📋 Key Information Summary
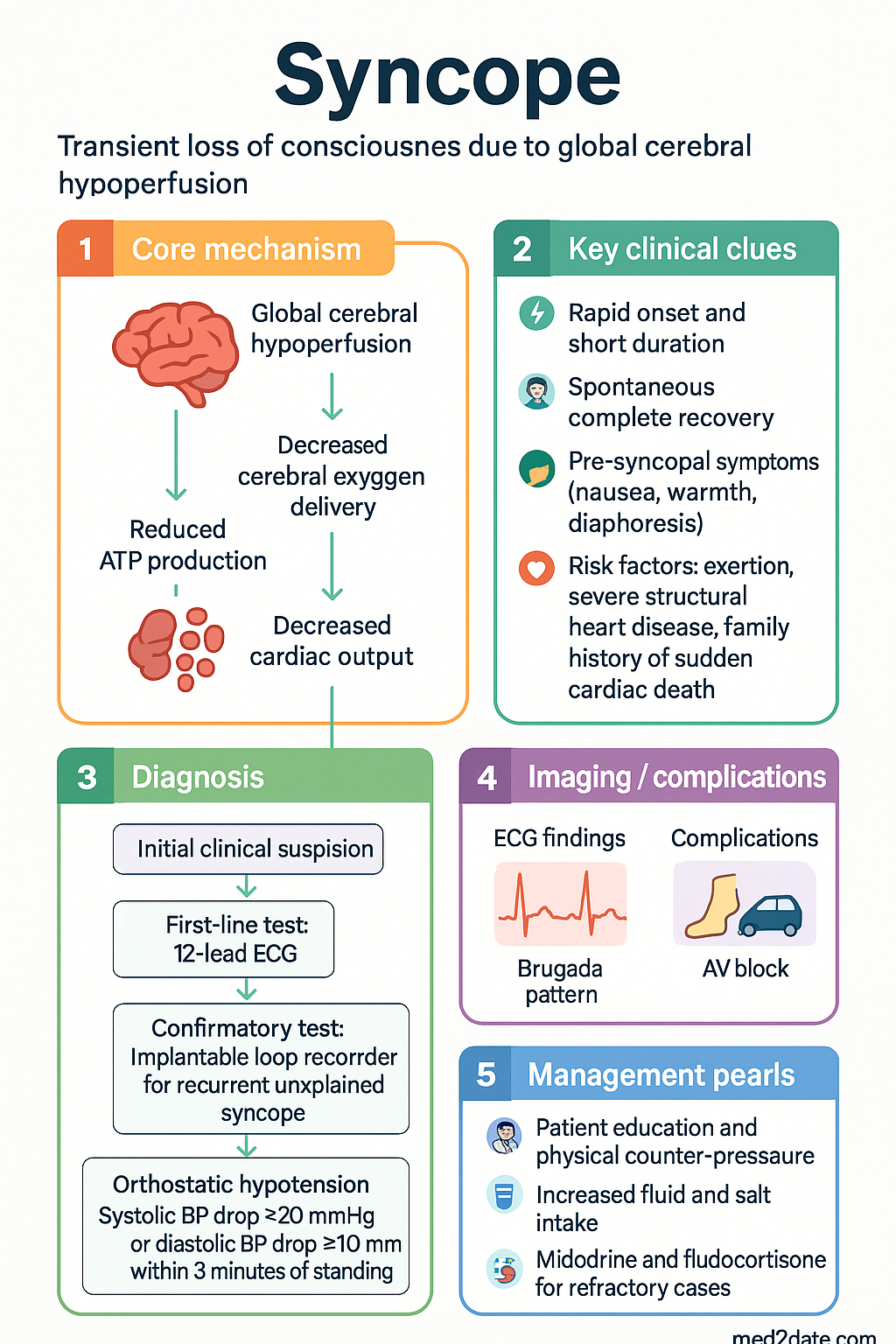
- Syncope is a transient loss of consciousness (TLOC) due to global cerebral hypoperfusion, with rapid onset, short duration, and spontaneous complete recovery.
- Affects approximately 3.5% of the Australian population; accounts for 1–3% of all emergency department presentations and up to 6% of acute medical admissions.
