📋 Key Information Summary
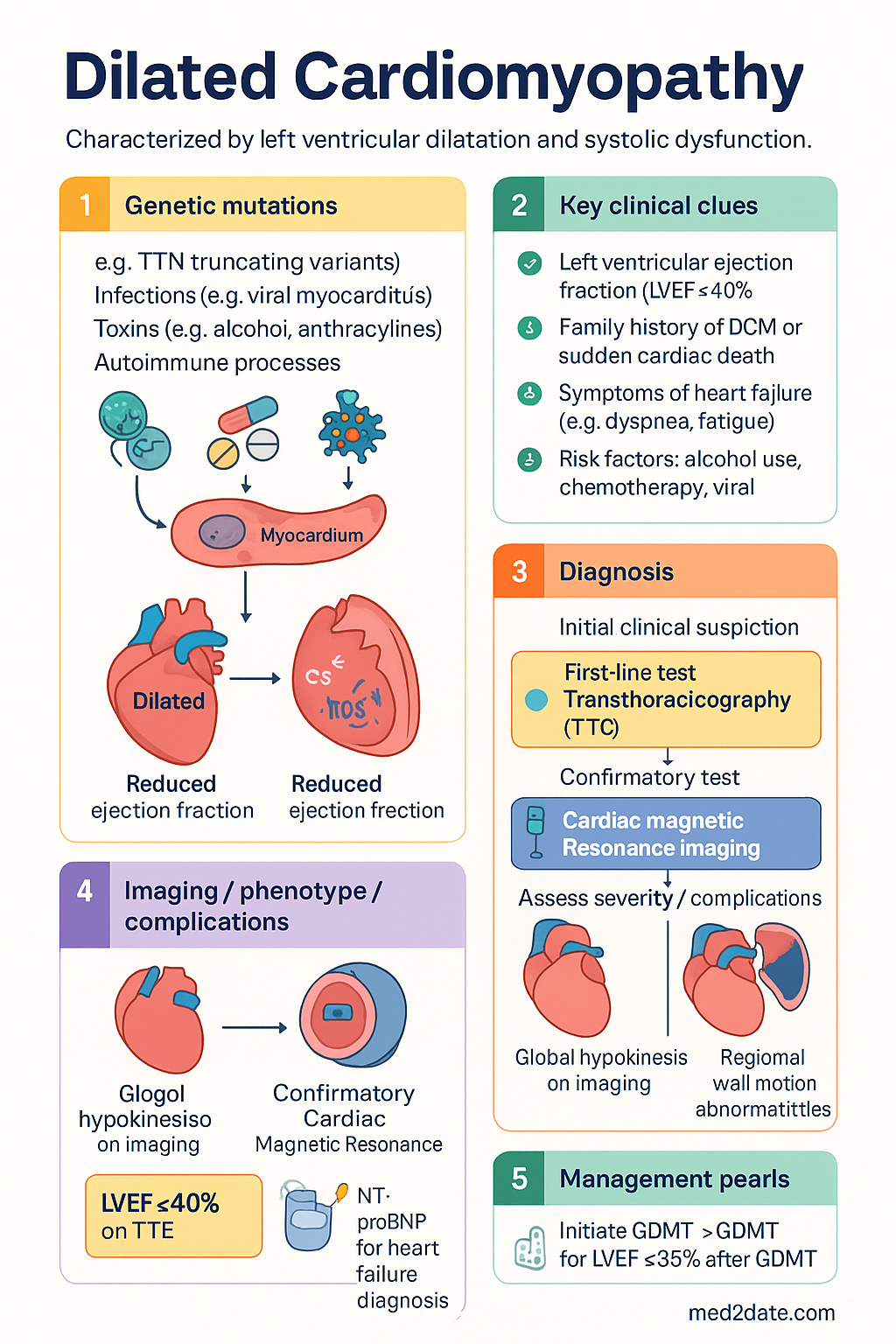
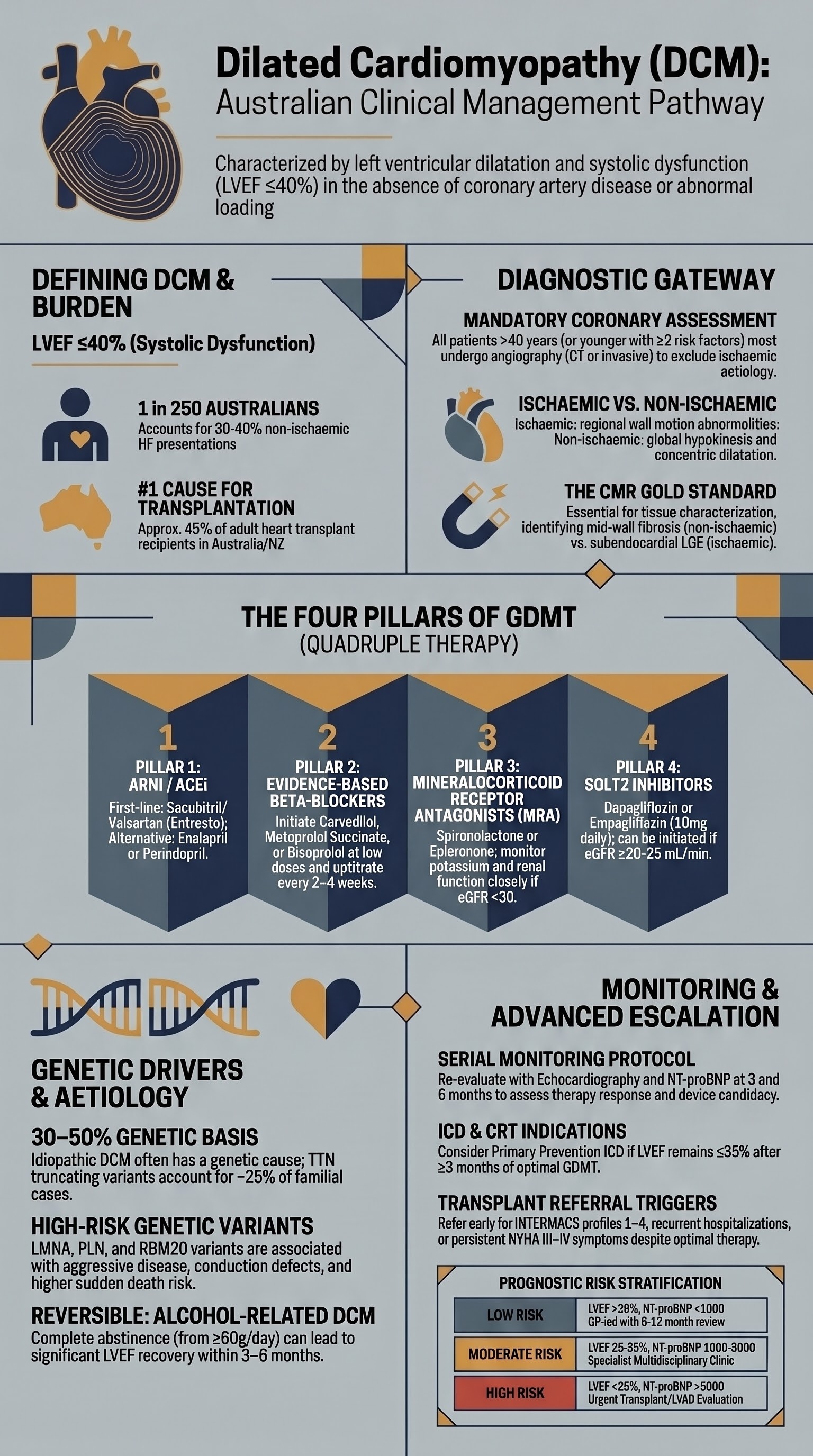
- Definition: Dilated cardiomyopathy (DCM) is characterised by left ventricular dilatation and systolic dysfunction (LVEF ≤40%) in the absence of abnormal loading conditions or coronary artery disease sufficient to explain the degree of impairment.
- Prevalence: Estimated prevalence of 1:250–1:500 in Australia; DCM accounts for approximately 30–40% of all non-ischaemic heart failure presentations and is the leading indication for cardiac transplantation.
- Ischaemic vs non-ischaemic: Coronary angiography (CT or invasive) is mandatory in all newly diagnosed DCM patients aged >40 years or with cardiovascular risk factors to exclude ischaemic aetiology — this distinction drives both prognosis and management.
- Genetic aetiology: Up to 30–50% of idiopathic DCM is genetic; TTN (titin) truncating variants account for ~25% of familial cases. Genetic testing should be offered to all patients with a family history of DCM, sudden cardiac death, or early-onset heart failure.
- Myocardial biopsy: Endomyocardial biopsy (EMB) is indicated when acute myocarditis is suspected (acute heart failure with recent viral illness, new LVEF <45%, elevated troponin), giant cell myocarditis, eosinophilic myocarditis, or cardiac sarcoidosis is on the differential.
- GDMT pillars: Guideline-directed medical therapy comprises ACEi/ARB/ARNI, beta-blocker (carvedilol, metoprolol succinate, or bisoprolol), mineralocorticoid receptor antagonist (MRA), and SGLT2 inhibitor (dapagliflozin or empagliflozin) — all four should be initiated and uptitrated to maximum tolerated doses.
