📋 Key Information Summary
- Atrial flutter is a macro-reentrant atrial tachycardia with organised atrial rates of ~250–350 bpm; typical (CTI-dependent) flutter is the most common form (≈80–90%).
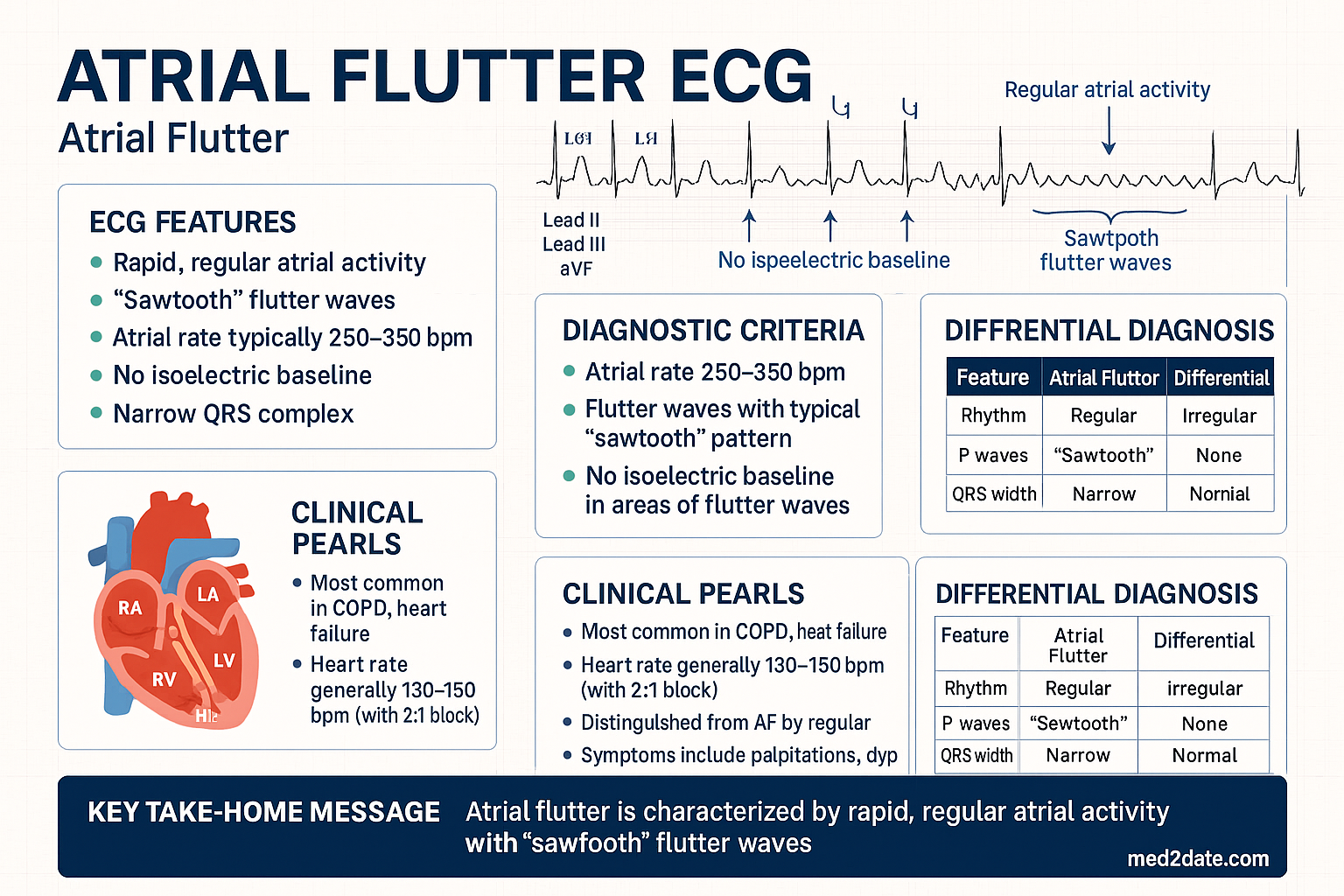
- Typical atrial flutter has a characteristic sawtooth pattern of inverted flutter waves in leads II, III, aVF with positive flutter waves in V1, often with 2:1 AV block yielding a ventricular rate of ~150 bpm.
