📋 Key Information Summary
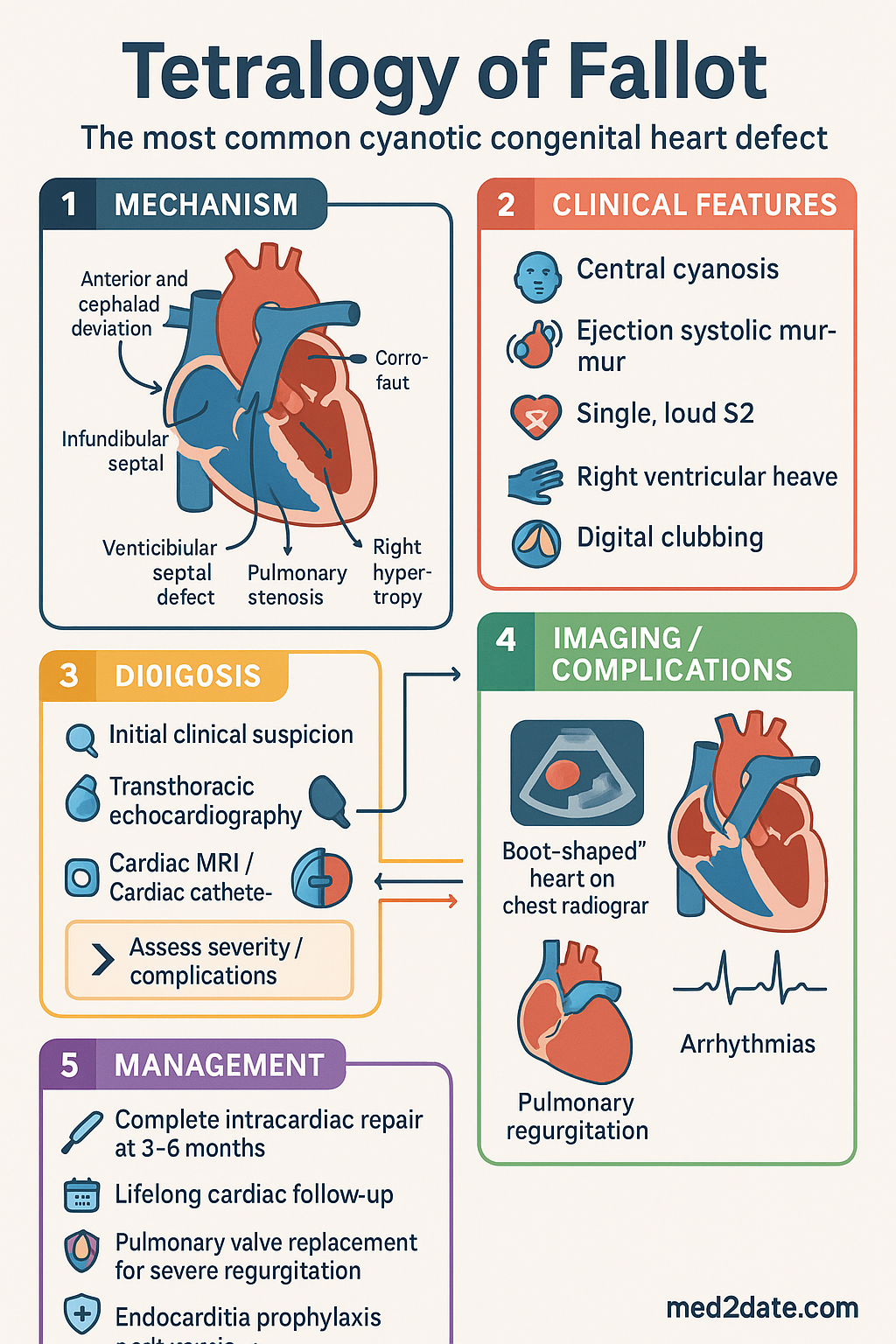
- Tetralogy of Fallot (TOF) is the most common cyanotic congenital heart defect, comprising four anatomical abnormalities: ventricular septal defect (VSD), overriding aorta, right ventricular outflow tract (RVOT) obstruction, and right ventricular hypertrophy (RVH).
