📋 Key Information Summary
- Supraventricular tachycardia (SVT) encompasses AVNRT, AVRT (including Wolff-Parkinson-White syndrome), and focal atrial tachycardia — all arising above the His bundle.
- AVNRT accounts for approximately 60% of all paroxysmal SVT and is twice as common in women as men.
- A 12-lead ECG during tachycardia is the cornerstone of diagnosis — assess QRS width, P-wave morphology, RP interval, and the presence or absence of delta waves.
- The modified Valsalva manoeuvre (performed supine with leg elevation and abdominal strain) is first-line acute management with conversion rates of 40–50%.
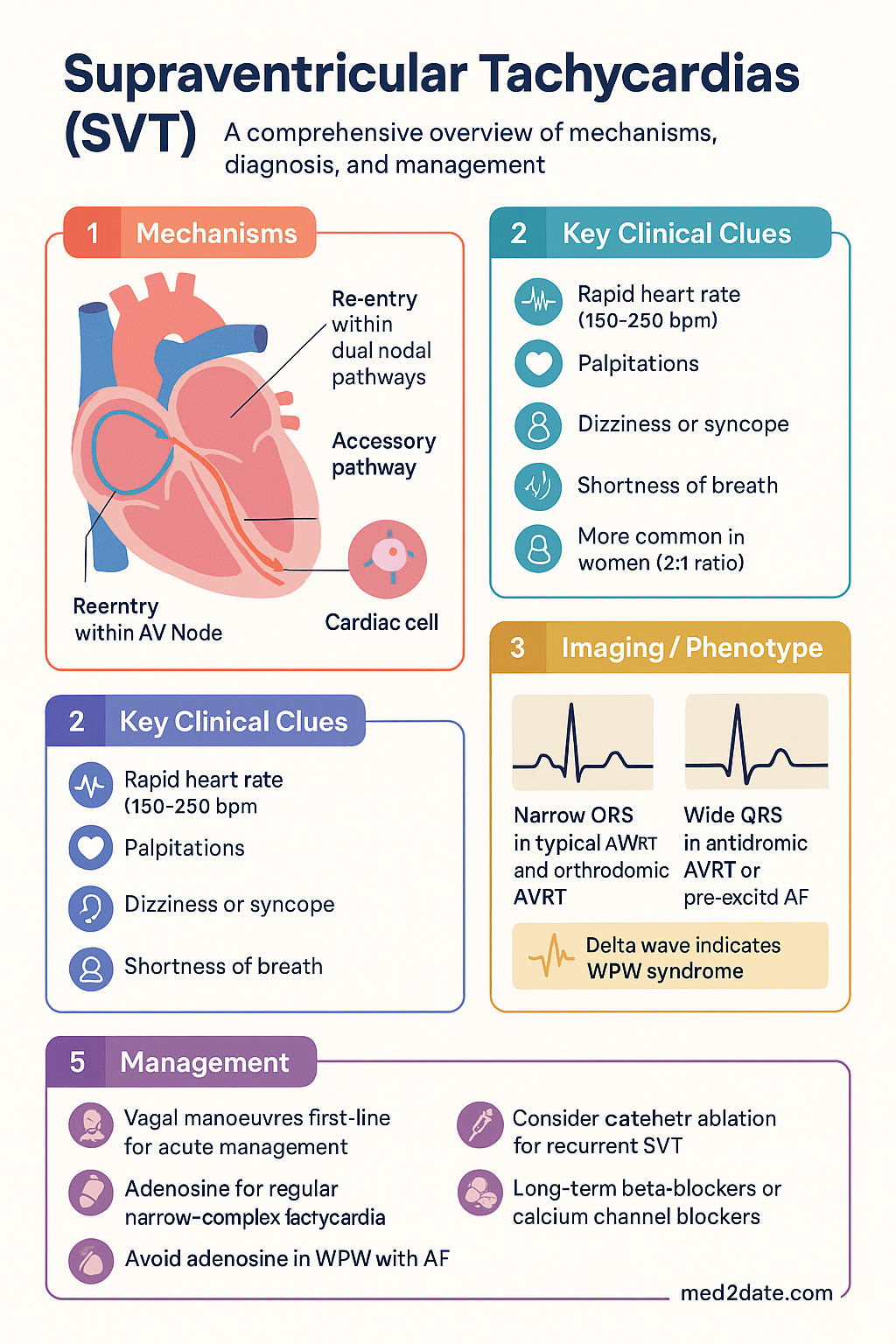
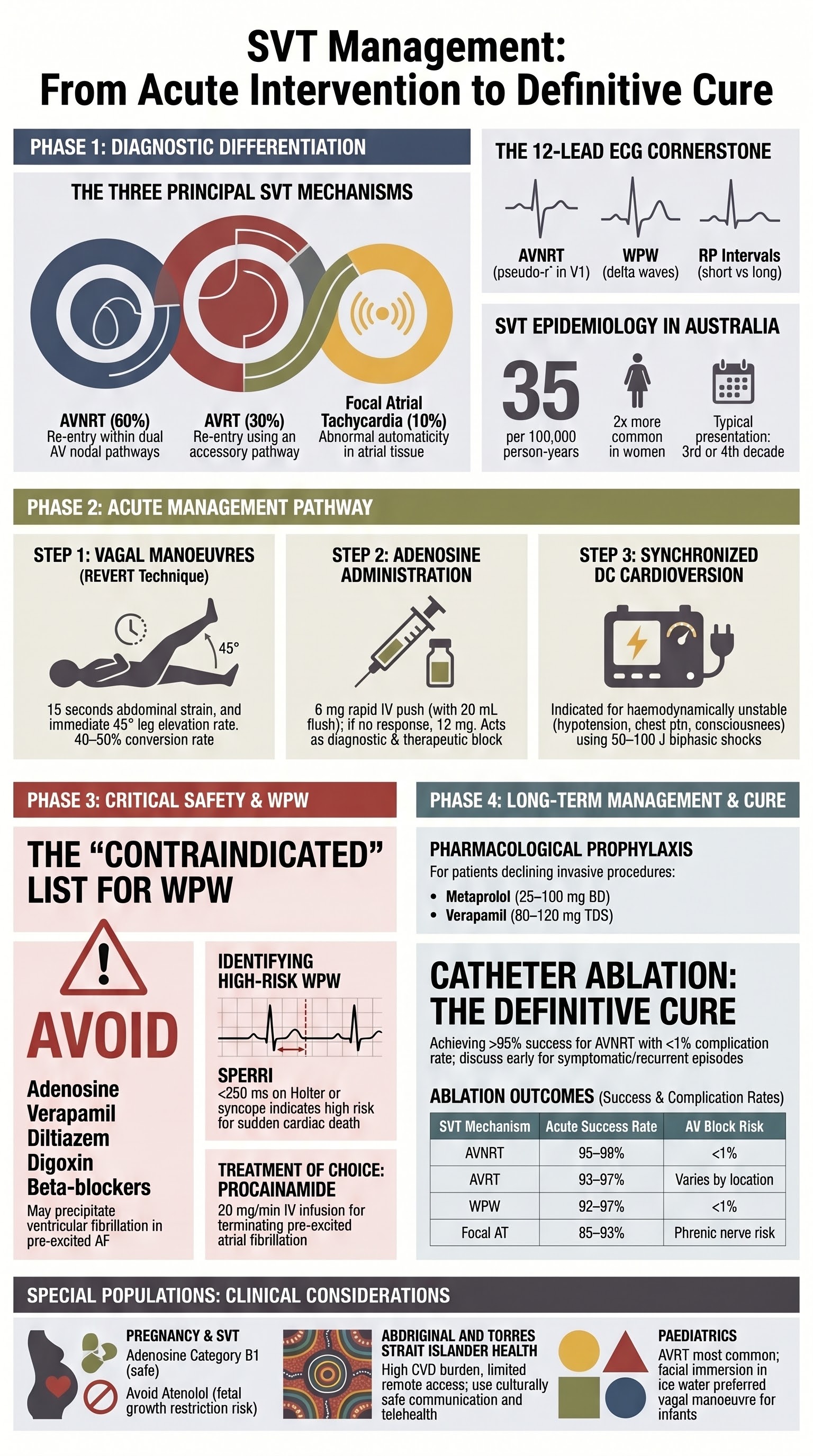
- Adenosine (6 mg rapid IV push → 12 mg if needed) is the pharmacological agent of choice for regular narrow-complex tachycardia; it is both diagnostic and therapeutic.
- In pre-excited atrial fibrillation (WPW), adenosine, verapamil, diltiazem, and digoxin are CONTRAINDICATED — they may precipitate ventricular fibrillation.
- Synchronised DC cardioversion (50–100 J biphasic) is indicated for haemodynamically unstable SVT unresponsive to vagal manoeuvres and adenosine.
- Long-term pharmacotherapy with beta-blockers (metoprolol, atenolol) or non-dihydropyridine calcium channel blockers (verapamil) is first-line for recurrent SVT.
- Catheter ablation for AVNRT achieves >95% acute success with <1% complication rate and is curative — it should be discussed early for recurrent or symptomatic episodes.
- WPW with a shortest pre-excited R-R interval <250 ms on Holter or inducible AVRT/AF at electrophysiology study indicates high risk and warrants ablation.
- Aboriginal and Torres Strait Islander Australians experience higher cardiovascular disease burden; access to electrophysiology services and specialist follow-up may be limited in remote communities.