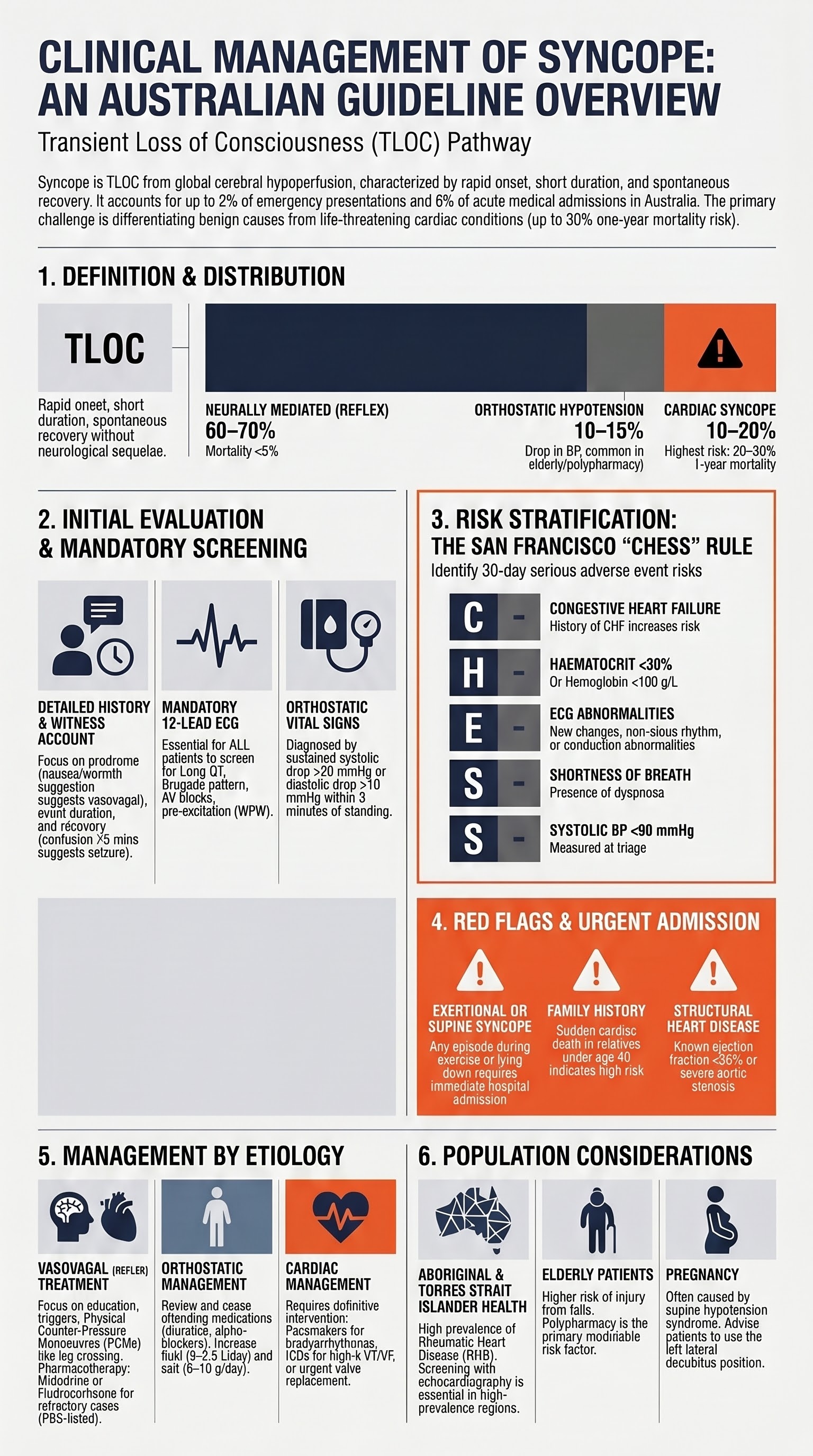
- Neurally mediated (vasovagal) syncope is the most common aetiology (60–70%), followed by orthostatic hypotension (10–15%) and cardiac syncope (10–20%).
- A 12-lead ECG is mandatory for all patients presenting with syncope — look for long QT, Brugada pattern, AV block, pre-excitation, and arrhythmia.
- High-risk features requiring hospital admission include: syncope during exertion, new-onset chest pain, severe structural heart disease, family history of sudden cardiac death under age 40, and ECG abnormalities.
- The San Francisco Syncope Rule and Canadian Syncope Risk Score are validated tools to stratify 30-day serious adverse events.
- Orthostatic hypotension is diagnosed by a sustained drop in systolic BP ≥20 mmHg or diastolic BP ≥10 mmHg within 3 minutes of standing.
- Implantable loop recorders (ILR) are recommended for recurrent unexplained syncope with negative initial workup — they detect intermittent arrhythmias in up to 50% of cases.
- First-line management of vasovagal syncope includes patient education, physical counter-pressure manoeuvres (leg crossing, squatting), and increased fluid (2–2.5 L/day) and salt intake (6–10 g/day).