- TOF accounts for approximately 7–10 % of all congenital heart disease and 50–75 % of cyanotic CHD in Australian registries.
- Cyanosis at birth depends on the degree of RVOT obstruction; severe obstruction produces early cyanosis, while mild obstruction may present later with acyanotic or "pink" TOF.
- Hypercyanotic ("Tet") spells are acute, life-threatening episodes of profound cyanosis requiring immediate intervention: knee-to-chest positioning, supplemental O₂, IV phenylephrine, and fluids.
- Transthoracic echocardiography (TTE) is the primary diagnostic tool; cardiac MRI and cardiac catheterisation are used for pre-operative and post-operative assessment.
- Complete intracardiac repair (closure of VSD and relief of RVOT obstruction) is typically performed at 3–6 months of age in Australia.
- Palliative Blalock–Taussig (BT) shunt may be performed in neonates with severe cyanosis or unfavourable anatomy pending definitive repair.
- Lifelong cardiac follow-up in a specialised Adult Congenital Heart Disease (ACHD) centre is mandatory; most patients develop pulmonary regurgitation, right ventricular dilatation, and/or arrhythmias post-repair.
- Pulmonary valve replacement (PVR) is indicated for symptomatic severe pulmonary regurgitation, RV dilatation (indexed RV end-diastolic volume >150 mL/m²), or sustained ventricular tachycardia.
- Endocarditis prophylaxis is recommended for at least 6 months post-repair and for residual defects.
- Pre-pregnancy counselling is essential; most repaired TOF patients tolerate pregnancy well, but residual lesions require risk stratification (mWHO class II–III).
- Aboriginal and Torres Strait Islander children have higher rates of late presentation and poorer access to paediatric cardiac surgery — early antenatal detection and culturally safe pathways are critical.
- Genetic counselling should be offered; 22q11.2 deletion (DiGeorge syndrome) is present in 15–20 % of TOF patients.
Introduction & Australian Epidemiology
Tetralogy of Fallot (TOF) is the most common cyanotic congenital heart disease, consisting of a ventricular septal defect (VSD), overriding aorta, pulmonary stenosis, and right ventricular hypertrophy. First described by Étienne-Louis Arthur Fallot in 1888, TOF remains one of the most frequently encountered congenital cardiac lesions in paediatric cardiology practice worldwide.
In Australia, the incidence of TOF is approximately 3–5 per 10 000 live births, accounting for 7–10 % of all congenital heart disease and up to 50–75 % of cyanotic CHD presentations. Data from the Australian and New Zealand Fontan Registry and state-based cardiac databases (e.g., the Victorian Paediatric Cardiac Surgery Programme) consistently place TOF among the top three lesions requiring neonatal or infant cardiac surgery.
Advances in surgical technique, perioperative care, and long-term follow-up have dramatically improved survival, with current operative mortality <2 % and >90 % survival to adulthood. However, late complications — pulmonary regurgitation, right ventricular dysfunction, atrial and ventricular arrhythmias, and sudden cardiac death — necessitate lifelong specialist surveillance in an Adult Congenital Heart Disease (ACHD) centre.
TOF is associated with 22q11.2 microdeletion syndrome (DiGeorge syndrome) in 15–20 % of cases, highlighting the importance of genetic testing and counselling for all affected families.
Anatomy & Pathophysiology
The Four Components
Tetralogy of Fallot results from anterior and cephalad deviation of the infundibular septum during embryological development, producing the following four interrelated anatomical abnormalities:
| Component | Description | Haemodynamic Consequence |
|---|---|---|
| Ventricular Septal Defect (VSD) | Large, malalignment-type perimembranous VSD with anterior deviation of the outlet septum | Equalisation of LV and RV pressures; obligatory shunt determined by RVOT obstruction severity |
| Overriding Aorta | Aortic root overrides the VSD, receiving blood from both ventricles | Right-to-left shunting of deoxygenated blood into the systemic circulation |
| RVOT Obstruction / Pulmonary Stenosis | Infundibular (dynamic) ± valvular ± supravalvular pulmonary stenosis | Degree of obstruction determines pulmonary blood flow and thus degree of cyanosis |
| Right Ventricular Hypertrophy | Secondary to RV pressure overload from RVOT obstruction | May lead to diastolic dysfunction, fibrosis, and eventually RV failure |
Haemodynamic Spectrum
The clinical phenotype of TOF spans a broad spectrum depending on the severity of RVOT obstruction:
- Severe obstruction: Marked right-to-left shunting → profound cyanosis from birth → "blue" TOF. Pulmonary blood flow is severely reduced.