Introduction & Australian Epidemiology
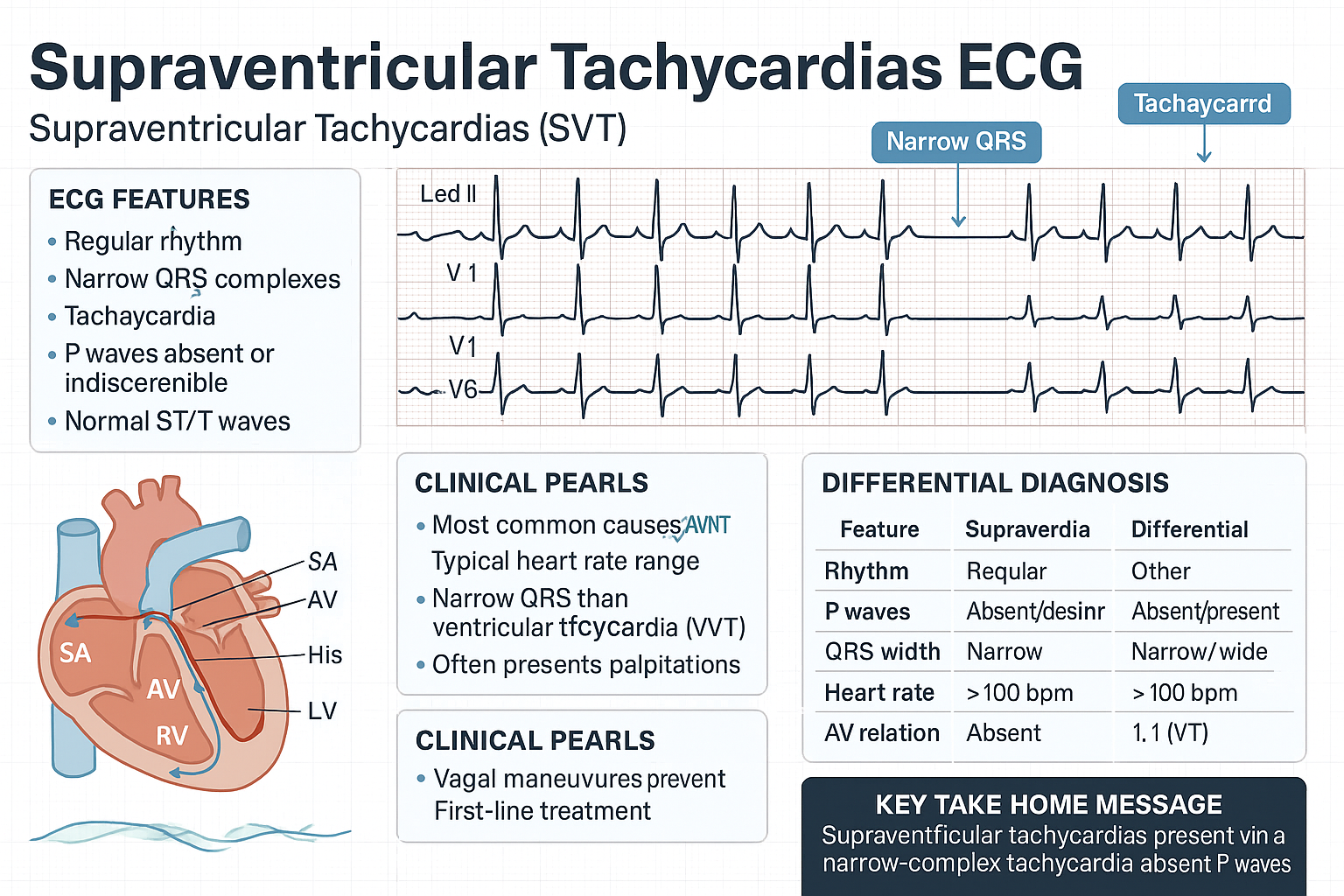
Supraventricular tachycardia (SVT) is a collective term for tachyarrhythmias that originate at or above the atrioventricular (AV) node, producing a heart rate typically between 150 and 250 beats per minute. SVT excludes sinus tachycardia, atrial fibrillation (AF), and atrial flutter, which are classified separately despite sharing a supraventricular origin. The three principal mechanisms are AV nodal re-entrant tachycardia (AVNRT), AV re-entrant tachycardia (AVRT, including Wolff-Parkinson-White syndrome), and focal atrial tachycardia (AT).
In Australia, the incidence of paroxysmal SVT is estimated at 35 per 100,000 person-years, with a point prevalence of approximately 2.25 per 1,000. AVNRT is the most common mechanism (≈60%), followed by AVRT (≈30%), and atrial tachycardia (≈10%). SVT is roughly twice as prevalent in women and tends to present in the third to fourth decade of life, although it may occur at any age. Paediatric SVT accounts for a significant proportion of emergency department presentations in children, with AVRT predominating in this age group.