- Midodrine (alpha-1 agonist) and fludrocortisone are second-line pharmacological options for refractory orthostatic hypotension and vasovagal syncope — both PBS-listed.
- Cardiac syncope carries the highest mortality risk (up to 30% 1-year mortality) and requires urgent cardiology assessment and definitive treatment (pacemaker, ICD, or catheter ablation).
- Aboriginal and Torres Strait Islander Australians have higher rates of rheumatic heart disease and structural cardiac causes of syncope, requiring culturally appropriate assessment and reduced referral barriers.
Introduction & Australian Epidemiology
Syncope is defined as transient loss of consciousness (TLOC) due to transient global cerebral hypoperfusion, characterised by rapid onset, short duration, and spontaneous and complete recovery without neurological sequelae. It must be distinguished from other causes of TLOC including epileptic seizures, psychogenic pseudosyncope, concussion, vertebrobasilar transient ischaemic attacks, and metabolic disturbances such as hypoglycaemia.
In Australia, syncope accounts for approximately 1–3% of all emergency department (ED) presentations, with an estimated incidence of 6.2 per 1,000 person-years. It is the cause of approximately 6% of acute medical admissions nationally. Lifetime prevalence is estimated at 3.5% of the general population, with a peak in adolescents and young adults (vasovagal type) and in those over 65 years (orthostatic and cardiac causes).
The economic burden of syncope in Australia is substantial, with average inpatient costs of ,500–,000 per admission. Recurrent syncope significantly impairs quality of life, with physical injury occurring in 6–30% of events (fractures in 5%, motor vehicle accidents if driving at onset).
Aetiology Distribution in Australian Practice
| Category | Prevalence | Examples | 1-Year Mortality |
|---|---|---|---|
| Neurally mediated (reflex) | 60–70% | Vasovagal, situational (cough, micturition, defecation), carotid sinus hypersensitivity | <5% |
| Orthostatic hypotension | 10–15% | Drug-induced, autonomic failure, dehydration, volume depletion | 5–10% |
| Cardiac (arrhythmic) | 10–15% | Bradyarrhythmias, SVT, VT, long QT, Brugada, WPW | 20–30% |
| Cardiac (structural) | 3–5% | Aortic stenosis, HOCM, pulmonary embolism, aortic dissection | 20–30% |
| Unexplained | 10–15% | After comprehensive evaluation | 5–10% |
Initial Evaluation
The initial evaluation of syncope is critical to differentiate benign causes from life-threatening conditions. A systematic approach combining thorough history, physical examination, orthostatic vital signs, and a resting 12-lead ECG will identify the likely aetiology in the majority of patients and guide disposition.
History and Physical Examination
The history is the single most important diagnostic tool in syncope evaluation and provides diagnostic clues in up to 50% of cases. Key elements to elicit include:
Focused Physical Examination
- Cardiovascular: Heart rate and rhythm, blood pressure (both arms), murmurs (aortic stenosis, HOCM), radio-femoral delay (coarctation), jugular venous pressure
- Neurological: Focal deficits (suggest structural brain disease, not syncope), cognition, speech
- Orthostatic vital signs: Measured using active standing protocol (see below)
- Carotid sinus massage: Only in patients >40 years with unexplained syncope, under continuous monitoring, excluding those with carotid bruit, recent stroke/TIA (<3 months), or ventricular tachyarrhythmias
Orthostatic Vital Signs
Orthostatic vital signs should be measured in all patients presenting with syncope unless there is an obvious cause (e.g., witnessed vasovagal episode in a young, healthy patient). The active standing test is the preferred method.