- ICD candidacy: Primary prevention ICD (implantable cardioverter-defibrillator) should be considered after ≥3 months of optimal GDMT if LVEF remains ≤35% (NYHA II–III); secondary prevention ICD for survivors of cardiac arrest or sustained VT.
- Inflammatory DCM: Immunosuppression (prednisolone ± azathioprine) may be considered in biopsy-proven inflammatory DCM; empiric immunosuppression without biopsy confirmation is NOT recommended.
- Alcohol and toxic DCM: Complete alcohol abstinence is essential in alcohol-related DCM — partial recovery of LVEF is common with sustained abstinence. Anthracycline-induced DCM requires cardiotoxicity surveillance during and after chemotherapy.
- Family screening: First-degree relatives of all DCM patients should undergo clinical screening with ECG and transthoracic echocardiography, ideally with genetic counselling if a pathogenic variant is identified.
- Advanced therapies: Referral for heart transplant assessment and/or LVAD evaluation should be considered early when patients demonstrate persistent NYHA III–IV symptoms, declining LVEF despite optimal GDMT, recurrent hospitalisations, or INTERMACS profiles ≤4.
- ATSI populations: Aboriginal and Torres Strait Islander Australians have a 2–3-fold higher burden of heart failure and cardiomyopathy; rheumatic heart disease remains a significant cause of secondary DCM in remote communities. Culturally safe screening and early referral are essential.
- Monitoring: Serial echocardiography at 3–6 months after treatment initiation, then annually. Serial NT-proBNP monitoring helps guide therapy. Multidisciplinary heart failure management programs reduce readmissions and mortality.
