📋 Key Information Summary
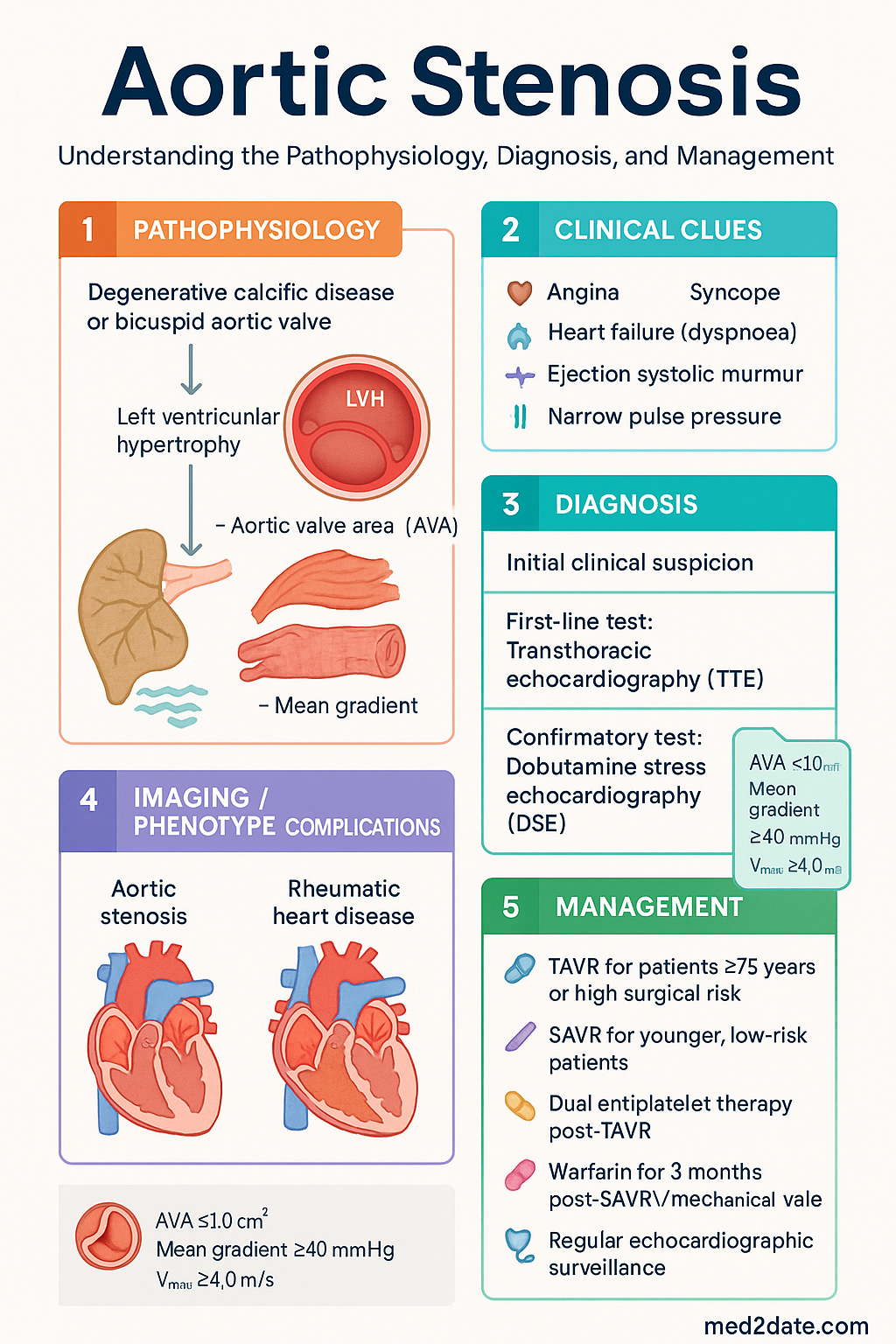
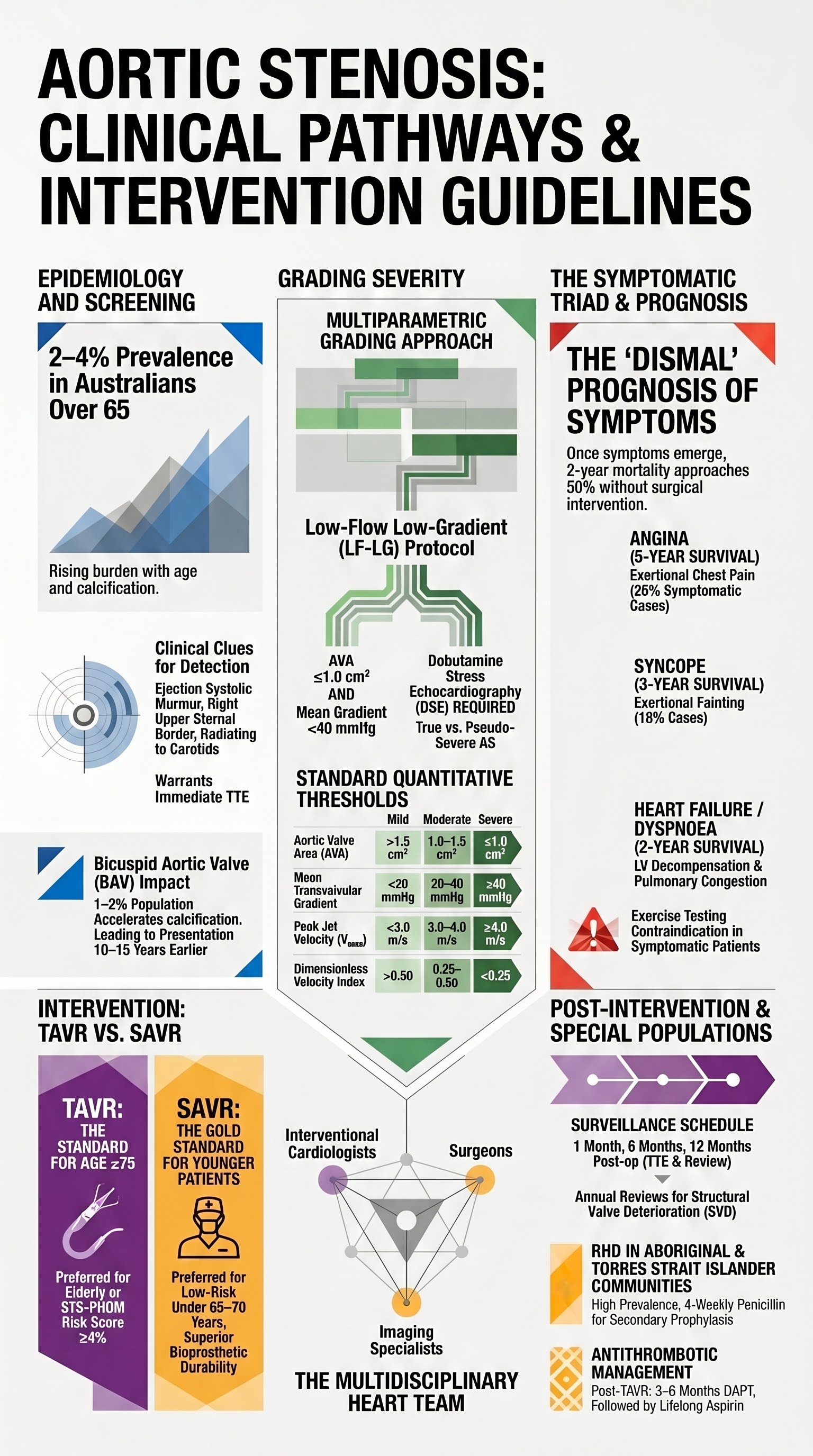
- Aortic stenosis (AS) is the most common valvular heart disease in Australia, with prevalence increasing sharply after age 65, driven by degenerative calcific disease.
- Severity grading relies on echocardiography: mild (AVA >1.5 cm², mean gradient <20 mmHg, Vmax <3.0 m/s), moderate (AVA 1.0–1.5 cm², mean gradient 20–40 mmHg, Vmax 3.0–4.0 m/s), and severe (AVA ≤1.0 cm², mean gradient ≥40 mmHg, Vmax ≥4.0 m/s).