- Patient lies supine for ≥5 minutes
- Record supine BP and HR
- Patient stands; BP and HR recorded at 1, 3, and 5 minutes
- Record symptoms during standing
- Test in the morning before medications when possible
- Orthostatic hypotension: Systolic BP drop ≥20 mmHg OR diastolic BP drop ≥10 mmHg within 3 minutes of standing
- Initial orthostatic hypotension: BP drop within 15 seconds of standing with rapid recovery
- Delayed orthostatic hypotension: BP drop occurs after 3 minutes of standing
- Postural tachycardia syndrome (POTS): HR increase ≥30 bpm within 10 minutes of standing without BP drop (age 12–19: ≥40 bpm)
12-Lead ECG — Mandatory
ECG Findings Requiring Urgent Evaluation
| Finding | Significance | Action |
|---|---|---|
| Bifascicular block (LBBB or RBBB + LAFB/LPFB) | Risk of progression to complete heart block | Cardiology admission, consider pacing |
| Second-degree type II or third-degree AV block | Indicates infra-nodal conduction disease | Urgent cardiology, pacing |
| Prolonged QTc (>500 ms or >480 ms with symptoms) | Risk of Torsades de Pointes | Electrolytes, medication review, cardiology |
| Brugada pattern (type 1 ST elevation V1–V3) | Risk of ventricular fibrillation | Urgent electrophysiology referral |
| Pre-excitation (delta wave, short PR) | Wolff-Parkinson-White — risk of sudden cardiac death with atrial fibrillation | Electrophysiology referral for ablation |
| Sustained or non-sustained ventricular tachycardia | Likely cause of syncope | Cardiology admission, ICD evaluation |
| New ischaemic changes (ST depression/elevation, T-wave inversion) | Acute coronary syndrome as precipitant | Troponin, cardiology, ACS pathway |
| Deep Q waves (inferior leads) | Prior MI; ventricular scar substrate for VT | Echocardiography, cardiology review |
High-Risk Features Warranting Hospital Admission
- Syncope during exertion or while supine
- New-onset or severe chest pain, dyspnoea, or palpitations
- Severe structural heart disease (ejection fraction <35%, severe aortic stenosis, HOCM)
- Family history of sudden cardiac death (age <40) or inherited channelopathy/arrhythmia syndrome
- Significant ECG abnormalities (see table above)
- Syncope resulting in significant injury
- Persistent abnormal vital signs (hypotension, tachycardia, hypoxia)
- Age >65 with first episode and no clear vasovagal cause
Risk Stratification
Risk stratification in syncope aims to identify patients at risk of 30-day serious adverse events (SAE), including death, myocardial infarction, arrhythmia, pulmonary embolism, aortic dissection, subarachnoid haemorrhage, and significant haemorrhage requiring transfusion. Several validated tools assist in disposition decision-making in the Australian ED setting.
San Francisco Syncope Rule (SFSR)
The San Francisco Syncope Rule identifies patients at risk of serious outcomes at 30 days. It was originally developed by Quinn et al. (2004) and has been externally validated in Australian populations. The rule uses the mnemonic "CHESS":
- C — History of Congestive heart failure
- H — Haematocrit <30% (Hb <100 g/L)
- E — Abnormal ECG (new changes, non-sinus rhythm, any conduction abnormality)
- S — Shortness of breath (dyspnoea)
- S — Systolic BP <90 mmHg at triage
ROSE Criteria (Risk Stratification Of Syncope in the Emergency Department)
The ROSE criteria were developed by Reed et al. (2010) and focus on identifying patients at risk of 30-day serious outcomes including death and cardiac arrhythmia:
- BRain natriuretic peptide (BNP) ≥300 pg/mL
- ECG with Q-wave (not in lead III)
- Oxygen saturation ≤94% on room air
- Systolic BP ≤90 mmHg at triage or in ED
- Blood on rectal examination / faecal occult blood positive / active haemorrhage
- Smoker or history of cardiovascular disease / diabetes
Interpretation: ≥1 criterion → high risk (sensitivity 87–90%, specificity 65%). BNP ≥300 pg/mL is the single strongest predictor. Useful when BNP is available (most Australian EDs can process BNP within 1–2 hours).
Canadian Syncope Risk Score (CSRS)
The Canadian Syncope Risk Score (Thiruganasambandamoorthy et al., 2016, JAMA) is the most robustly validated clinical decision tool and is increasingly used in Australian tertiary EDs. It stratifies patients into low, medium, and high-risk categories for 30-day SAE.
| CSRS Predictor | Points |
|---|---|
| Predisposition to vasovagal symptoms (warm/crowded environment, prolonged standing, fear, emotional stress, pain) | −1 |
| History of heart disease (CAD, CHF, valvular, arrhythmia) | +1 |
| Any systolic BP <90 or >180 mmHg in ED | +2 |
| Troponin above 99th percentile (high-sensitivity troponin) | +2 |
| Abnormal QRS axis (<−30° or >100°) | +1 |
| QRS duration >130 ms | +1 |
| QTc interval >480 ms (corrected for heart rate) | +2 |
| Diagnosis of vasovagal syncope in ED | −2 |
| Diagnosis of cardiac syncope in ED | +2 |
Diagnostic Testing
Diagnostic testing beyond the initial evaluation (history, examination, orthostatic vitals, ECG) is guided by clinical suspicion. The majority of tests are directed at confirming or excluding cardiac syncope, which carries the highest morbidity and mortality. Testing should follow a stepwise approach — invasive testing is reserved for cases where non-invasive investigation has been exhausted or clinical suspicion is high.