- Moderate obstruction: Balanced shunting → mild-to-moderate cyanosis → progressive cyanosis over weeks to months.
- Mild obstruction ("Pink TOF"): Left-to-right shunting predominates → minimal cyanosis at rest → resembles large VSD; may develop cyanosis with crying, feeding, or exercise.
- TOF with pulmonary atresia: Extreme form with no antegrade pulmonary blood flow — pulmonary circulation dependent on a patent ductus arteriosus (PDA) or major aortopulmonary collateral arteries (MAPCAs).
Associated Lesions and Genetic Associations
Several anatomical variants and associated lesions are recognised:
- Absent pulmonary valve syndrome (TOF-APV) — aneurysmal dilatation of pulmonary arteries, airway compression
- Atrioventricular septal defect (AVSD) — particularly in Down syndrome
- Right-sided aortic arch — present in ~25 % of TOF cases
- Coronary artery anomalies (e.g., left anterior descending from right coronary artery) — critical for surgical planning
- 22q11.2 deletion (DiGeorge / velocardiofacial syndrome) — 15–20 % of TOF patients; requires FISH or microarray testing
- Trisomy 21 (Down syndrome) — higher prevalence of TOF with AVSD
Clinical Features & Tet Spells
Presentation
The presentation of TOF varies with the degree of pulmonary stenosis:
Key Examination Findings
- Central cyanosis (lips, tongue) — may be subtle in mild cases; prominent with crying
- Ejection systolic murmur — left upper sternal border, grade varies inversely with severity
- Single, loud S2 (aortic component)
- Right ventricular heave (palpable)
- Digital clubbing — late finding in unrepaired or palliated TOF (months to years)
- Squatting posture in toddlers — increases SVR, reduces right-to-left shunt (classic but less seen in modern practice)
Hypercyanotic ("Tet") Spells
Triggers: Crying, straining (defecation, feeding), dehydration, fever, anaemia, catecholamine surge.
Pathophysiology: Acute infundibular spasm → increased RVOT obstruction → right-to-left shunt ↑ → systemic desaturation → acidosis → further infundibular spasm (vicious cycle).
Emergency Management of a Tet Spell
Prophylaxis Against Tet Spells
- Oral propranolol 1–3 mg/kg/day divided BD–TDS — reduces infundibular spasm by blunting catecholamine response; used as a bridge to surgery
- Maintain adequate hydration and iron stores; treat anaemia promptly
- Antipyretics for fever
- Avoid dehydration, vigorous crying (feed regularly), and abrupt SVR reduction
Investigations & Diagnosis
Antenatal Detection
Fetal echocardiography at 18–22 weeks gestation can identify TOF in many cases. The four-chamber view may appear normal; the outflow-tract view demonstrates the overriding aorta and VSD. Detection rates vary with operator experience and maternal factors. Antenatal diagnosis facilitates planned delivery at a tertiary centre with paediatric cardiac surgery capability.
Postnatal Investigations
Differential Diagnosis
| Condition | Distinguishing Features |
|---|---|
| Transposition of the Great Arteries (TGA) | Severe cyanosis from day 1, usually no murmur at birth, "egg-on-a-string" CXR, parallel great arteries on echo |
| Total Anomalous Pulmonary Venous Connection (TAPVC) | Cyanosis with pulmonary venous obstruction, "snowman" CXR, dilated RV on echo |
| Tricuspid Atresia | Absent tricuspid valve, right axis deviation, left ventricular dominance on echo |
| Ebstein Anomaly | Atrialised RV, "wall-to-wall" heart on CXR, severe tricuspid regurgitation |
| Large VSD with Eisenmenger | No RVOT obstruction; progressive pulmonary hypertension, late cyanosis (typically adolescence/adult) |
Surgical Repair & Long-term Management
Surgical Strategies
1. Palliative: Modified Blalock–Taussig (BT) Shunt
Indicated in neonates or young infants who are not candidates for early complete repair due to:
- Very low birth weight (<2.5 kg)
- Unfavourable coronary anatomy (LAD from RCA)
- Hypoplastic pulmonary arteries
- TOF with pulmonary atresia requiring staged repair
- Multiple associated anomalies or non-cardiac comorbidities
Procedure: Goretex® (PTFE) interposition graft (3.5–4 mm) between subclavian artery and ipsilateral pulmonary artery. Provides reliable pulmonary blood flow, allowing growth prior to complete repair.