- Low-flow low-gradient severe AS (AVA ≤1.0 cm², mean gradient <40 mmHg, LVEF <50%) requires dobutamine stress echocardiography to distinguish true severe AS from pseudo-severe AS.
- Symptomatic severe AS carries a dismal prognosis without intervention (2-year mortality ~50%); classic triad includes angina, syncope, and heart failure (dyspnoea).
- Exercise testing is contraindicated in symptomatic AS but is recommended in asymptomatic severe AS to unmask latent symptoms or abnormal blood pressure response.
- TAVR (transcatheter aortic valve replacement) is now the standard of care for patients aged ≥75 years or those at high/intermediate surgical risk (STS-PROM ≥4%), and is increasingly used in low-risk patients based on trial data.
- Surgical AVR (SAVR) remains the gold standard for younger, low-risk patients and those with concomitant cardiac pathology requiring surgery (e.g., severe CAD, mitral disease).
- Asymptomatic severe AS with very low AVA (≤0.6 cm²), rapid progression (Vmax increase ≥0.3 m/s/year), elevated BNP, or abnormal exercise response should be considered for early intervention.
- Post-TAVR management includes dual antiplatelet therapy (aspirin + clopidogrel) for 3–6 months; post-SAVR management includes warfarin for 3 months if a mechanical valve is used; bioprosthetic valves require only aspirin long-term.
- Paravalvular leak (PVL) post-TAVR is common (10–25% mild); moderate-to-severe PVL warrants consideration of percutaneous closure. Structural valve deterioration (SVD) mandates regular echocardiographic surveillance.
- Aboriginal and Torres Strait Islander peoples experience higher rates of rheumatic heart disease–related valvular pathology, later presentation, and barriers to specialist access, requiring culturally safe pathways and outreach echocardiography programmes.
- Multidisciplinary Heart Team discussion is mandatory for all patients being considered for valve intervention to ensure evidence-based, patient-centred decision-making.
Introduction & Australian Epidemiology
Aortic stenosis (AS) is the most prevalent valvular heart disease in high-income countries, including Australia. Degenerative calcific AS accounts for the vast majority of cases in adults aged >65 years, with prevalence estimated at 2–4% of Australians over 65 and rising sharply with age. Bicuspid aortic valve (BAV), affecting approximately 1–2% of the population, accelerates calcification and typically presents 10–15 years earlier than trileaflet degenerative AS. Rheumatic AS remains an important cause in Aboriginal and Torres Strait Islander communities and in migrants from endemic regions.
The Australian Institute of Health and Welfare (AIHW) reports that valvular heart disease accounts for a significant proportion of cardiac surgical admissions nationally. With Australia's ageing population, the burden of AS is projected to increase substantially over the coming decades, placing greater demands on echocardiography services, Heart Team capacity, and access to both surgical AVR (SAVR) and transcatheter aortic valve replacement (TAVR).
AS progresses from a prolonged asymptomatic phase to a symptomatic phase characterised by angina, syncope, and heart failure. Once symptoms develop, prognosis without intervention is poor — median survival is approximately 2–5 years depending on symptom severity. Timely detection through clinical examination (ejection systolic murmur, narrow pulse pressure, slow-rising carotid pulse) and confirmation with transthoracic echocardiography (TTE) are the cornerstones of early management.
Grading Severity
Accurate grading of AS severity is essential for clinical decision-making. Transthoracic echocardiography (TTE) is the primary diagnostic modality. The 2020 ACC/AHA and 2021 ESC/EACTS guidelines endorse a multiparametric approach integrating valve area, transvalvular gradients, and flow velocities.
Standard Echocardiographic Parameters
| Parameter | Mild | Moderate | Severe |
|---|---|---|---|
| Aortic valve area (AVA) | >1.5 cm² | 1.0–1.5 cm² | ≤1.0 cm² |
| Indexed AVA (AVAi) | >0.85 cm²/m² | 0.60–0.85 cm²/m² | ≤0.6 cm²/m² |
| Mean transvalvular gradient | <20 mmHg | 20–40 mmHg | ≥40 mmHg |
| Peak aortic jet velocity (Vmax) | <3.0 m/s | 3.0–4.0 m/s | ≥4.0 m/s |
| Dimensionless velocity index (DVi) | >0.50 | 0.25–0.50 | <0.25 |
Low-Flow Low-Gradient AS
Low-flow low-gradient (LF-LG) AS is defined as AVA ≤1.0 cm² with mean gradient <40 mmHg and stroke volume index (SVi) ≤35 mL/m². It accounts for 5–10% of severe AS presentations and may occur with reduced LVEF (<50%) or with preserved LVEF (normal-flow LG or paradoxical LF-LG).