The Australian Institute of Health and Welfare (AIHW) reports that cardiac arrhythmias contribute substantially to emergency department burden nationally, with SVT being among the most common paroxysmal arrhythmias seen. In the 2022–23 financial year, cardiac arrhythmia presentations exceeded 140,000 emergency encounters Australia-wide. Access to electrophysiology services is concentrated in major metropolitan centres, creating disparities for rural and remote populations, particularly Aboriginal and Torres Strait Islander communities.
Most SVT is not life-threatening; however, recurrent episodes impair quality of life, cause anxiety, and may lead to tachycardia-mediated cardiomyopathy if sustained and untreated. Catheter ablation has transformed the management of SVT, offering a definitive cure with high success rates and minimal morbidity.
Diagnosis & Mechanisms
Pathophysiology of SVT Mechanisms
Understanding the electrophysiological mechanism is essential for selecting appropriate acute and long-term therapy. The three principal SVT mechanisms are distinguished by their circuit or focus of origin:
| Feature | AVNRT | AVRT (Orthodromic) | Focal Atrial Tachycardia |
|---|---|---|---|
| Mechanism | Re-entry within dual AV nodal pathways (slow + fast) | Re-entry using accessory pathway (concealed or manifest) + AV node | Abnormal automaticity, triggered activity, or micro-re-entry in atrial tissue |
| Proportion of SVT | ≈60% | ≈30% | ≈10% |
| Typical age of onset | 30–50 years, F > M (2:1) | Children and young adults | Any age; peaks in 40s–60s |
| P wave during tachycardia | Often hidden in QRS (pseudo-r′ in V1, pseudo-S in II/III/aVF) or short RP | Visible after QRS, short RP (RP < PR) | Visible before QRS; morphology differs from sinus P wave; long or short RP |
| ECG between episodes | Normal (no delta wave) | Delta wave if manifest accessory pathway (WPW); normal if concealed | Normal |
| Response to adenosine | Terminates (breaks re-entry at slow pathway) | Terminates (blocks AV node) | May terminate or reveal underlying P waves (diagnostic) |
AV Nodal Re-entrant Tachycardia (AVNRT)
AVNRT is the most common paroxysmal SVT. It occurs when two functionally distinct pathways exist within or near the AV node — a slowly conducting pathway (typical antegrade limb) and a rapidly conducting pathway (typical retrograde limb). The re-entrant circuit is confined to the AV node and its perinodal atrial tissue. In typical (slow–fast) AVNRT, the impulse travels antegradely via the slow pathway and retrogradely via the fast pathway, producing a short RP tachycardia with retrograde P waves often buried within or just after the QRS complex.
Atypical (fast–slow or slow–slow) AVNRT accounts for approximately 5–10% of AVNRT and presents with a long RP tachycardia that can mimic atrial tachycardia or atypical AVRT.
AV Re-entrant Tachycardia (AVRT)
AVRT requires an accessory pathway connecting the atrium and ventricle outside the normal AV conduction system. In orthodromic AVRT (the most common form, >90%), conduction proceeds antegradely through the AV node and retrogradely through the accessory pathway, producing a narrow QRS complex with visible retrograde P waves. In antidromic AVRT (<10%), conduction is antegradely through the accessory pathway, resulting in a wide QRS tachycardia that may be confused with ventricular tachycardia.
Accessory pathways may be manifest (capable of antegrade conduction, producing a delta wave on resting ECG — Wolff-Parkinson-White pattern) or concealed (only capable of retrograde conduction, with a normal resting ECG). The distinction is clinically critical because manifest pathways carry the risk of pre-excited atrial fibrillation and sudden cardiac death.
Focal Atrial Tachycardia
Focal atrial tachycardia arises from a discrete focus within the atrial myocardium, commonly near the crista terminalis, pulmonary vein ostia, or around the coronary sinus. The P-wave morphology is determined by the site of origin. Multifocal atrial tachycardia (MAT), characterised by ≥3 distinct P-wave morphologies at varying rates, is typically associated with underlying pulmonary disease, theophylline use, or electrolyte disturbance rather than a single ablatable focus.
ECG Differentiation
A 12-lead ECG obtained during tachycardia is the single most valuable diagnostic tool. Key features to assess include:
- QRS duration: Narrow (<120 ms) in typical AVNRT and orthodromic AVRT; wide (≥120 ms) in antidromic AVRT, AVNRT with aberrancy, or pre-excited AF.
- RP interval: Short RP (RP < PR) in typical AVNRT and orthodromic AVRT; long RP (RP > PR) in atypical AVNRT, PJRT, and some atrial tachycardias.