Investigations Overview
Tilt Table Testing — Detailed Protocol
The tilt table test is the primary investigation for confirming neurally mediated (vasovagal) syncope when clinical features are atypical or when recurrent episodes warrant a definitive diagnosis. The test evaluates the cardiovascular response to prolonged upright posture.
Response Patterns on Tilt Table Testing
| Vasovagal Response Type | Haemodynamic Pattern | Treatment Implication |
|---|---|---|
| Type 1 (mixed) | BP drops, HR falls but does not reach <40 bpm or lasts <10 s without asystole | Volume expansion, counter-pressure manoeuvres |
| Type 2A (cardioinhibitory without asystole) | HR <40 bpm for ≥10 s but no asystole >3 s; BP drops before HR falls | Pacing rarely needed; pharmacotherapy + counter-pressure |
| Type 2B (cardioinhibitory with asystole) | Asystole >3 s; HR drops before or simultaneous with BP drop | Consider cardiac pacing in recurrent, injury-prone cases |
| Type 3 (vasodepressor) | BP drops without significant HR fall (<10% from peak) | Midodrine, fludrocortisone, volume expansion |
| POTS pattern | HR increase ≥30 bpm within 10 min (≥40 bpm age 12–19) without hypotension | Exercise training, volume/salt, low-dose beta-blocker, ivabradine |
Ambulatory Monitoring Strategy
The choice of ambulatory monitoring depends on the frequency of syncope episodes and the pre-test probability of an arrhythmic aetiology:
| Monitoring Duration | Device | Diagnostic Yield | Indication |
|---|---|---|---|
| 24–48 hours | Holter monitor | 1–2% | Daily or near-daily symptoms |
| 7–30 days | External event recorder (e.g., Ziopatch™) | 15–25% | Weekly to monthly symptoms |
| Up to 3 years | Implantable loop recorder (ILR) | 33–50% at 12 months | Infrequent recurrence (<monthly), negative initial workup |
Management by Etiology
Treatment of syncope is directed at the underlying cause. The major therapeutic categories include non-pharmacological interventions for neurally mediated syncope, volume management and pharmacotherapy for orthostatic hypotension, and definitive cardiac interventions for cardiac arrhythmia or structural disease.
Neurally Mediated (Vasovagal) Syncope
Vasovagal syncope is the most common cause and is generally benign, but recurrent episodes can significantly impair quality of life and cause injury. Treatment follows a stepwise approach from conservative measures through to pharmacotherapy and, rarely, pacing.
Step 1: Patient Education and Reassurance
- Explain the benign nature and mechanism of vasovagal syncope — reduces anxiety and healthcare utilisation
- Identify and avoid triggers: prolonged standing, warm environments, dehydration, alcohol, fasting
- Increase fluid intake to 2–2.5 L per day
- Increase dietary salt intake to 6–10 g per day (approximately 1–2 additional teaspoons) unless contraindicated (heart failure, renal impairment, hypertension)
- Gradual positional changes — avoid sudden standing from supine/sitting
Step 2: Physical Counter-Pressure Manoeuvres (PCMs)
PCMs are first-line physical interventions effective at aborting or delaying vasovagal episodes when a prodrome is present. They work by increasing venous return and cardiac output through muscle contraction:
- Leg crossing with muscle tensing: Cross legs and squeeze thighs together + clench buttocks and abdominal muscles. Most effective PCM, increases systolic BP by 20–40 mmHg
- Squatting: Rapidly squat when prodromal symptoms occur. Increases preload via compression of leg veins
- Arm tensing: Grip one hand in the other and pull (isometric arm contraction). Useful when leg manoeuvres are not feasible (e.g., seated)
- PCMs should be taught and practised during clinic visits — patient education handouts available from the Cardiac Society of Australia and New Zealand (CSANZ)
Step 3: Tilt Training
Standing practice against a wall for 15–30 minutes daily, gradually increasing duration. Evidence is mixed but may benefit highly motivated patients with recurrent vasovagal syncope. A meta-analysis showed a 60–70% reduction in syncope frequency.
Step 4: Pharmacotherapy for Refractory Cases
Step 5: Cardiac Pacing for Vasovagal Syncope
Orthostatic Hypotension
Orthostatic hypotension (OH) is a common cause of syncope in the elderly and those on multiple medications. Management addresses reversible causes first, then non-pharmacological measures, and finally pharmacotherapy.
Step 1: Identify and Correct Reversible Causes
- Medication review: Reduce or cease offending agents — antihypertensives (especially alpha-blockers such as prazosin/doxazosin, vasodilating beta-blockers, diuretics, nitrates), antidepressants (TCAs, MAOIs, SSRIs), antipsychotics, opioids, dopaminergic agents. Coordinate with GP for gradual dose reduction.