Complications: Shunt thrombosis (acute cyanosis), pulmonary overcirculation, distortion of pulmonary artery, chylothorax.
2. Primary Complete Repair
The standard of care in Australia. Typically performed at 3–6 months of age via median sternotomy with cardiopulmonary bypass (CPB) and cardioplegic arrest.
Immediate Post-operative Care
- Intensive care monitoring — arterial line, central venous line, LA line (selected cases)
- Low cardiac output syndrome (LCOS) in first 12–24 hours — milrinone 0.25–0.75 mcg/kg/min is first-line
- Inotropes (adrenaline 0.01–0.1 mcg/kg/min) as needed
- Temporary epicardial pacing wires placed — junctional ectopic tachycardia (JET) is common post-TOF repair
- Maintain sinus rhythm; treat JET with cooling, pacing at faster rate, or amiodarone if haemodynamically significant
- Diuretic therapy (frusemide, spironolactone) for fluid management
- Prophylactic antibiotics — cefazolin for 48 hours post-CPB (eTG Antibiotic)
Long-term Management & Complications
Despite excellent surgical outcomes, the majority of TOF patients develop late sequelae requiring lifelong follow-up in an ACHD centre (e.g., The Prince Charles Hospital Brisbane, Royal Melbourne Hospital, Westmead Hospital Sydney).
| Late Complication | Mechanism | Assessment | Management |
|---|---|---|---|
| Pulmonary regurgitation (PR) | Transannular patch; valvotomy-induced damage | Echo, cardiac MRI (PR fraction >25 % = moderate-severe) | Pulmonary valve replacement (surgical or percutaneous) when indicated |
| RV dilatation & dysfunction | Chronic PR → volume overload → RV remodelling → fibrosis | Cardiac MRI — RVEDVi >150 mL/m² is threshold for PVR consideration | PVR, diuretics, ACE inhibitor if LV dysfunction |
| Ventricular tachycardia (VT) | Re-entrant circuits around VSD patch and RVOT scar | 12-lead ECG, Holter, exercise test, electrophysiology study | ICD implantation if sustained VT or high-risk features; catheter ablation |
| Atrial arrhythmias | RA dilatation, atrial scar | ECG, Holter monitoring | Rate/rhythm control; anticoagulation if AF/Flutter; catheter ablation |
| Sudden cardiac death (SCD) | VT/VF; multifactorial (RV dilatation, QRS duration >180 ms, PR) | Annual ECG (QRS duration), Holter, exercise test | ICD for primary/secondary prevention |
| Residual VSD | Patch leak | Echo | Catheter device closure if haemodynamically significant |
| RVOT aneurysm / obstruction | Patch degeneration; neo-intimal proliferation | Echo, CT, MRI | Re-intervention (surgery or percutaneous valve) |
Pulmonary Valve Replacement (PVR)
PVR is the most common re-intervention after TOF repair. Indications for PVR include:
- Symptomatic moderate-to-severe pulmonary regurgitation (exertional dyspnoea, exercise intolerance)
- Progressive RV dilatation — RVEDVi >150 mL/m² or RVESVi >80 mL/m² on cardiac MRI
- Sustained or symptomatic ventricular arrhythmias associated with RV dilatation
- Declining RV function — RVEF <45 %
Surgical PVR: Bioprosthetic valve (porcine or bovine pericardial) or homograft. Durable but requires future re-replacement.
Percutaneous PVR: Melody® valve (Medtronic) or SAPIEN® valve (Edwards) delivered via catheter. Suitable for patients with conduit or RVOT diameter ≤24 mm. Avoids re-sternotomy. Available at major Australian paediatric and adult congenital centres. PBS: authority required for eligible patients.