Introduction & Australian Epidemiology
Dilated cardiomyopathy (DCM) is a myocardial disorder defined by ventricular chamber enlargement and systolic impairment that is not explained by abnormal loading conditions (hypertension, valve disease) or coronary artery disease sufficient to account for the global dysfunction. The hallmark haemodynamic finding is a reduced left ventricular ejection fraction (LVEF ≤40%), which underlies the clinical syndrome of heart failure with reduced ejection fraction (HFrEF).
DCM is the most common cardiomyopathy globally and the most frequent reason for cardiac transplantation worldwide. The aetiology is heterogeneous — genetic, infectious, toxic, autoimmune, and idiopathic mechanisms all contribute — making systematic diagnostic evaluation essential.
Australian Burden of Disease
- Prevalence: Approximately 1 in 250 to 1 in 500 Australians carry a diagnosis of DCM, though subclinical disease is likely under-detected. The Australian Institute of Health and Welfare (AIHW) reports cardiomyopathies as a significant contributor to the >60,000 annual heart failure hospitalisations nationally.
- Incidence: Population-based Australian data suggest an incidence of approximately 5–8 per 100,000 person-years for new-onset DCM, with higher rates in males and those of lower socioeconomic status.
- Heart failure burden: Heart failure affects an estimated 480,000 Australians; DCM underlies 30–40% of HFrEF cases in Australian tertiary centres. The condition accounts for approximately 2.5% of all hospitalisations in those aged >65 years.
- Transplant data: The Australian and New Zealand Organ Donation Registry (ANZOD) and the Australian & New Zealand Cardiothoracic Transplant Registry report DCM as the leading primary diagnosis in ~45% of adult heart transplant recipients.
- Indigenous Australians: Aboriginal and Torres Strait Islander Australians carry a 2–3-fold excess burden of heart failure, with rheumatic heart disease (RHD) remaining an important cause of secondary cardiomyopathy in remote Northern Territory and Western Australian communities.
- Economic impact: Heart failure costs the Australian healthcare system approximately $2.7 billion annually; DCM-related costs include ongoing pharmacotherapy (PBS expenditure), device implantation, hospital readmissions, and advanced therapies.
Etiology & Diagnosis
A systematic diagnostic approach is essential because the aetiology of DCM influences prognosis, treatment decisions (particularly immunosuppression and device therapy), and the need for family screening. The initial workup must distinguish ischaemic from non-ischaemic DCM and identify potentially reversible or treatable causes.
Ischaemic vs Non-Ischaemic Differentiation
Differentiating ischaemic from non-ischaemic cardiomyopathy is a critical first step because the management pathways, eligibility for revascularisation, and prognosis differ substantially. In ischaemic cardiomyopathy, regional wall motion abnormalities correspond to coronary territories, whereas non-ischaemic DCM typically demonstrates global hypokinesis with or without mid-wall fibrosis.
| Feature | Ischaemic DCM | Non-Ischaemic DCM |
|---|---|---|
| Coronary anatomy | Significant epicardial CAD (≥70% stenosis) or prior MI | Normal or non-obstructive coronaries |
| Wall motion | Regional — corresponding to coronary territory | Global hypokinesis ± regional mid-wall fibrosis pattern |
| LV morphology | May be segmental dilatation with aneurysm | Concentric global dilatation |
| History | Prior MI, angina, PCI/CABG | Variable — may be familial, post-viral, toxic, idiopathic |
| CMR pattern | Subendocardial/transmural LGE in coronary territory | Mid-wall fibrosis (non-territorial LGE), or diffuse oedema (myocarditis) |
| Prognosis | Worse — potential benefit from revascularisation | Generally better 5-year survival if idiopathic |
Comprehensive Aetiological Workup
After excluding coronary artery disease, the following evaluation should be performed to identify reversible or treatable causes:
| Category | Specific Causes | Key Investigations |
|---|---|---|
| Toxic / drug-related | Alcohol (≥80 g/day for >5 years), anthracyclines (doxorubicin, epirubicin), trastuzumab, cocaine, methamphetamine, hydroxychloroquine | Detailed substance and chemotherapy history; urine drug screen |
| Infectious / inflammatory | Viral myocarditis (Coxsackievirus, parvovirus B19, HHV-6, SARS-CoV-2), giant cell myocarditis, cardiac sarcoidosis, eosinophilic myocarditis, Chagas disease, HIV | CMR (oedema, LGE pattern), EMB if indicated; serology (HIV, Trypanosoma); FDG-PET for sarcoidosis |
| Endocrine / metabolic | Hypothyroidism, hyperthyroidism, phaeochromocytoma, acromegaly, thiamine deficiency (beriberi), carnitine deficiency, iron overload (haemochromatosis) | TFTs, 24-hr urinary catecholamines, serum iron studies, echocardiographic iron assessment |
| Autoimmune / systemic | Systemic lupus erythematosus, rheumatoid arthritis, systemic sclerosis, sarcoidosis, vasculitis, eosinophilic granulomatosis with polyangiitis (EGPA) | ANA, anti-dsDNA, RF, anti-CCP, ACE level, ESR, CRP, eosinophil count |
| Infiltrative / storage | Amyloidosis (AL and ATTR), Fabry disease, haemochromatosis | Serum free light chains, technetium-99m pyrophosphate scintigraphy (ATTR), alpha-galactosidase A activity, genetic testing |