- Volume depletion: Correct dehydration (GI losses, diuretic excess, reduced intake). Assess fluid status clinically and with UEC (raised urea:creatinine ratio suggests pre-renal).
- Autonomic neuropathy: Consider diabetes mellitus (most common cause of autonomic neuropathy in Australia), amyloidosis, Parkinson's disease, pure autonomic failure, multiple system atrophy
Step 2: Non-Pharmacological Interventions
- Increase fluid intake: 2–2.5 L/day
- Increase salt intake: 6–10 g/day (contraindicated in heart failure, renal failure, hypertension)
- Sleep with head of bed elevated 10–20° (reduces nocturnal polyuria, attenuates supine hypertension)
- Avoid sudden postural changes; stand slowly from lying/sitting
- Physical counter-pressure manoeuvres (as above)
- Compression stockings (thigh-high, 30–40 mmHg) — evidence limited but commonly used; abdominal binders may be more effective for those with predominant splanchnic pooling
- Small, frequent meals (reduces post-prandial hypotension)
Step 3: Pharmacotherapy
Cardiac Syncope
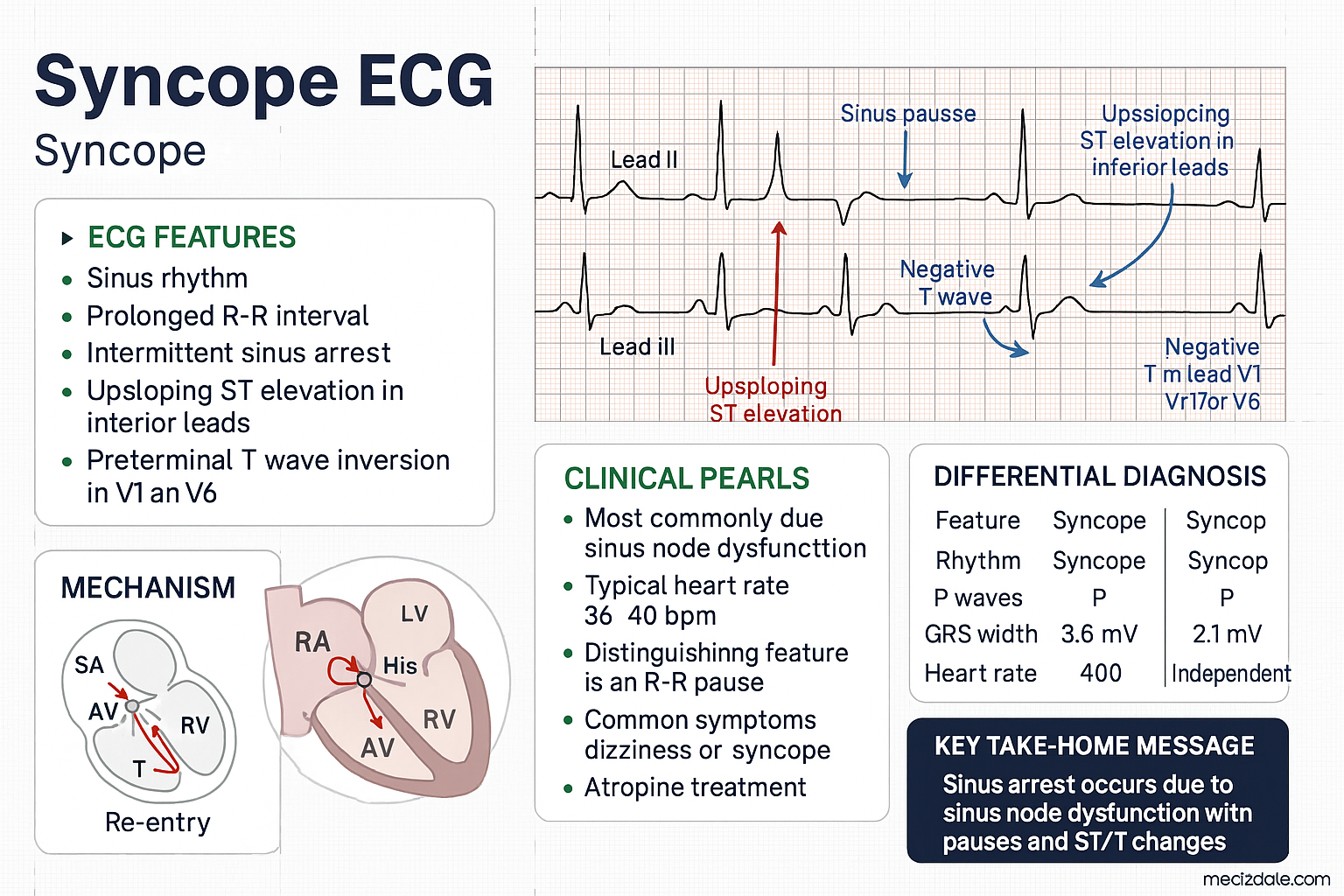
Bradyarrhythmias (Sinus Node Dysfunction, AV Block)
- Symptomatic sinus node dysfunction with documented bradycardia (HR <40 bpm) and syncope → permanent pacemaker implantation
- Second-degree type II AV block or third-degree (complete) AV block → permanent pacemaker (dual-chamber, DDD mode preferred)
- Atropine 0.5–1 mg IV for acute symptomatic bradycardia (temporary measure)
- Transcutaneous pacing for haemodynamically unstable bradycardia while awaiting transvenous pacing
- MBS item 38300 (permanent pacemaker insertion, dual-chamber). Available at all tertiary and many regional hospitals in Australia.