- Pseudo-r′ in V1 and pseudo-S in leads II/III/aVF: Highly specific for typical (slow–fast) AVNRT — represents simultaneous atrial and ventricular depolarisation.
- Delta wave in sinus rhythm: Indicates a manifest accessory pathway (WPW pattern).
- Alternating QRS amplitude (electrical alternates): Can occur in any rapid SVT; more commonly associated with AVRT but not pathognomonic.
- AV dissociation: FAVOURS ventricular tachycardia rather than SVT; its absence does not confirm SVT.
Electrophysiology Study (EPS)
An invasive electrophysiology study is indicated when:
- The mechanism of SVT is uncertain after non-invasive evaluation.
- Catheter ablation is planned (EPS and ablation are typically performed as a single procedure).
- Risk stratification of accessory pathways is required (WPW with syncope, aborted cardiac arrest, or high-risk occupations — see WPW section).
- Recurrent SVT despite pharmacotherapy.
EPS involves placing multipolar catheters in the right atrium, His bundle position, coronary sinus, and right ventricle. Programmed electrical stimulation is used to induce tachycardia and map the circuit. In Australia, EPS is available at all major tertiary centres and an increasing number of private electrophysiology labs. A referral to a cardiac electrophysiologist is required.
Acute Management
The acute management of SVT follows a stepwise approach: initial assessment and monitoring, vagal manoeuvres, pharmacotherapy (principally adenosine), and synchronised cardioversion for haemodynamically unstable patients.
Step 1 — Initial Assessment
- Confirm haemodynamic stability — assess blood pressure, level of consciousness, chest pain, and signs of end-organ hypoperfusion.
- Obtain a 12-lead ECG during tachycardia (before treatment if the patient is stable).
- Establish IV access and continuous cardiac monitoring.
- Identify and treat reversible precipitants: caffeine, alcohol, sympathomimetics, thyrotoxicosis, electrolyte abnormalities (hypokalaemia, hypomagnesaemia).
Step 2 — Vagal Manoeuvres
Vagal manoeuvres increase vagal tone, transiently slowing AV nodal conduction and potentially terminating re-entrant tachycardias that incorporate the AV node as part of the circuit.
- Modified Valsalva manoeuvre (REVERT technique): The patient performs a forced expiratory effort against a closed glottis (40 mmHg for 15 seconds using a syringe or manometer) while supine, followed immediately by passive leg elevation at 45° for 15 seconds. This technique increases intrathoracic pressure, reduces venous return, and then augments vagal reflex on release. Conversion rate: 40–50% (superior to standard Valsalva at ≈17%).
- Carotid sinus massage: Firm pressure applied unilaterally for 5–10 seconds over the carotid bifurcation (at the level of the thyroid cartilage). CONTRAINDICATED in patients with carotid bruits, recent stroke/TIA, or known carotid stenosis. Auscultate for bruits before performing.
- Facial immersion in cold water (diving reflex): Particularly effective in infants and children. Apply ice-cold water–soaked towels to the face or immerse the face in cold water for 15–30 seconds.
- Phenylephrine (IV): 100–500 mcg IV bolus titrated to raise systolic BP by 50% or to 160 mmHg. Baroreceptor-mediated vagal activation. Use with caution; contraindicated in severe hypertension or coronary artery disease. Rarely used in modern practice.
Step 3 — Adenosine
Step 4 — Second-Line Pharmacotherapy (if adenosine fails)
Step 5 — Synchronised DC Cardioversion
Synchronised cardioversion is indicated for:
- Haemodynamically unstable SVT (hypotension, altered consciousness, acute pulmonary oedema, chest pain with ischaemic ECG changes) unresponsive to vagal manoeuvres and adenosine.
- Pre-excited atrial fibrillation where pharmacological options are limited or contraindicated.
- Refractory SVT unresponsive to all pharmacological interventions.
Technique: Biphasic synchronised shock at 50 J, escalating to 100 J, then 200 J if needed. Ensure synchronisation mode to avoid R-on-T phenomenon. Procedural sedation with propofol or midazolam/fentanyl should be administered where time and resources allow.
Long-term Management
Long-term management of SVT depends on the frequency and severity of episodes, patient preference, the SVT mechanism, and the presence of structural heart disease. Options include a pill-in-the-pocket approach, daily prophylactic pharmacotherapy, and catheter ablation.
Pharmacological Prophylaxis
Daily pharmacotherapy is appropriate for patients with frequent SVT episodes who decline or are not yet ready for catheter ablation. The choice of agent depends on the SVT mechanism, comorbidities, and the presence of structural heart disease.
