in eGFR <30 mL/min (renally cleared).
Ranolazine: Maximum 375 mg BD in eGFR 15–30 mL/min; avoid in eGFR <15.
Statins: Atorvastatin — no dose adjustment (preferred in CKD). Rosuvastatin — maximum 10 mg if eGFR <30 mL/min. Avoid simvastatin >10 mg with concurrent verapamil or diltiazem (myopathy risk).
Contrast for angiography/imaging: Use iso-osmolar or low-osmolar contrast; pre-hydrate with IV saline (1 mL/kg/h for 6–12 hours pre- and post-procedure); limit contrast volume. CKD-EPI eGFR <30 mL/min: discuss risk–benefit with nephrology and interventional cardiology.
Clopidogrel is preferred over ticagrelor or prasugrel if dual antiplatelet therapy is needed (no renal dose adjustment).
Hepatic Impairment
Verapamil: Reduce dose by 50–70% in hepatic impairment (high first-pass metabolism). Risk of AV block and heart failure.
Amlodipine: Start 2.5 mg daily; titrate slowly.
Metoprolol: Consider dose reduction in severe hepatic impairment; monitor HR and BP closely.
Statins: Use with caution; contraindicated in active liver disease or unexplained persistent transaminase elevations >3× ULN. Atorvastatin and pravastatin have the most favourable hepatic safety profile.
Ranolazine: Child-Pugh A — no adjustment; Child-Pugh B — maximum 375 mg BD; Child-Pugh C — avoid.
Avoid long-acting nitrates in severe hepatic impairment due to increased bioavailability and risk of hypotension.
Immunocompromised
Patients with HIV, organ transplant recipients, and those on immunosuppressive therapy have accelerated atherosclerosis and higher rates of stable angina. HIV-associated CAD may involve plaque morphology distinct from traditional atherosclerosis (more non-calcified, inflammatory plaques).
Drug interactions: Protease inhibitors (e.g. ritonavir) significantly inhibit CYP3A4 — avoid verapamil, diltiazem, and ranolazine (risk of toxicity). Use amlodipine with caution. Atorvastatin maximum 20 mg with most protease inhibitors. Consult HIV drug interaction databases (e.g. Liverpool HIV Interaction Checker).
Calcineurin inhibitors: Tacrolimus and cyclosporine increase statin levels — prefer pravastatin or fluvastatin with monitoring of immunosuppressant trough levels.
Cardiac risk assessment should be part of routine cardiovascular screening in immunocompromised patients, with a lower threshold for investigation.
Aboriginal and Torres Strait Islander Australians experience coronary heart disease at 1.7–2.0 times the rate of non-Indigenous Australians, with earlier onset (10–15 years younger on average), more severe disease at presentation, and higher case-fatality rates. The AIHW reports that cardiovascular disease accounts for approximately 22% of the Indigenous health gap. Culturally safe, person-centred care and community-based health strategies are essential to addressing these disparities.
📚 References
- 1. Knuuti J, Wijns W, Saraste A, et al. 2019 ESC Guidelines for the diagnosis and management of chronic coronary syndromes. Eur Heart J. 2020;41(3):407-477. doi:10.1093/eurheartj/ehz425
- 2. National Heart Foundation of Australia and Cardiac Society of Australia and New Zealand. Australian clinical guidelines for the diagnosis and management of chronic coronary syndromes. Heart Lung Circ. 2023;32(11):1318-1364.
- 3. Maron DJ, Hochman JS, Reynolds HR, et al. Initial invasive or conservative strategy for stable coronary disease. N Engl J Med. 2020;382(15):1395-1407. doi:10.1056/NEJMoa1915922 (ISCHEMIA trial)
- 4. Boden WE, O'Rourke RA, Teo KK, et al. Optimal medical therapy with or without PCI for stable coronary disease. N Engl J Med. 2007;356(15):1503-1516. doi:10.1056/NEJMoa070829 (COURAGE trial)
- 5. De Bruyne B, Fearon WF, Pijls NHJ, et al. Fractional flow reserve-guided PCI for stable coronary artery disease. N Engl J Med. 2014;371(13):1208-1217. doi:10.1056/NEJMoa1408758 (FAME 2 trial)
- 6. Serruys PW, Morice MC, Kappetein AP, et al. Percutaneous coronary intervention versus coronary-artery bypass grafting for severe coronary artery disease. N Engl J Med. 2009;360(10):961-972. doi:10.1056/NEJMoa0804626 (SYNTAX trial)
- 7. Farkouh ME, Domanski M, Sleeper LA, et al. Strategies for multivessel revascularization in patients with diabetes. N Engl J Med. 2012;367(25):2375-2384. doi:10.1056/NEJMoa1211585 (FREEDOM trial)
- 8. SCOT-HEART Investigators. CT coronary angiography in patients with suspected angina due to coronary heart disease (SCOT-HEART): an open-label, parallel-group, multicentre trial. Lancet. 2015;385(9985):2383-2391. doi:10.1016/S0140-6736(15)60291-4
- 9. Douglas PS, Hoffmann U, Patel MR, et al. Outcomes of anatomical versus functional testing for coronary artery disease. N Engl J Med. 2015;372(14):1291-1300. doi:10.1056/NEJMoa1415516 (PROMISE trial)
- 10. Australian Institute of Health and Welfare. Heart, stroke and vascular disease — Australian facts. AIHW, Canberra; 2023. Cat. no. CVD 88.
- 11. National Health and Medical Research Council. Australian guidelines to reduce health risks from drinking alcohol. NHMRC, Canberra; 2020.
- 12. Estruch R, Ros E, Salas-Salvadó J, et al. Primary prevention of cardiovascular disease with a Mediterranean diet supplemented with extra-virgin olive oil or nuts. N Engl J Med. 2018;378(25):e34. doi:10.1056/NEJMoa1800389 (PREDIMED trial)
- 13. Anderson L, Oldridge N, Thompson DR, et al. Exercise-based cardiac rehabilitation for coronary heart disease: Cochrane systematic review and meta-analysis. J Am Coll Cardiol. 2016;67(1):1-12. doi:10.1016/j.jacc.2015.10.044
- 14. de Lorgeril M, Salen P, Martin JL, et al. Mediterranean diet, traditional risk factors, and the rate of cardiovascular complications after myocardial infarction: final report of the Lyon Diet Heart Study. Circulation. 1999;99(6):779-785. doi:10.1161/01.CIR.99.6.779
- 15. Australian Bureau of Statistics. National Aboriginal and Torres Strait Islander Health Survey 2018–19. ABS, Canberra; 2019. Cat. no. 4715.0.
- 16. Marso SP, Bain SC, Consoli A, et al. Semaglutide and cardiovascular outcomes in patients with type 2 diabetes. N Engl J Med. 2016;375(19):1834-1844. doi:10.1056/NEJMoa1607141 (SUSTAIN-6 trial)
- 17. Lincoff AM, Brown-Frandsen K, Colhoun HM, et al. Semaglutide and cardiovascular outcomes in obesity without diabetes. N Engl J Med. 2023;389(24):2221-2232. doi:10.1056/NEJMoa2307563 (SELECT trial)