Supraventricular Tachycardia (SVT)
- Acute management: vagal manoeuvres (Valsalva, carotid sinus massage) → IV adenosine 6 mg rapid push (12 mg if first dose fails, may repeat 12 mg). Flush immediately with 20 mL NS.
- Long-term: catheter ablation (curative in 90–95% of AVNRT and AVRT/WPW). Referral to electrophysiology.
- Pharmacological rate/rhythm control if ablation not desired: flecainide, sotalol, or beta-blockers
Ventricular Tachycardia (VT) and Ventricular Fibrillation
- Haemodynamically unstable VT / VF: Immediate synchronised cardioversion (biphasic 120–200 J) or defibrillation. ACLS protocol.
- Stable sustained monomorphic VT: IV amiodarone 150 mg over 10 minutes (may repeat once) → consider procainamide 20–50 mg/min up to 17 mg/kg if amiodarone fails.
- Long-term VT management with reduced LVEF: ICD (implantable cardioverter-defibrillator) implantation for secondary prevention of sudden cardiac death (SCD). MBS item 38326 (ICD insertion).
- ICD implantation indications in syncope: documented VT/VF, LVEF ≤35% with NYHA II–III after ≥3 months of optimal medical therapy (primary prevention), or unexplained syncope with inducible VT at EPS in setting of structural heart disease.
- Catheter ablation: Increasingly used for VT substrate ablation (especially in ischaemic cardiomyopathy with recurrent VT). Refer to electrophysiology at a tertiary centre.
Structural Cardiac Causes
- Aortic stenosis: Syncope with critical aortic stenosis (valve area <1.0 cm²) requires urgent surgical or transcatheter aortic valve replacement (TAVI/SAVR). MBS item 38426 (TAVI). Refer to structural heart disease team.
- Hypertrophic cardiomyopathy (HOCM): Avoid dehydration, intense exertion, Valsalva. Beta-blockers (metoprolol or atenolol) or verapamil first-line. ICD if high-risk features (syncope, NSVT, family history SCD, maximal wall thickness ≥30 mm, LV apical aneurysm, extensive late gadolinium enhancement on CMR). Septal myectomy/alcohol ablation for refractory obstruction.
- Pulmonary embolism: Syncope may be the presenting feature of massive PE. CT pulmonary angiography if suspected. Anticoagulation (apixaban or rivaroxaban) or thrombolysis (alteplase) for massive PE with haemodynamic instability.
- Aortic dissection: Syncope with severe tearing chest/back pain, pulse differential, and aortic regurgitation murmur. CT aortogram urgent. Emergency surgical repair for Type A; medical management with IV esmolol/labetalol for Type B.
Volume Repletion
Volume repletion is a cornerstone of acute and chronic management for syncope related to hypovolaemia, orthostatic hypotension, and neurally mediated syncope:
- Acute intravenous fluids: 500 mL 0.9% sodium chloride (normal saline) over 30–60 minutes for acute hypovolaemic syncope. Reassess haemodynamic response — avoid excessive fluid administration in elderly patients with heart failure. Hartmann's solution (compound sodium lactate) is a reasonable alternative.
- Chronic oral fluid intake: Target 2–2.5 L/day of non-caffeinated fluids. Water bolus drinking (500 mL water over 5 minutes, consumed 30 minutes before prolonged standing) increases systolic BP by 20–30 mmHg via sympathetic activation — a simple, evidence-based intervention.