Pill-in-the-Pocket Approach
For patients with infrequent but well-tolerated SVT episodes, a self-administered single oral dose of flecainide (2–3 mg/kg, typically 150–200 mg) or diltiazem (120 mg) plus metoprolol (50 mg) at the onset of tachycardia can terminate the episode without emergency department attendance. This strategy requires prior in-hospital observation to confirm efficacy and safety. It is appropriate for AVNRT and AVRT but NOT for WPW with pre-excitation unless directed by an electrophysiologist.
Catheter Ablation
Catheter ablation is the definitive treatment for SVT and should be discussed with all patients at an early stage. It is particularly recommended for:
- Recurrent or poorly tolerated SVT episodes.
- Patient preference for a curative procedure over lifelong pharmacotherapy.
- Drug intolerance, contraindications, or failure of pharmacotherapy.
- Manifest accessory pathways (WPW) with high-risk features.
| SVT Mechanism | Ablation Target | Acute Success Rate | Recurrence Rate | Key Complications |
|---|---|---|---|---|
| AVNRT | Slow pathway ablation (inferior to AV node) | 95–98% | 2–5% | AV block requiring pacemaker <1% |
| AVRT (concealed pathway) | Accessory pathway (atrial or ventricular insertion) | 93–97% | 3–7% | Varies by location — septal pathways carry higher AV block risk |
| WPW (manifest pathway) | Accessory pathway ablation | 92–97% | 3–8% | AV block <1% (higher for anteroseptal/mid-septal pathways) |
| Focal AT | Focal origin (mapped during EPS) | 85–93% | 7–15% | Phrenic nerve injury (lateral right atrial foci) |
In Australia, catheter ablation for SVT is performed at major public and private electrophysiology centres in all capital cities and several regional centres. Public hospital waiting times vary by state (typically 3–12 months). Private health insurance or self-funding may allow earlier access. MBS item numbers for electrophysiology study and ablation apply (consult current MBS schedule). The procedure is typically performed as a day-case or overnight stay under local anaesthesia with conscious sedation.
Wolff-Parkinson-White (WPW) Syndrome
Wolff-Parkinson-White syndrome is defined as the combination of a manifest accessory pathway (pre-excitation on resting 12-lead ECG) and documented tachyarrhythmia. The WPW pattern (asymptomatic delta wave on ECG without arrhythmia) occurs in approximately 1–3 per 1,000 of the general population. The lifetime risk of sudden cardiac death in WPW is estimated at 0.1–0.6%, predominantly from pre-excited atrial fibrillation degenerating to ventricular fibrillation.
ECG Features of Pre-excitation
- Delta wave: Slurred upstroke of the QRS complex arising from early ventricular activation via the accessory pathway.
- Short PR interval: <120 ms due to rapid AV conduction bypassing the normal AV nodal delay.
- Wide QRS: ≥120 ms (fusion of pre-excited and normal ventricular activation).
- Secondary ST-T wave changes: Discordant to the direction of the delta wave (may mimic ischaemia or LVH).
Risk Stratification
Risk stratification aims to identify patients with manifest accessory pathways at risk of sudden cardiac death from rapid ventricular conduction during atrial fibrillation. This is essential for guiding management decisions regarding ablation versus observation.
Avoiding AV Nodal Blockers in Pre-excited Atrial Fibrillation
Ablation Indications in WPW
Catheter ablation of the accessory pathway is the definitive treatment for WPW syndrome and is indicated for:
- Symptomatic patients with documented AVRT or pre-excited AF (class I indication).
- Asymptomatic patients with SPERRI <250 ms or inducible arrhythmia at EPS (class I).
- High-risk occupations — commercial pilots (CASA requirement: no WPW without successful ablation), train drivers, divers, emergency services personnel.
- Patients who prefer definitive treatment over pharmacotherapy or observation.
- Resuscitated sudden cardiac arrest in WPW (class I — ablation mandatory).
Pharmacological Management of WPW (when ablation deferred or declined)
If ablation is not immediately available or the patient declines, antiarrhythmic agents that slow accessory pathway conduction are preferred:
- Flecainide (50–150 mg PO BD): Effective for AVRT; slows accessory pathway conduction. Avoid in structural heart disease.
- Propafenone (150–300 mg PO TDS): Similar mechanism and precautions to flecainide.
- Sotalol (80–160 mg PO BD): Class III antiarrhythmic with beta-blocking properties. Effective for both AVRT and pre-excited AF. Risk of QT prolongation and torsades de pointes.
Avoid all of the following in manifest WPW: adenosine, verapamil, diltiazem, digoxin, and standalone beta-blockers — these may enhance accessory pathway conduction during AF.
Monitoring
Post-Ablation Monitoring
- ECG at 1 day, 1 month, 3 months, and 12 months post-ablation to confirm absence of delta wave and monitor for recurrence.
- 24-hour Holter monitor at 3–6 months if palpitations recur.