Reduced LVEF LF-LG AS (classical LF-LG): Distinguishing true severe AS from pseudo-severe AS (where low flow causes incomplete valve opening of a moderately diseased valve) is critical. Dobutamine stress echocardiography (DSE) is the recommended investigation.
Dobutamine Stress Echocardiography Protocol
Paradoxical low-flow low-gradient AS (preserved LVEF): Occurs when LVEF is ≥50% but SVi is ≤35 mL/m² due to pronounced LV concentric remodelling, small LV cavity, diastolic dysfunction, atrial fibrillation, or significant mitral regurgitation. AVA is ≤1.0 cm² with mean gradient <40 mmHg. CT calcium scoring of the aortic valve (Agatston score >2000 AU in men, >1200 AU in women) can help confirm true severe AS in equivocal cases. Cardiac MRI may also be useful for quantifying flow and LV geometry.
CT Aortic Valve Calcium Scoring
CT calcium scoring of the aortic valve is increasingly used in Australian centres (available at major tertiary hospitals; MBS item numbers for CT coronary angiography may apply in selected cases, though dedicated valve calcium scoring is not separately listed on the MBS). Thresholds for severe AS:
- Men: >2000 Agatston units (AU)
- Women: >1200 AU
This is particularly useful when echo parameters are discordant and DSE is not feasible or inconclusive.
Symptomatic Severe AS
The development of symptoms in severe AS marks a critical inflection point. Once the classic triad emerges, the natural history becomes devastating without intervention, with 2-year mortality approaching 50% in patients with heart failure symptoms.
Classic Triad
Role of Exercise Testing
Exercise testing is contraindicated in symptomatic severe AS. It plays a vital role only in asymptomatic severe AS (discussed below).
In symptomatic patients, the diagnosis and severity assessment are established by resting TTE. Exercise testing in this context is unsafe and unnecessary — the presence of symptoms with confirmed severe AS on echo is sufficient to recommend intervention.
Timing of Intervention
Intervention (SAVR or TAVR) is a Class I recommendation for symptomatic severe AS, regardless of LVEF. Key timing considerations:
- Urgent/emergent intervention: Patients presenting with acute decompensated heart failure, cardiogenic shock, or haemodynamic instability secondary to AS require stabilisation (inotropes, cautious diuresis, avoidance of vasodilators) followed by expedited intervention.
- Early intervention: Once symptoms are confirmed and severe AS is documented, intervention should not be delayed. Prolonged waiting increases the risk of irreversible LV dysfunction, sudden death, and operative mortality.
- Pre-operative optimisation: Address reversible comorbidities (anaemia, renal impairment, infection) but do not delay intervention indefinitely. Coronary angiography should be performed pre-SAVR; for TAVR, CT coronary angiography may suffice.
TAVR vs Surgical AVR
The choice between transcatheter aortic valve replacement (TAVR) and surgical aortic valve replacement (SAVR) is one of the most significant decisions in valvular heart disease management. All patients should be evaluated by a multidisciplinary Heart Team (interventional cardiologist, cardiac surgeon, imaging specialist, anaesthetist, geriatrician where appropriate) and undergo shared decision-making with the patient.
Risk Assessment
Surgical risk stratification guides the choice between SAVR and TAVR. Multiple scoring systems are used in Australian practice:
| Scoring System | Low Risk | Intermediate Risk | High Risk | Prohibitive Risk |
|---|---|---|---|---|
| STS-PROM | <4% | 4–8% | >8% | Predicted mortality >15% or ≥50% risk of irreversible morbidity |
| EuroSCORE II | <4% | 4–10% | >10% | Not directly applicable |
In addition to formal scores, the Heart Team integrates frailty indices, porcelain aorta, hostile chest (prior radiation, chest wall deformity), liver disease, prior cardiac surgery, and patient cognitive/psychosocial status.