- Dietary salt supplementation: 6–10 g NaCl/day for neurally mediated syncope and orthostatic hypotension (equivalent to approximately 2.4–4 g sodium/day). Salt tablets (1 g NaCl each) may be used — available without prescription. Contraindicated in heart failure (NYHA III–IV), chronic kidney disease (eGFR <30), and hypertension (BP >160/100).
Special Populations
Pregnancy
Paediatrics
Elderly (>65 Years)
Renal Impairment
Hepatic Impairment
Immunocompromised
Aboriginal and Torres Strait Islander Health
Aboriginal and Torres Strait Islander Australians experience a significantly higher burden of cardiovascular disease compared with non-Indigenous Australians. Syncope in this population requires particular attention to structural cardiac causes, rheumatic heart disease, and barriers to accessing specialist diagnostic services, particularly in remote and very remote communities.
Epidemiological Considerations
- Aboriginal and Torres Strait Islander Australians have 2–3 times the rate of cardiovascular mortality compared with non-Indigenous Australians (AIHW, 2023).
- Acute rheumatic fever (ARF) and rheumatic heart disease (RHD) remain endemic in northern and central Australia, disproportionately affecting Aboriginal and Torres Strait Islander communities. RHD can cause syncope through valvular obstruction, arrhythmia, or heart failure.
- Endocarditis is more prevalent in Aboriginal and Torres Strait Islander Australians, which can lead to valvular damage and subsequent syncope.
- CA-MRSA skin infections are more common in remote Aboriginal communities, which may indirectly relate to endocarditis risk through injection drug use or bacteraemia.
- Rheumatic heart disease-related syncope is disproportionately seen in Aboriginal and Torres Strait Islander patients aged 15–45 years, an age group where cardiac syncope is otherwise uncommon.
📚 References
- 1. Shen W-K, Sheldon RS, Benditt DG, et al. 2017 ACC/AHA/HRS Guideline for the Evaluation and Management of Patients With Syncope. J Am Coll Cardiol. 2017;70(5):e39–e110.
- 2. Brignole M, Moya A, de Lange FJ, et al. 2018 ESC Guidelines for the diagnosis and management of syncope. Eur Heart J. 2018;39(21):1883–1948.
- 3. Thiruganasambandamoorthy V, Kwong K, Wells GA, et al. Development of the Canadian Syncope Risk Score to predict serious adverse events after emergency department assessment of syncope. CMAJ. 2016;188(12):E289–E298.
- 4. Quinn JV, Stiell IG, McDermott DA, et al. Derivation of the San Francisco Syncope Rule to predict patients with short-term serious outcomes. Ann Emerg Med. 2004;43(2):224–232.
- 5. Reed MJ, Newby DE, Coull AJ, et al. The ROSE (Risk Stratification of Syncope in the Emergency Department) study. J Am Coll Cardiol. 2010;55(8):713–721.
- 6. Parry SW, Matthews IG. Implantable loop recorders in the investigation of unexplained syncope: state of the art. Intern Med J. 2010;40(10):674–681.
- 7. Brignole M, Donateo P, Tomaino M, et al. The benefit of pacemaker therapy in patients with presumed neurally mediated syncope presenting with syncope and documented asystole: the ISSUE-3 trial. Europace. 2014;16(6):851–857.
- 8. Sheldon R, Raj SR. Pacing and vasovagal syncope: back to our physiologic roots. Clin Auton Res. 2017;27(1):11–19.
- 9. Raj SR. Postural tachycardia syndrome (POTS). Circulation. 2013;127(23):2336–2342.
- 10. Australian Institute of Health and Welfare (AIHW). Cardiovascular disease in Aboriginal and Torres Strait Islander people. Canberra: AIHW; 2023.
- 11. RHDAustralia (ARF/RHD Program, Menzies School of Health Research). Australian guideline for prevention, diagnosis and management of acute rheumatic fever and rheumatic heart disease. 3rd ed. Darwin: RHDAustralia; 2020.
- 12. Heart Foundation of Australia. Position statement: Syncope assessment and management in the emergency department. Melbourne: Heart Foundation; 2019.
- 13. Raj SR, Coffin ST. Medical therapy and physical maneuvers in the treatment of the vasovagal syncope and orthostatic hypotension. Prog Cardiovasc Dis. 2013;55(4):425–433.
- 14. Moya A, Sutton R, Ammirati F, et al. Guidelines for the diagnosis and management of syncope (version 2009). Eur Heart J. 2009;30(21):2631–2671.
- 15. Cardiac Society of Australia and New Zealand (CSANZ). Guidelines for the management of arrhythmias in the emergency department. Sydney: CSANZ; 2022.