- Atypical flutters include left atrial flutters, incisional flutters (post-surgical), and CTI-independent right atrial flutters; these are often more difficult to manage medically and ablate.
- Anticoagulation follows the same CHA₂DS₂-VA framework as atrial fibrillation; DOACs are preferred first-line in most patients.
- Rate control targets a resting HR <110 bpm; beta-blockers (metoprolol) or non-dihydropyridine CCBs (diltiazem) are first-line depending on ventricular function.
- Ibutilide IV or atrial overdrive pacing are preferred acute rhythm control methods; direct-current cardioversion (DCCV) at 50–200 J biphasic is highly effective (>95%).
- Catheter ablation of the cavotricuspid isthmus (CTI) for typical flutter has long-term success rates of 90–95% and is recommended for symptomatic or recurrent cases.
- Patients with atrial flutter remain at significant stroke risk equivalent to AF; anticoagulation must not be withheld based on arrhythmia type.
- Flutter with 1:1 conduction is a haemodynamic emergency, often precipitated by class IC antiarrhythmics (flecainide, propafenone) or sympathetic activation.
- Aboriginal and Torres Strait Islander Australians experience higher rates of AF/flutter and cardiovascular morbidity, with barriers to specialist and catheter lab access in remote communities.
- Risk factors include structural heart disease, hypertension, obesity, obstructive sleep apnoea, hyperthyroidism, and chronic lung disease.
- Post-cardiac surgery atrial flutter occurs in 20–30% of patients and may require distinct management strategies including overdrive pacing.
Introduction & Australian Epidemiology
Atrial flutter is a supraventricular arrhythmia characterised by organised macro-reentrant circuits within the atria, producing regular atrial rates typically between 250 and 350 beats per minute. In the most common form — cavotricuspid isthmus (CTI)-dependent typical atrial flutter — the re-entrant circuit revolves around the tricuspid annulus, with the CTI as the critical zone of slow conduction. The AV node usually filters the rapid atrial activity, most commonly producing a 2:1 AV block and a ventricular rate of approximately 150 bpm, though variable block is frequent and 1:1 conduction can be life-threatening.
Atrial flutter shares many risk factors and complications with atrial fibrillation (AF), most notably ischaemic stroke, and carries a similarly elevated thromboembolic risk that warrants anticoagulation in accordance with the CHA₂DS₂-VA scoring system. In clinical practice, atrial flutter frequently coexists with or alternates with AF — termed a "hybrid" or "undifferentiated" atrial tachyarrhythmia — and progression from flutter to AF is common.
Australian Epidemiology
- Atrial flutter accounts for approximately 10–20% of all supraventricular tachycardias presenting to Australian emergency departments.
- The age-standardised incidence increases with advancing age, peaking in the seventh and eighth decades, with a male-to-female ratio of approximately 2:1.
- Hospital admission data from the AIHW show that atrial flutter/AF-related admissions represent one of the most common cardiac diagnoses in Australian hospitals, with over 80,000 separations annually when combined with AF.
- Atrial flutter is a recognised complication following cardiac surgery (CABG, valvular surgery) and catheter-based interventions, with post-operative rates of 20–30%.
- Obstructive sleep apnoea, obesity, and metabolic syndrome — all prevalent in Australia — are increasingly recognised as modifiable risk factors.
- Remote and rural Australians face delayed access to electrophysiology (EP) services, which are predominantly concentrated in tertiary metropolitan centres.
Mechanisms: Typical vs Atypical Flutter
Typical Atrial Flutter (CTI-Dependent)
Typical atrial flutter accounts for 80–90% of all atrial flutter cases. The re-entrant circuit revolves around the tricuspid annulus in the right atrium, using the cavotricuspid isthmus — the anatomical corridor between the inferior vena cava (IVC) and the tricuspid valve annulus — as the critical zone of slow conduction. Two rotation directions exist:
| Feature | Counterclockwise (Common) | Clockwise (Uncommon) |
|---|---|---|
| Frequency | ~90% of typical flutters | ~10% of typical flutters |
| Circuit direction | Counterclockwise around the tricuspid annulus (caudocranial in the septum) | Clockwise around the tricuspid annulus (craniocaudal in the septum) |
| Flutter wave morphology | Negative sawtooth in II, III, aVF; positive in V1 | Positive in II, III, aVF; negative/broad in V1 |
| Ablation target | CTI — same as clockwise | CTI — same as counterclockwise |
| Ablation success | 90–95% | 90–95% |
Atypical Atrial Flutter
Atypical flutter encompasses all macro-reentrant atrial tachycardias that are not dependent on the CTI. These are more heterogeneous and generally more difficult to treat:
- Right atrial atypical flutters: CTI-independent circuits involving the crista terminalis, right atrial free wall, or scar-related re-entry (e.g., post-atrial septal defect repair).