| Peripartum | Peripartum cardiomyopathy (last month of pregnancy to 5 months postpartum) | Echocardiography in patients with new heart failure symptoms peri/postpartum |
| Arrhythmia-mediated | Chronic tachycardia (persistent AF, incessant SVT, permanent junctional reciprocating tachycardia) | ECG, Holter; rate control or ablation may reverse DCM |
| Genetic / familial | TTN, LMNA, MYH7, MYBPC3, SCN5A, RBM20, FLNC, DSP, PLN, BAG3, DES variants | Genetic testing panel (see Genetic Testing section) |
| Rheumatic heart disease | Chronic rheumatic carditis with progressive ventricular dilatation — particularly relevant in ATSI communities | Echocardiography (valvular involvement), ASO titre, ESR/CRP |
Diagnostic Imaging Modalities
Myocardial Biopsy — Indications and Utility
Endomyocardial biopsy is an invasive procedure with a complication rate of <1% (perforation, tamponade, arrhythmia). Its utility is highest when histological diagnosis would change management. The 2023 ESC position statement on EMB recommends the following indications:
Biomarkers in Diagnosis
| Biomarker | Role in DCM | Australian Availability / MBS |
|---|---|---|
| NT-proBNP / BNP | Diagnosis of heart failure (rule-out); prognostic marker; guides therapy (target NT-proBNP <1000 pg/mL); serial monitoring | Widely available. MBS item 66407 (BNP). Bulk-billed at most pathology providers. |
| High-sensitivity troponin | Elevated in myocarditis, acute decompensation, and ongoing myocardial injury; helps select patients for EMB | Standard across all Australian hospitals. |
| Serum iron studies | Haemochromatosis screening (ferritin, transferrin saturation); iron deficiency assessment (ferritin <100 or 100–299 with TSAT <20%) — intravenous iron improves symptoms in HFrEF | Standard pathology. MBS item 66571. |
| TFTs (TSH, fT4, fT3) | Exclude thyroid dysfunction — reversible cause of DCM | Standard pathology. |
| Serum free light chains + SPEP/UPEP | Screen for AL amyloidosis in all patients with suspected cardiac amyloidosis | Available at all major pathology providers. |
| hs-CRP / ESR | Non-specific inflammatory markers; elevated in myocarditis, sarcoidosis, autoimmune aetiologies | Standard pathology. |
Treatment Protocols
Management of DCM follows the principles of guideline-directed medical therapy (GDMT) for heart failure with reduced ejection fraction (HFrEF), with additional targeted interventions for specific aetiologies. The 2024 Australian Chronic Heart Failure Clinical Care Standard and Therapeutic Guidelines (eTG) recommend a structured approach to GDMT initiation and uptitration.
Guideline-Directed Medical Therapy (GDMT) — The Four Pillars
Additional Pharmacotherapy
Device Therapy — ICD and CRT
| Device | Indication | Criteria |
|---|---|---|
| ICD — Primary Prevention | Reduce sudden cardiac death in high-risk DCM patients | LVEF ≤35% after ≥3 months optimal GDMT; NYHA II–III; life expectancy >1 year with good functional status. Consider if LVEF ≤30% regardless of NYHA class. |
| ICD — Secondary Prevention | Survivors of cardiac arrest or sustained VT | Cardiac arrest survivor; sustained VT with haemodynamic compromise; syncope with inducible VT at EP study. |
| CRT (CRT-D or CRT-P) | Cardiac resynchronisation for dyssynchrony-related worsening | LVEF ≤35%, LBBB with QRS ≥150 ms, NYHA II–IV despite optimal GDMT, sinus rhythm. CRT-D preferred if also ICD-indicated. Non-LBBB: QRS ≥150 ms considered, weaker evidence. |
Immunosuppression in Inflammatory DCM
Immunosuppressive therapy should be reserved for biopsy-proven inflammatory aetiologies and is not routinely recommended for all DCM patients.
| Condition | Immunosuppressive Regimen | Evidence & Notes |
|---|---|---|
| Giant cell myocarditis | Methylprednisolone 1g IV daily × 3 days → prednisolone 1 mg/kg/day PO, wean over 6–12 months. Add cyclosporine 3–5 mg/kg/day or azathioprine 2 mg/kg/day. | Mandatory — untreated mortality >90% at 1 year. Early transplant referral simultaneously. |
| Eosinophilic myocarditis | Methylprednisolone 500–1000 mg IV daily × 3 days → prednisolone 1 mg/kg/day. Add mepolizumab 300 mg SC 4-weekly for EGPA-related cases. | Identify and treat underlying cause (hypereosinophilic syndrome, EGPA, drug reaction). |
| Cardiac sarcoidosis | Prednisolone 0.5–1 mg/kg/day for 4–8 weeks, then slow taper over 6–12 months. Add methotrexate 10–20 mg/week as steroid-sparing agent if relapsing. | FDG-PET guides treatment initiation and response. Multidisciplinary with respiratory/sarcoidosis team. |
| Lymphocytic myocarditis (viral) | Immunosuppression NOT recommended unless viral PCR negative on biopsy. If autoimmune-negative, viral-positive: consider antivirals. If virus-negative, inflammation-positive: prednisolone 1 mg/kg/day + azathioprine. | TIMIC trial showed benefit of immunosuppression in virus-negative, inflammation-positive lymphocytic myocarditis. |
| Immune checkpoint inhibitor (ICI) myocarditis | Hold ICI immediately. Methylprednisolone 1g IV daily for 3–5 days → prednisolone 1–2 mg/kg/day taper over ≥6 weeks. Add mycophenolate or infliximab for steroid-refractory cases. | High mortality — urgent cardiology-oncology MDT. Re-challenge with ICI is generally contraindicated after grade ≥3 myocarditis. |
Alcohol Cessation in Alcoholic DCM
- Threshold: Significant risk of alcoholic cardiomyopathy with ≥80 g alcohol/day (approximately 8 standard drinks/day) for ≥5 years, though lower cumulative exposure may be sufficient in some individuals.