Endocarditis Prophylaxis
Per the 2024 Australian guidelines (Heart Foundation / CSANZ consensus):
- Indefinite prophylaxis if residual shunts, prosthetic material, or prior endocarditis
- At least 6 months post-repair (until endothelialisation of patches/valves)
- Amoxicillin 50 mg/kg (max 2 g) PO, 1 hour before procedure — first-line
- Allergy: Clindamycin 20 mg/kg (max 600 mg) PO — penicillin allergy
- Covered procedures: dental procedures involving gingival manipulation, upper respiratory tract procedures, procedures on infected skin/musculoskeletal tissue
- Explain endocarditis prevention — dental hygiene, regular dental reviews
Exercise & Physical Activity
Exercise recommendations are based on residual haemodynamic status, per the 36th Bethesda Conference and updated CSANZ position statements:
| Clinical Status | Exercise Permitted |
|---|---|
| Repaired, no residual lesions, no arrhythmias | All sports encouraged; competitive sport generally permitted |
| Mild PR, normal RV, no arrhythmias | Most sports permitted; annual reassessment |
| Moderate PR, mildly dilated RV | Low-to-moderate competitive sport; avoid high-dynamic sports |
| Severe PR or significant RV dysfunction or arrhythmias | Recreational low-intensity sport only; no competitive sport pending intervention |
Special Populations
Aboriginal and Torres Strait Islander Health Considerations
📚 References
- 1. Apitz C, Webb GD, Redington AN. Tetralogy of Fallot. Lancet. 2009;374(9699):1462–1471.
- 2. Villafañe J, Feinstein JA, Jenkins KJ, et al. Hot topics in tetralogy of Fallot. J Am Coll Cardiol. 2013;62(23):2155–2166.
- 3. Geva T. Indications and timing of pulmonary valve replacement after tetralogy of Fallot repair. Semin Thorac Cardiovasc Surg Pediatr Card Surg Annu. 2006;9(1):11–22.
- 4. Stout KK, Daniels CJ, Aboulhosn JA, et al. 2018 AHA/ACC guideline for the management of adults with congenital heart disease. Circulation. 2019;139(14):e698–e800.
- 5. Baumgartner H, De Backer J, Babu-Narayan SV, et al. 2020 ESC guidelines for the management of adult congenital heart disease. Eur Heart J. 2021;42(6):563–645.
- 6. Australian Institute of Health and Welfare (AIHW). Congenital heart disease in Australia. Cat. no. CDK 4. Canberra: AIHW; 2023.
- 7. d'Udekem Y, Iyengar AJ, Galati JC, et al. Redefining expectations of long-term survival after the Fontan procedure: twenty-five years of follow-up from the entire population of Australia and New Zealand. Circulation. 2014;130(11 Suppl 1):S32–S38.
- 8. Warnes CA, Williams RG, Bashore TM, et al. ACC/AHA 2008 guidelines for the management of adults with congenital heart disease. J Am Coll Cardiol. 2008;52(23):e143–e263.
- 9. Marelli AJ, Ionescu-Ittu R, Mackie AS, Guo L, Dendukuri N, Kaouache M. Lifetime prevalence of congenital heart disease in the general population from 2000 to 2010. Circulation. 2014;130(9):749–756.
- 10. Cheung EWY, Wong WHS, Cheung YF. Meta-analysis of pulmonary valve replacement after operative repair of tetralogy of Fallot. Am J Cardiol. 2010;106(4):552–557.
- 11. Caruana M, Grech JL, Grech V. Review of 22q11.2 deletion and congenital heart disease. Cardiol Young. 2020;30(11):1551–1557.
- 12. Heart Foundation of Australia; Cardiac Society of Australia and New Zealand. Position statement on infective endocarditis prophylaxis. Heart Lung Circ. 2023;32(6):701–710.
- 13. Aboriginal and Torres Strait Islander Health Performance Framework 2020. Australian Institute of Health and Welfare. Canberra: AIHW; 2020.
- 14. RHDAustralia. The 2020 Australian guideline for prevention, diagnosis, and management of acute rheumatic fever and rheumatic heart disease (3rd edition). Darwin: Menzies School of Health Research; 2020.