- Left atrial flutters: Often related to prior AF ablation (pulmonary vein isolation), mitral valve surgery, or fibrotic substrate. Circuits may revolve around the mitral annulus, pulmonary veins, or within the left atrial roof.
- Scar-related / incisional flutters: Post-cardiac surgery, particularly after atriotomy for congenital heart disease, septal repairs, or maze procedures. These circuits follow surgical scars and suture lines.
- Focal atrial tachycardias: Strictly speaking not re-entrant, but may mimic flutter on surface ECG; arise from discrete automatic or triggered foci.
Atypical flutters typically require 3D electroanatomical mapping for circuit identification and targeted ablation. Empirical CTI ablation is not effective for atypical flutter and should not be performed without confirming CTI dependence.
ECG Features & Diagnosis
Surface ECG — Typical Atrial Flutter
The surface ECG is the primary diagnostic tool. Key features of typical (counterclockwise) atrial flutter:
- Atrial rate: Regular, 250–350 bpm (classically ~300 bpm).
- Sawtooth flutter waves: Characteristic undulating baseline with negative deflections in leads II, III, and aVF; positive deflection in V1 (due to caudocranial septal activation).
- Ventricular response: Typically 2:1 AV block → ventricular rate ~150 bpm. Variable block (3:1, 4:1) produces slower ventricular rates. 1:1 conduction is an emergency.
- QRS: Usually narrow unless pre-existing bundle branch block, rate-related aberrancy, or ventricular pacing.
Diagnostic Challenges
- Flutter with 2:1 block mimicking sinus tachycardia: A ventricular rate of exactly 150 bpm should always raise suspicion for flutter with 2:1 block. Vagal manoeuvres (carotid sinus massage, Valsalva) or IV adenosine can transiently increase AV block, unmasking flutter waves.
- Flutter vs atrial tachycardia: Atrial rates <240 bpm or isoelectric intervals between P-waves favour atrial tachycardia rather than flutter.
- Flutter vs AF: Fibrillatory baseline with irregular R-R intervals suggests AF, though flutter with variable block can appear irregular.
- Atypical flutter ECG patterns: Variable and less specific; may show atypical P-wave morphology or an indeterminate rhythm — 3D mapping is often required for definitive diagnosis.
Additional Investigations
Rate vs Rhythm Control
Anticoagulation — Foundation of Management
Anticoagulation decisions are guided by the CHA₂DS₂-VA score (Australian adaptation replacing CHA₂DS₂-VASc, removing the sex variable as per NHFA guidelines). The stroke risk in atrial flutter is equivalent to AF; anticoagulation should be offered when the score is ≥2 in men or ≥3 in women, and may be considered at lower scores based on individual risk.
| CHA₂DS₂-VA Risk Factor | Points |
|---|---|
| C — Congestive heart failure | 1 |
| H — Hypertension | 1 |
| A₂ — Age ≥75 years | 2 |
| D — Diabetes mellitus | 1 |
| S₂ — Stroke / TIA / thromboembolism | 2 |
| V — Vascular disease (prior MI, PAD, aortic plaque) | 1 |
| A — Age 65–74 years | 1 |
DOACs — Preferred Anticoagulants
Rate Control
Rate control aims for a resting ventricular rate <110 bpm (lenient strategy) or <80 bpm (strict strategy). The choice of agent depends on left ventricular ejection fraction (LVEF) and comorbidities.
Rhythm Control
Rhythm control is preferred in symptomatic patients, haemodynamic compromise, and where rate control is inadequate. Methods include electrical cardioversion, pharmacological cardioversion, antiarrhythmic maintenance, and catheter ablation.