- Counselling: All patients with suspected alcohol-related DCM should receive structured alcohol counselling and referral to addiction medicine services. The AUDIT-C screening tool should be administered.
- Pharmacological support: Naltrexone (50 mg PO daily) or acamprosate (666 mg PO TDS) for alcohol use disorder — both PBS-listed for this indication. Thiamine supplementation (100 mg PO daily) should be co-prescribed.
- Monitoring: Repeat echocardiography at 3 and 6 months after alcohol cessation to assess for recovery. If LVEF improves to >35%, reassess device candidacy.
- Relapse: Relapse to harmful drinking predicts recurrent LV deterioration. Integrated cardiac and addiction services are essential. Australian data suggest that only ~50% of patients achieve sustained abstinence.
Peripartum Cardiomyopathy
- Defined as heart failure secondary to LV systolic dysfunction (LVEF ≤45%) occurring in the last month of pregnancy or within 5 months of delivery, with no other identifiable cause.
- GDMT principles apply, but ACEi/ARB/ARNI are contraindicated during pregnancy — use hydralazine + nitrates + carvedilol during pregnancy. Sacubitril/valsartan and SGLT2 inhibitors are also contraindicated in pregnancy.
- Bromocriptine (2.5 mg PO BD for 2 weeks, then 2.5 mg daily for 4 weeks) may be considered to inhibit prolactin-driven pathophysiology — supported by small trials. Discuss with cardiologist and obstetrician.
- Approximately 50% of patients recover LVEF to ≥50% within 6–12 months; those who do not should be reclassified as chronic DCM and managed accordingly.
Anthracycline Cardiotoxicity Prevention and Management
- Baseline echocardiography before initiation of anthracycline therapy
- Serial echocardiography during treatment (every 2–4 cycles for high-risk regimens)
- Cumulative dose limits: doxorubicin 450–550 mg/m²; epirubicin 900–1000 mg/m²
- Dexrazoxane (cardioprotectant) for patients receiving high cumulative doses
- Consider liposomal formulations (Caelyx®) for higher-risk patients
- Global longitudinal strain (GLS) on speckle tracking echocardiography — early detection of subclinical cardiotoxicity (>15% relative reduction from baseline)
- Initiate GDMT (ACEi/ARB/ARNI + beta-blocker) immediately upon detection of LVEF decline
- Cardiology-oncology MDT discussion — risk-benefit analysis of continuing chemotherapy
- Trastuzumab-related cardiomyopathy is typically reversible (unlike anthracycline toxicity) — recovery of LVEF occurs in >80% after drug cessation
- Long-term cardiac follow-up for all anthracycline-exposed patients — survivorship care plans per ACSQHC standards
Genetic Testing & Counseling
Genetic factors are increasingly recognised as major contributors to DCM aetiology. Approximately 30–50% of "idiopathic" DCM cases have a genetic basis when systematic testing and family screening are performed. Genetic diagnosis enables targeted family screening, informs prognosis (particularly LMNA variants), guides device decisions, and enables reproductive counselling.
When to Refer for Genetic Testing
Key Genes in DCM
| Gene | Protein / Function | Frequency in Familial DCM | Key Clinical Features | Inheritance |
|---|---|---|---|---|
| TTN | Titin — sarcomere structural protein | ~25% of familial DCM | Most common genetic cause. Truncating variants (TTNtv) predominantly affect A-band. Generally reduced penetrance (~10–20% by age 40). Good prognosis on GDMT. | AD |
| LMNA | Lamin A/C — nuclear envelope | ~6–8% | High-risk gene — conduction disease (AV block), atrial fibrillation, ventricular arrhythmias, aggressive phenotype. Lower threshold for ICD implantation. Consider early EP study. | AD |
| MYH7 | β-myosin heavy chain | ~4–5% | Overlap with hypertrophic cardiomyopathy mutations. Can present with isolated DCM. | AD |
| MYBPC3 | Myosin-binding protein C | ~3–4% | Usually associated with HCM; DCM phenotype less common. | AD |
| FLNC | Filamin C — Z-disc | ~3–5% | Associated with ventricular arrhythmias and fibrosis. Sudden death risk — consider ICD at earlier stage. | AD |
| PLN | Phospholamban — calcium handling | ~1–2% | Aggressive phenotype; risk of end-stage HF and sudden death. Founder variant p.Arg14del particularly malignant. | AD |
| RBM20 | RNA-binding motif protein 20 | ~2–3% | Very aggressive early-onset DCM, high arrhythmia burden, risk of LV thrombus. Early transplant consideration. | AD |
| SCN5A | Cardiac sodium channel | ~2% | Overlap with Brugada syndrome, progressive cardiac conduction defect. DCM + arrhythmia phenotype. | AD |
| DES | Desmin — intermediate filament | ~1–2% | DCM + skeletal myopathy. May have elevated CK. Progressive conduction disease. | AD/AR |
| DSP / DSG2 / PKP2 | Desmosomal proteins | ~2–3% | Arrhythmogenic cardiomyopathy — overlap phenotype with DCM. Arrhythmias, fibrofatty replacement. May mimic DCM on echo. | AD |
| DMD | Dystrophin | X-linked | Duchenne/Becker muscular dystrophy. DCM may be presenting feature before overt myopathy. Female carriers may develop DCM in adulthood. | X-linked |
Interpreting Genetic Test Results
| Result | Clinical Action | Family Implications |
|---|---|---|
| Pathogenic / Likely Pathogenic | Confirmatory for genetic DCM. Guide prognosis (LMNA, PLN, RBM20 = high-risk). Influence ICD threshold. Cascade testing of first-degree relatives. | 50% risk for each offspring. Cascade screening with variant-specific testing. At-risk relatives undergo ECG + echo even if genetic test negative (reduced penetrance). |
| Variant of Uncertain Significance (VUS) | Do NOT use for clinical decision-making. Continue clinical surveillance as if no genetic result. May be reclassified over time as databases grow. | NOT suitable for cascade screening. Re-contact every 1–2 years for reclassification updates. |