- Exercise stress test at 3–6 months post-ablation for WPW patients to confirm absence of pre-excitation under physiological stress.
- Repeat EPS is indicated if symptoms recur or pre-excitation returns.
Pharmacotherapy Monitoring
- Beta-blockers: Monitor heart rate, blood pressure, symptoms of fatigue, bronchospasm. ECG at baseline and 1–2 weeks after initiation or dose change.
- Verapamil: Monitor heart rate, blood pressure, symptoms of constipation, peripheral oedema. ECG at baseline and after initiation.
- Flecainide: ECG at baseline and after initiation (assess QRS duration — increase >25% warrants dose reduction). Serum levels if renal impairment. Echocardiogram to exclude structural heart disease BEFORE commencing.
- Sotalol: ECG at baseline and after initiation (QTc — stop if QTc >500 ms). Serum potassium and magnesium. Renal function for dosing.
Long-term Follow-up
Patients with SVT should have regular follow-up with their general practitioner or cardiologist. Those on pharmacotherapy should be reviewed at least every 6–12 months to assess efficacy, side effects, and the need for continued treatment. Patients managed with a pill-in-the-pocket strategy should maintain a symptom diary and have access to emergency care.
Special Populations
Pregnancy
- SVT is the most common symptomatic arrhythmia in pregnancy, with increased frequency due to increased blood volume, hormonal changes, and heightened sympathetic tone.
- Vagal manoeuvres are first-line and safe in pregnancy.
- Adenosine is considered safe (Category B1 — ultra-short half-life, no fetal accumulation) and is the preferred pharmacological agent.
- Metoprolol (Category C) and verapamil (Category C) can be used when adenosine fails or for prophylaxis. Metoprolol is generally preferred for long-term use.
- Flecainide (Category C) may be used in refractory cases, particularly for accessory pathway–mediated tachycardia.
- Avoid atenolol in pregnancy — associated with fetal growth restriction (use metoprolol instead).
- Synchronised cardioversion is safe at all stages of pregnancy and should not be delayed for haemodynamically unstable SVT.
- Catheter ablation is generally deferred until after delivery unless SVT is refractory and causing significant haemodynamic compromise. If required, zero-fluoroscopy or low-fluoroscopy ablation techniques minimise fetal radiation exposure.
Paediatrics
- SVT is the most common arrhythmia in children, with AVRT (via accessory pathways) predominating over AVNRT, especially in infancy.
- Infants may present with nonspecific features: poor feeding, irritability, pallor, tachypnoea, and signs of heart failure if SVT is sustained.
- Acute management: Facial immersion in ice water (diving reflex) is the preferred vagal manoeuvre in infants. Adenosine 0.1 mg/kg rapid IV push (max 6 mg first dose), escalate to 0.2 mg/kg (max 12 mg).
- Synchronised cardioversion at 0.5–1 J/kg (biphasic), escalating to 2 J/kg if needed, for haemodynamically unstable SVT.
- Long-term prophylaxis: Propranolol (1–2 mg/kg/day divided TDS) or atenolol (1–2 mg/kg/day) are first-line. Flecainide (3–6 mg/kg/day divided BD) for refractory cases or accessory pathway–mediated tachycardia.
- Catheter ablation in children is typically deferred until age 4–5 years unless SVT is refractory or causing ventricular dysfunction. The procedure is performed under general anaesthesia with a success rate of 90–95% in experienced paediatric centres.
- Infantile SVT (onset <1 year) may spontaneously resolve by age 1 — some centres use a period of observation with prophylaxis rather than early ablation.
Elderly
- SVT in elderly patients is more commonly atrial tachycardia rather than AVNRT/AVRT. Diagnostic overlap with atrial fibrillation and flutter is common.
- Elderly patients are more susceptible to haemodynamic compromise during SVT due to reduced cardiac reserve and diastolic dysfunction.
- Adenosine is safe but side effects (chest tightness, dyspnoea) may be more distressing. Use standard dosing — no adjustment for age.
- Beta-blockers and verapamil require careful titration due to increased sensitivity to negative chronotropy and inotropy. Start at lower doses.
- Assess for concurrent medications (rate-controlling agents for AF, antihypertensives) that may interact or compound bradycardia risk.
- Catheter ablation remains effective and safe in the elderly; however, procedural risk is modestly increased and patient frailty should be considered in decision-making.
Renal Impairment
- Adenosine requires no renal dose adjustment — it is metabolised intracellularly by adenosine deaminase within seconds.
- Atenolol is predominantly renally excreted — dose reduction required (see drug card above). Metoprolol is preferred as it is hepatically metabolised.
- Flecainide: reduce dose and monitor serum levels in eGFR <35 mL/min (30–40% renal excretion).