Acute Rhythm Control
Antiarrhythmic Maintenance Therapy
Catheter Ablation — Cavotricuspid Isthmus
Catheter ablation of typical atrial flutter by creating a bidirectional conduction block across the cavotricuspid isthmus (CTI) is one of the most successful and safe electrophysiology procedures, with long-term success rates of 90–95%. It is recommended for patients with symptomatic typical flutter, recurrent episodes, failed antiarrhythmic therapy, drug intolerance, or patient preference. CTI ablation is classified as a Class I (or strong) recommendation in current Australian and international guidelines.
Procedural Details
Success Rates & Complications
| Outcome | Rate |
|---|---|
| Acute success (bidirectional block achieved) | 95–99% |
| Long-term freedom from recurrence (5 years) | 90–95% |
| Flutter recurrence | 3–8% |
| New-onset AF post-ablation | 20–40% (often pre-existing substrate) |
| Major complications (tamponade, AV block, vascular) | <1% |
Post-Ablation Considerations
- Anticoagulation: Continue for at least 3 months post-ablation; ongoing anticoagulation per CHA₂DS₂-VA score (not based on apparent rhythm success).
- AF monitoring: Up to 40% of patients develop AF post-ablation; consider extended monitoring (loop recorder, 7-day Holter) if symptoms recur.
- Antiarrhythmics: May be weaned 1–3 months post-ablation if no AF is detected, with cardiologist guidance.
- Follow-up: 3-month review with ECG; consider 24-hour Holter or event monitor at 6 and 12 months.
Indications for Referral to Electrophysiology
- Symptomatic typical or atypical atrial flutter not controlled by rate-controlling agents.
- Recurrent atrial flutter despite antiarrhythmic drug therapy.
- Intolerance to antiarrhythmic drugs (side effects, proarrhythmia).
- Atypical flutter or left atrial flutter requiring specialist 3D mapping.
- Young patients or those desiring a drug-free, potentially curative approach.
- Post-surgical flutter refractory to medical therapy.
Special Populations
Aboriginal and Torres Strait Islander Health Considerations
📚 References
- 1. Page RL, Joglar JA, Caldwell MA, et al. 2015 ACC/AHA/HRS Guideline for the Management of Adult Patients with Supraventricular Tachycardia. J Am Coll Cardiol. 2016;67(13):e27–e115.
- 2. Hindricks G, Potpara T, Dagres N, et al. 2020 ESC Guidelines for the diagnosis and management of atrial fibrillation. Eur Heart J. 2021;42(5):373–498.
- 3. Brieger D, Chow C, Nasis A, et al. Management of atrial fibrillation in Australia: an update from the National Heart Foundation of Australia. Med J Aust. 2023;218(1):30–37.
- 4. Saoudi N, Cosío F, Waldo A, et al. A classification of atrial flutter and regular atrial tachycardia according to electrophysiological mechanisms and anatomical bases. Eur Heart J. 2001;22(14):1162–1182.
- 5. Pérez FJ, Schubert CM, Parvez B, et al. Long-term outcomes after catheter ablation of cavo-tricuspid isthmus dependent atrial flutter. Circ Arrhythm Electrophysiol. 2009;2(4):393–401.
- 6. AIHW (Australian Institute of Health and Welfare). Atrial fibrillation in Australia. Cat. no. CVD 90. Canberra: AIHW; 2023.
- 7. RHDAustralia (RHD Australia). The 2020 Australian guideline for prevention, diagnosis and management of acute rheumatic fever and rheumatic heart disease (3rd edn). Menzies School of Health Research; 2020.
- 8. Stiell IG, Macle L. Canadian Cardiovascular Society atrial fibrillation guidelines 2010: management of recent-onset atrial fibrillation and flutter in the emergency department. Can J Cardiol. 2011;27(1):38–46.
- 9. Potpara TS, Lip GYH, Blomström-Lundqvist C, et al. The 2020 European Heart Rhythm Association practical guide on the use of non-vitamin K antagonist oral anticoagulants in patients with atrial fibrillation. Europace. 2021;23(10):1612–1676.
- 10. Medi C, Kalman JM, Freedman SB. Supraventricular tachycardia in adults. Med J Aust. 2019;210(5):222–228.
- 11. NHS (National Health Service) RightCare. Atrial fibrillation and atrial flutter: optimising diagnosis and management. Br J Gen Pract. 2020;70(693):178–179.
- 12. Wijesurendra RS, Casadei B. Mechanisms of atrial fibrillation. Heart. 2019;105(24):1860–1867.