| Negative (no pathogenic variant identified) | Does not exclude genetic aetiology (up to 70% of familial DCM remains genetically elusive with current panels). Clinical family screening still recommended. | First-degree relatives should still undergo clinical screening (ECG + echo) given the high rate of genetically unsolved cases. |
Family Cascade Screening Protocol
Australian Genetic Testing Access
| Service | Details |
|---|---|
| State Clinical Genetics Services | Publicly funded genetic counselling and testing for hereditary cardiomyopathies. Available in all states/territories. Wait times vary (2–6 months). Refer through cardiologist or GP. |
| Sonic Genetics / PathWest / VCGS | Cardiomyopathy gene panels (40–100+ genes). Turnaround 6–12 weeks. May be bulk-billed when referred through genetics service; private testing ~$500–800. |
| Australian Genetic Heart Disease Registry | Research registry at Victor Chang Cardiac Research Institute. Facilitates research participation and family contact for genetic studies. |
| MBS Medicare | No dedicated MBS item for cardiomyopathy genetic testing currently. Testing is funded through state hospital genetics services or via research pathways. |
Reproductive Counselling
- Autosomal dominant DCM confers a 50% risk of inheritance for each child. Preimplantation genetic testing (PGT-M) is available in Australia through accredited IVF centres for known pathogenic variants.
- Discuss reproductive options including natural conception with prenatal testing, PGT-M, donor gametes, and adoption.
- Women with DCM (particularly LMNA, RBM20, PLN) must be counselled about pregnancy risks — haemodynamic changes in pregnancy increase risk of decompensation. Multidisciplinary cardio-obstetric care at a tertiary centre is essential.
Prognosis & Monitoring
Prognosis in DCM is highly variable and depends on aetiology, genetic substrate, response to GDMT, and the presence of adverse risk features. Serial monitoring is essential to guide therapeutic escalation and timely referral for advanced heart failure therapies.
Risk Stratification
Prognostic Markers
| Marker | Prognostic Significance | Action Threshold |
|---|---|---|
| NT-proBNP | Strongest independent predictor of mortality in HFrEF. Serial trajectory more important than single value. | Target <1000 pg/mL. Rising levels despite therapy indicate treatment failure or disease progression. |
| LVEF | Baseline LVEF and change with treatment predict outcomes. ≥10% absolute improvement confers survival benefit. | LVEF ≤35% after ≥3 months GDMT → ICD candidacy. Continued decline → advanced therapy referral. |
| CMR mid-wall fibrosis (LGE) | Presence of mid-wall LGE in DCM is an independent predictor of all-cause mortality, sudden death, and ventricular arrhythmias — OR 4.6 for combined events. | LGE-positive DCM: lower ICD implantation threshold; closer monitoring for arrhythmias. |
| Global longitudinal strain (GLS) | GLS >-8% (severely reduced) associated with worse outcomes. More sensitive than LVEF for early deterioration. | Serial GLS monitoring at echocardiography — decline >15% relative change warrants re-evaluation. |
| Renal function (eGFR) | Cardiorenal syndrome — progressive renal impairment predicts poor outcomes. Rapid decline (>20% over 3 months) is ominous. | eGFR <30 mL/min: reassess GDMT doses; consider advanced therapy referral. |
| Hyponatraemia | Serum sodium <135 mmol/L reflects neurohormonal activation and predicts mortality in acute and chronic HF. | Sodium <130 mmol/L: urgent HF specialist review; consider advanced therapies. |
| Genetic substrate | LMNA, PLN, RBM20 variants associated with worse prognosis (faster progression, arrhythmia risk, sudden death). TTNtv generally more benign. | High-risk genotype: ICD at lower LVEF threshold; earlier transplant listing consideration. |
| Exercise capacity (6MWT / CPET) | Peak VO₂ <12 mL/kg/min on cardiopulmonary exercise testing (CPET) indicates advanced HF and poor prognosis. 6-minute walk distance <300 m is also adverse. | Peak VO₂ <14 mL/kg/min: consider transplant listing. Peak VO₂ <12 mL/kg/min: strong indication. |
Serial Monitoring Protocol
Indications for Heart Transplant / LVAD Evaluation
| Indication for Advanced Therapy Referral | Detail |
|---|---|
| Persistent NYHA III–IV despite optimal GDMT | Symptoms limiting daily activities after ≥3 months of maximally tolerated GDMT and device therapy (if indicated). |
| Recurrent HF hospitalisations | ≥2 hospitalisations for acute decompensated heart failure within 12 months despite optimal outpatient therapy. |
| Declining peak VO₂ | Peak VO₂ <14 mL/kg/min (or <50% predicted) on CPET. If <12 mL/kg/min — strong indication for transplant listing. |
| Progressive LVEF decline | Continued decline of LVEF despite uptitrated GDMT; LVEF <20% despite treatment. |
| Inotrope dependence | Requirement for continuous IV inotrope support (milrinone, dobutamine) as bridge to transplant or decision-making. |
| High-risk genotype with progressive phenotype | LMNA, PLN, or RBM20 with aggressive disease trajectory, recurrent VT/VF despite ICD, or rapid functional decline. |
| INTERMACS profiles 1–4 | Profile 1 (crash and burn) through Profile 4 (resting symptoms) indicate need for urgent advanced therapies. LVAD as bridge to transplant or destination therapy. |
Heart Transplantation in Australia
- Approximately 100–130 heart transplants are performed annually in Australia and New Zealand through the ANZOD registry, with DCM as the primary diagnosis in ~45% of recipients.