Anatomical Suitability for TAVR
Pre-procedural CT angiography (aorto-femoral or CT aorta with 3D reconstruction) is mandatory for TAVR planning. Key measurements include:
- Aortic annulus: Perimeter, area, and mean diameter — determines prosthesis sizing
- Sinus of Valsalva: Height and width — coronary obstruction risk
- Sinotubular junction: Diameter — sealing and anchoring
- Ascending aorta: Diameter and tortuosity
- Iliofemoral access: Minimum lumen diameter (≥5.0–5.5 mm for most current systems), calcification, tortuosity
- Distance from annulus to coronary ostia: ≥10 mm reduces coronary obstruction risk
- Aortic valve morphology: Bicuspid vs trileaflet (bicuspid valves are associated with higher paravalvular leak and conduction disturbance rates, though expanding evidence supports TAVR in bicuspid anatomy)
Valve Choice: TAVR vs SAVR by Risk Category
| Risk Category | Preferred Intervention | Key Evidence | Considerations |
|---|---|---|---|
| Prohibitive / extreme risk | TAVR (if anatomically suitable) | PARTNER 1B, CoreValve Extreme Risk | Palliative TAVR superior to medical therapy. Not all patients are suitable — assess futility. |
| High risk (STS ≥8%) | TAVR or SAVR (Heart Team decision) | PARTNER 1A, CoreValve High Risk, SURTAVI (expanded criteria) | TAVR non-inferior or superior to SAVR for 1–5 year outcomes. Transfemoral TAVR preferred access. |
| Intermediate risk (STS 4–8%) | TAVR or SAVR (Heart Team decision) | SURTAVI, PARTNER 2A | TAVR non-inferior. Patient age, anatomy, and preference guide choice. TAVR increasingly favoured in elderly. |
| Low risk (STS <4%) | SAVR or TAVR (individualised) | PARTNER 3, Evolut Low Risk | TAVR non-inferior/superior at 2 years. Long-term (>10 year) durability data for TAVR bioprostheses limited. SAVR preferred in younger patients (<65–70 years) for durability and potential future redo access. |
Bioprosthetic vs Mechanical Valve (SAVR)
For patients undergoing SAVR:
- Age ≥65 years: Bioprosthetic valve (bovine pericardial or porcine) is preferred. Avoids lifelong anticoagulation. SVD expected at 10–20 years.
- Age <65 years: Mechanical valve may be preferred if the patient accepts lifelong warfarin therapy. Superior durability. Shared decision-making is critical.
- Age <50 years: Consider the Ross procedure (pulmonary autograft) in selected patients at experienced centres.
Shared Decision-Making
The Heart Team discussion should incorporate:
- Life expectancy and quality of life goals
- Patient values regarding anticoagulation, reoperation risk, recovery time
- Anatomical suitability and procedural risks specific to the patient
- Cognitive status, frailty, and social support for post-procedural rehabilitation
- Patient preference after clear explanation of risks, benefits, and alternatives of both SAVR and TAVR
Asymptomatic Severe AS
Many patients with severe AS are initially asymptomatic. Current guidelines recommend watchful waiting with serial echocardiographic surveillance in most cases. However, certain high-risk features may warrant earlier intervention.
Surveillance Protocol
| AS Severity | Echo Frequency | Clinical Review |
|---|---|---|
| Severe (AVA ≤1.0 cm²) | Every 6–12 months | Every 6 months |
| Moderate (AVA 1.0–1.5 cm²) | Every 1–2 years | Every 12 months |
| Mild (AVA >1.5 cm²) | Every 3–5 years | As per routine |
Exercise Testing in Asymptomatic Severe AS
Exercise testing (symptom-limited treadmill or semi-supine bicycle echo) is recommended (Class IIa) in asymptomatic severe AS to unmask:
- Exertional symptoms (angina, dyspnoea, pre-syncope) — present in up to 30–40% of patients who report being asymptomatic
- Abnormal blood pressure response (failure of SBP to rise ≥20 mmHg or fall ≥20 mmHg from baseline)
- Exercise-induced ST changes or arrhythmias
A positive exercise test in asymptomatic severe AS confers significantly worse prognosis and supports early intervention.