- Sotalol: significant renal excretion — dose reduction mandatory based on eGFR. CrCl 30–60 mL/min: 80 mg daily. CrCl 10–30 mL/min: 80 mg every 48 hours. CrCl <10 mL/min: avoid.
- Procainamide: active metabolite (NAPA) is renally cleared — reduce infusion rate and monitor levels in renal impairment.
Hepatic Impairment
- Metoprolol: significant first-pass metabolism — use cautiously in severe hepatic impairment (Child-Pugh C); consider dose reduction.
- Verapamil: extensive hepatic metabolism — reduce dose by 50% in hepatic impairment; monitor for excessive bradycardia and hypotension.
- Flecainide: hepatic metabolism to a limited extent — generally safe in mild–modate impairment; caution in severe liver disease.
- Adenosine: no hepatic adjustment required.
Immunocompromised
- SVT management does not fundamentally change in immunocompromised patients. However, consider that drug interactions with immunosuppressants may affect antiarrhythmic metabolism (e.g., tacrolimus and cyclosporine with verapamil via CYP3A4 inhibition).
- HIV patients on protease inhibitors may have impaired verapamil metabolism — consider metoprolol instead.
- Transplant recipients may have denervated hearts that do not respond to vagal manoeuvres — proceed directly to adenosine.
Aboriginal and Torres Strait Islander Australians experience a disproportionately higher burden of cardiovascular disease compared to non-Indigenous Australians. While specific data on SVT prevalence in Indigenous populations are limited, the overall burden of cardiac arrhythmias is elevated due to higher rates of rheumatic heart disease, cardiomyopathy, ischaemic heart disease, and congenital heart disease — all of which may predispose to or complicate SVT.
📚 References
- 1. Page RL, Joglar JA, Caldwell MA, et al. 2015 ACC/AHA/HRS Guideline for the Management of Adult Patients With Supraventricular Tachycardia. J Am Coll Cardiol. 2016;67(13):e27–e115.
- 2. Brugada J, Katritsis DG, Arbelo E, et al. 2019 ESC Guidelines for the Management of Patients With Supraventricular Tachycardia. Eur Heart J. 2020;41(5):655–720.
- 3. Appelboam A, Reuben A, Mann C, et al. Postural modification to the standard Valsalva manoeuvre for emergency treatment of supraventricular tachycardias (REVERT): a randomised controlled trial. Lancet. 2015;386(10005):1747–1753.
- 4. Al-Khatib SM, Arshad A, Balk EM, et al. Risk Stratification for Arrhythmic Events in Patients With Asymptomatic Pre-Excitation: A Systematic Review for the 2015 ACC/AHA/HRS Guideline. Circulation. 2016;133(14):e575–e586.
- 5. Obeyesekere MN, Leong-Sit P, Massel D, et al. Risk of arrhythmia and sudden death in patients with asymptomatic pre-excitation: a meta-analysis. Circulation. 2012;125(19):2308–2315.
- 6. Brembilla-Perrot B. Pre-excited atrial fibrillation: what is the risk of sudden death and how to manage it? Arch Cardiovasc Dis. 2013;106(12):641–644.
- 7. Australian Institute of Health and Welfare (AIHW). Heart, stroke and vascular disease — Australian facts. AIHW, Canberra; 2024.
- 8. Katritsis DG, Boriani G, Cosio FG, et al. European Heart Rhythm Association (EHRA) position paper on arrhythmia management in cardiac patients during the COVID-19 pandemic. Europace. 2020;22(8):1197–1202.
- 9. National Heart Foundation of Australia and Cardiac Society of Australia and New Zealand. Guidelines for the prevention, detection, and management of heart failure in Australia. 2018 (updated 2024).
- 10. RHDAustralia (Rheumatic Heart Disease Australia). Acute Rheumatic Fever and Rheumatic Heart Disease Australian Guideline. 3rd edition. Darwin: Menzies School of Health Research; 2020.
- 11. Civil Aviation Safety Authority (CASA). Designated Aviation Medical Examiner's Handbook. Canberra: CASA; 2023. [Cardiovascular section — WPW and arrhythmia certification requirements].
- 12. January CT, Wann LS, Calkins H, et al. 2019 AHA/ACC/HRS Focused Update of the 2014 Guideline for the Management of Patients With Atrial Fibrillation. J Am Coll Cardiol. 2019;74(1):104–132.
- 13. Saul JP, Kanter RJ, Abrams D, et al. PACES/HRS Expert Consensus Statement on the Use of Catheter Ablation in Children and Patients With Congenital Heart Disease. Heart Rhythm. 2016;13(6):e251–e289.
- 14. National Aboriginal Community Controlled Health Organisation (NACCHO). National Aboriginal and Torres Strait Islander Health Plan 2021–2031. Canberra: Commonwealth of Australia; 2021.