- Transplant centres: St Vincent's Hospital Sydney, Alfred Hospital Melbourne, Prince Charles Hospital Brisbane, Royal Adelaide Hospital, Fiona Stanley Hospital Perth, and Wellington Hospital (NZ).
- 1-year post-transplant survival exceeds 90% at Australian centres. Median graft survival is approximately 12–14 years.
- Contraindications include active infection, active malignancy, severe irreversible pulmonary hypertension (PVR >6 Wood units despite vasodilator testing), active substance abuse, and severe psychosocial barriers to adherence.
Left Ventricular Assist Device (LVAD)
- LVAD (HeartMate 3® is the current standard) is used as bridge to transplant (BTT), bridge to decision (BTD), or increasingly as destination therapy (DT) in patients ineligible for transplant.
- Available at St Vincent's Hospital Sydney and Alfred Hospital Melbourne.
- 2-year survival with HeartMate 3 is approximately 75–80%. Stroke and device thrombosis rates have improved with contemporary devices.
- Requires intensive anticoagulation management, driveline care, and specialist LVAD centre follow-up. Not all patients are suitable candidates — age, body habitus, and comorbidities are considered.
Recovery of LVEF — Can Therapy Be De-escalated?
Special Populations
Pregnancy
- DCM in pregnancy encompasses pre-existing cardiomyopathy and peripartum cardiomyopathy (PPCM).
- Contraindicated in pregnancy: ACEi, ARB, ARNI, SGLT2i, MRA — all are teratogenic. Must be stopped ideally before conception or immediately upon recognition of pregnancy.
- Safe in pregnancy: Labetalol (200–1200 mg/day PO divided BD-TDS) or metoprolol (50–200 mg/day) for beta-blockade; hydralazine (25–75 mg PO TDS) + long-acting nitrate for afterload reduction; frusemide (use lowest effective dose — monitor amniotic fluid volume).
- Women with LVEF <30% or NYHA III–IV should be counselled that pregnancy carries significant maternal risk (10–20% mortality in severe DCM). Multidisciplinary cardio-obstetric team management at a tertiary centre is essential.
- Mode of delivery: vaginal delivery preferred with assisted second stage (instrumental); caesarean section for obstetric indications or haemodynamic instability.
- Bromocriptine (2.5 mg PO BD for 2 weeks then daily for 4 weeks) may be considered in PPCM — small studies suggest improved recovery. Avoid breastfeeding if using bromocriptine.
- Brestfeeding: ACEi/ARB are compatible with breastfeeding. Enalapril is preferred. SGLT2i: avoid breastfeeding (limited data). Beta-blockers: propranolol and metoprolol are compatible.
Paediatric DCM
- DCM is the most common cardiomyopathy in children (~50–60% of paediatric cardiomyopathies). Incidence: 0.57–1.24 per 100,000 children per year (Australian data).
- Aetiology differs from adults: idiopathic (~50%), myocarditis (~15%), neuromuscular disease (Duchenne/Becker), metabolic/inborn errors of metabolism, and genetic/familial (~25%).
- Age at presentation matters: infants <1 year have higher rates of myocarditis and metabolic aetiology; older children more often have genetic or idiopathic causes.
- GDMT adaptation: Enalapril (0.1 mg/kg PO BD, titrate to 0.5 mg/kg BD) — standard paediatric ACEi. Carvedilol (0.05 mg/kg PO BD, titrate to 0.4 mg/kg BD) — limited paediatric RCT evidence but used in Australian paediatric HF centres. SGLT2i: NOT approved for paediatric use in heart failure.
- Spironolactone: 1–2 mg/kg/day PO. Frusemide: 0.5–2 mg/kg/day PO.
- ICD in children: indicated for secondary prevention or high-risk primary prevention (LMNA with significant conduction disease). Primary prevention ICD in children is challenging due to size constraints — subcutaneous ICD may be considered in older children.
- Referral to paediatric cardiology at a tertiary centre (e.g., Royal Children's Hospital Melbourne, Children's Hospital Westmead, Queensland Children's Hospital) for all newly diagnosed cases.
- Genetic testing is particularly valuable in paediatric DCM — high yield for pathogenic variants, especially if diagnosed <1 year of age.
Elderly
- DCM in the elderly (≥75 years) is often multifactorial — age-related myocardial remodelling, long-standing hypertension, ischaemic heart disease, and tachycardia-mediated cardiomyopathy from AF all contribute.