Very Severe AS
Very severe AS is defined as AVA ≤0.6 cm² (or Vmax ≥5.0 m/s). These patients have a markedly worse natural history even when asymptomatic, with event rates of 20–40% per year. Current guidelines (ESC 2021, ACC/AHA 2020) support consideration of early intervention in very severe AS when performed at a centre with low operative mortality (<1–2% for SAVR, <3% for TAVR).
Rapid Progression
AS progression is variable. Rapid progression is defined as:
- Increase in Vmax ≥0.3 m/s per year
- Decrease in AVA ≥0.1 cm² per year
- Increase in mean gradient ≥7–10 mmHg per year
Rapid progression is associated with earlier symptom onset and worse outcomes. More frequent surveillance (every 6 months) is warranted, and earlier intervention may be justified.
Elevated Biomarkers
Elevated B-type natriuretic peptide (BNP) or NT-proBNP (>3× age- and sex-adjusted normal range) in asymptomatic severe AS is an independent predictor of symptom onset and adverse outcomes. Serial BNP monitoring can help identify subclinical LV decompensation. An increase in BNP >75 pg/mL (or NT-proBNP >300 pg/mL) from baseline supports consideration of earlier intervention, particularly when combined with other high-risk features.
High-sensitivity cardiac troponin (hs-cTn) elevation is also emerging as a prognostic marker in asymptomatic AS, reflecting ongoing myocardial injury from pressure overload. It is not yet standard of care for decision-making but adds to risk stratification.
Summary: When to Intervene in Asymptomatic Severe AS
| Feature | Recommendation | Class/Level |
|---|---|---|
| LVEF <50% (confirmed severe AS) | Intervention indicated | Class I / LOE B |
| Abnormal exercise test (symptoms or BP drop) | Intervention reasonable | Class IIa / LOE B |
| Very severe AS (AVA ≤0.6 cm²) at low surgical risk centre | Intervention reasonable | Class IIa / LOE C |
| Rapid progression (Vmax increase ≥0.3 m/s/year) | Intervention may be considered | Class IIb / LOE C |
| Elevated BNP (>3× normal) | Intervention may be considered | Class IIb / LOE C |
Post-Intervention Management
Lifelong follow-up is essential after valve intervention. Post-procedural management includes antithrombotic therapy, surveillance for complications, endocarditis prophylaxis counselling, and management of comorbidities.
Antithrombotic Therapy
Paravalvular Leak (PVL)
Paravalvular leak is more common after TAVR (10–25% mild, 2–5% moderate-to-severe) than SAVR (<5%).
- Mild PVL: Generally well-tolerated. Surveillance only. No specific treatment.
- Moderate PVL: Associated with increased mortality, heart failure, and haemolytic anaemia. Echocardiographic surveillance at 1, 6, and 12 months, then annually. Consider percutaneous closure if symptomatic or progressive.
- Severe PVL: Requires intervention. Percutaneous PVL closure (with Amplatzer Vascular Plug or dedicated PVL devices) is the first-line approach. Redo surgery carries high mortality risk and is reserved for cases not amenable to percutaneous closure.
Haemolytic anaemia secondary to PVL should be investigated with FBC, reticulocyte count, LDH, haptoglobin, and peripheral blood film. Erythropoietin-stimulating agents and iron supplementation may be required; definitive treatment is PVL closure.
Structural Valve Deterioration (SVD)
All bioprosthetic valves (surgical and transcatheter) are subject to SVD over time.
| Valve Type | Expected SVD Timeline | Key Features |
|---|---|---|
| SAVR bioprosthetic | 10–20 years (age-dependent; younger patients → faster SVD) | Stenosis predominant in younger patients; regurgitation predominant in older patients |
| TAVR bioprosthetic | Data emerging; 5-year durability appears comparable to SAVR; 10+ year data limited | May be less prone to SVD due to supra-annular positioning and newer designs |
| Mechanical valve | Virtually unlimited durability | Requires lifelong anticoagulation. Thrombotic obstruction is the primary long-term failure mode. |
SVD is defined using the Valve Academic Research Consortium (VARC-3) criteria as haemodynamic deterioration (increase in mean gradient ≥10 mmHg from post-implant baseline and/or new or worsening regurgitation ≥ moderate) with or without clinical consequences. Management options include redo SAVR, TAVR-in-TAVR (valve-in-valve), or TAVR-in-SAVR.
Follow-Up Protocol
Endocarditis Prophylaxis
The Australian Therapeutic Guidelines and the 2020 AHA/ACC guidelines recommend antibiotic prophylaxis for infective endocarditis in patients with prosthetic heart valves (including TAVR prostheses) undergoing high-risk dental procedures (dental extractions, periodontal procedures, dental implant placement). Recommend good oral hygiene and regular dental review for all prosthetic valve recipients.
Investigations
Essential and Supplementary Investigations
Special Populations
Pregnancy
Paediatrics
Elderly (>80 years)
Renal Impairment
Hepatic Impairment
Immunocompromised
Aboriginal and Torres Strait Islander Health Considerations
Quick Reference: Antithrombotic Therapy Post-Valve Intervention
📚 References
- 1. Otto CM, Nishimura RA, Bonow RO, et al. 2020 ACC/AHA Guideline for the Management of Patients With Valvular Heart Disease. Circulation. 2021;143(5):e72–e227.
- 2. Vahanian A, Beyersdorf F, Praz F, et al. 2021 ESC/EACTS Guidelines for the management of valvular heart disease. Eur Heart J. 2022;43(7):561–632.
- 3. Leon MB, Smith CR, Mack MJ, et al. Transcatheter or Surgical Aortic-Valve Replacement in Intermediate-Risk Patients. N Engl J Med. 2016;374(17):1609–1620. (PARTNER 2A)
- 4. Reardon MJ, Van Mieghem NM, Popma JJ, et al. Surgical or Transcatheter Aortic-Valve Replacement in Intermediate-Risk Patients. N Engl J Med. 2017;376(14):1321–1331. (SURTAVI)
- 5. Mack MJ, Leon MB, Thourani VH, et al. Transcatheter Aortic-Valve Replacement with a Balloon-Expandable Valve in Low-Risk Patients. N Engl J Med. 2019;380(18):1695–1705. (PARTNER 3)
- 6. Popma JJ, Deeb GM, Yakubov SJ, et al. Transcatheter Aortic-Valve Replacement with a Self-Expanding Valve in Low-Risk Patients. N Engl J Med. 2019;380(18):1706–1715. (Evolut Low Risk)
- 7. Pibarot P, Dumesnil JG. Low-flow, low-gradient aortic stenosis with normal and depressed left ventricular ejection fraction. J Am Coll Cardiol. 2012;60(19):1845–1853.
- 8. Clavel MA, Messika-Zeitoun D, Pibarot P, et al. The complex nature of discordant severe calcified aortic valve disease grading. J Am Coll Cardiol. 2013;62(24):2329–2338.
- 9. Baumgartner H, Falk V, Bax JJ, et al. 2017 ESC/EACTS Guidelines for the management of valvular heart disease (updated). Eur Heart J. 2017;38(36):2739–2791.
- 10. RHDAustralia (ARF/RHD writing group). National Agreement Guidelines for the Prevention, Diagnosis and Management of Acute Rheumatic Fever and Rheumatic Heart Disease in Australia. 3rd ed. Darwin: Menzies School of Health Research; 2020.
- 11. Australian Institute of Health and Welfare (AIHW). Cardiovascular disease in Australia 2024. AIHW; 2024.
- 12. Capodanno D, Petronio AS, Prendergast B, et al. Standardized definitions of structural valve deterioration and clinical endpoints for transcatheter and surgical bioprosthetic aortic valves. Eur Heart J. 2022;43(28):2638–2652. (VARC-3)
- 13. Van Mieghem NM, Unbehaun A, Piazza N, et al. Edoxaban versus standard anticoagulation after transcatheter aortic valve implantation: the ATLANTIS trial. J Am Coll Cardiol. 2021;78(24):2426–2436.
- 14. Saito Y, Watanabe M, Kaneko H, et al. Apixaban versus warfarin after transcatheter aortic valve implantation: the ENVISAGE-TAVI AF trial. N Engl J Med. 2021;385(23):2113–2124.
- 15. Heart Foundation of Australia. Position Statement: Aortic Valve Stenosis. Sydney: Heart Foundation; 2022.