- GDMT initiation requires careful dose adjustment and monitoring — start at lowest doses and titrate slowly. Hypotension and renal impairment are common barriers.
- Polypharmacy: review all medications for interactions and deprescribe where appropriate. Avoid NSAIDs which worsen fluid retention and renal function.
- ICD decision-making: balance life expectancy and comorbidities. Patients with limited life expectancy (<1 year) or severe frailty may not benefit from primary prevention ICD.
- Frailty assessment (Clinical Frailty Scale) should inform treatment intensity and advance care planning. Shared decision-making is particularly important.
- Heart failure management programs and TeleHF monitoring (available through state health services) can reduce emergency presentations and support community-based care.
Renal Impairment
- Cardiorenal syndrome is common in DCM — worsening renal function reflects low cardiac output and venous congestion, and independently predicts mortality.
- ACEi/ARB/ARNI: Use with caution if eGFR <30 mL/min. Avoid if eGFR <20. Monitor K⁺ and creatinine within 1–2 weeks of initiation or dose change. Accept up to 30% rise in creatinine — do not discontinue unless K⁺ >6.0 or acute kidney injury.
- MRA: Avoid if eGFR <30 or K⁺ >5.0. Higher hyperkalaemia risk when combined with ARNI.
- SGLT2i: Can initiate if eGFR ≥20 mL/min for heart failure indication (dapagliflozin PBS requires eGFR ≥25). The diuretic effect may reduce loop diuretic requirements.
- Diuretics: May need higher doses or combination (frusemide + metolazone) in advanced renal impairment. Monitor volume status and renal function weekly during titration.
- Haemodialysis patients with DCM: management is complex and requires nephrology-cardiology co-management. Ultrafiltration targets and dry weight optimization are key.
Hepatic Impairment
- Congestive hepatopathy is common in advanced DCM — hepatic congestion leads to elevated LFTs (typically AST/ALT 2–3× normal, raised ALP/GGT). Cardiac cirrhosis may develop with chronic right heart failure.
- ACEi/ARB: use with caution in hepatic impairment — enalapril does not require hepatic dose adjustment. Sacubitril/valsartan: limited data in severe hepatic impairment (Child-Pugh C); use with caution.
- Spironolactone: may accumulate in hepatic impairment — start at lowest dose and monitor closely. Eplerenone: avoid if Child-Pugh C.
- Carvedilol: extensively hepatically metabolised — use cautiously; consider dose reduction in significant hepatic impairment.
- Warfarin (if indicated for AF): requires careful INR monitoring — increased sensitivity in hepatic congestion.
Immunocompromised
- HIV-associated cardiomyopathy: DCM occurs in 10–15% of people living with HIV (PLWH), mediated by direct viral myocardial injury, chronic inflammation, antiretroviral toxicity, and opportunistic infections. Echocardiographic screening is recommended for PLWH with new cardiac symptoms.
- Treatment: GDMT applies. Optimise antiretroviral therapy. Consider EMB to exclude specific opportunistic causes (Toxoplasma, CMV, Cryptococcus) if immunosuppressed with acute cardiomyopathy.
- Transplant candidates: HIV-positive patients can undergo heart transplantation with good outcomes if viral load is undetectable and CD4 count >200 cells/µL on stable ART.
- Post-transplant immunosuppression: standard regimens (tacrolimus + mycophenolate + prednisolone) are used with close HIV virological monitoring. Drug interactions between calcineurin inhibitors and protease inhibitors require careful dose adjustment.
- Immune checkpoint inhibitor (ICI) cardiomyopathy: increasingly recognised in oncology patients. Prompt cessation of ICI and urgent cardiology referral for immunosuppression. See Treatment Protocols section for management.
Aboriginal and Torres Strait Islander Health Considerations
Aboriginal and Torres Strait Islander Australians experience a disproportionate burden of cardiovascular disease and heart failure. Culturally safe, evidence-based approaches to DCM management are essential to reduce health inequity and improve outcomes.
📚 References
- 1. Heidenreich PA, Bozkurt B, Aguilar D, et al. 2022 AHA/ACC/HFSA Guideline for the Management of Heart Failure: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation. 2022;145(18):e895–e1032.
- 2. McDonagh TA, Metra M, Adamo M, et al. 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure. Eur Heart J. 2021;42(36):3599–3726.
- 3. Bozkurt B, Colvin M, Cook J, et al. Current Diagnostic and Treatment Strategies for Specific Dilated Cardiomyopathies: A Scientific Statement from the American Heart Association. Circulation. 2016;134(23):e579–e646.
- 4. > Weintraub RG, Semsarian C, Macdonald P. Dilated cardiomyopathy. Lancet. 2017;390(10092):400–414.
- 5. Hershberger RE, Givertz MM, Ho CY, et al. Genetic Evaluation of Cardiomyopathy—A Heart Failure Society of America Practice Guideline. J Card Fail. 2018;24(5):281–302.
- 6. Verdonschot JAJ, Hazebroek MR, Derks KWJ, et al. Titin cardiomyopathy phenotype varies with titin variant type. J Am Coll Cardiol. 2018;72(17):2053–2054.
- 7. Pinto YM, Elliott PM, Arbustini E, et al. Proposal for a revised definition of dilated cardiomyopathy, hypokinetic non-dilated cardiomyopathy, and its implications for clinical practice: a position statement of the ESC Working Group on Myocardial and Pericardial Diseases. Eur Heart J. 2016;37(23):1850–1858.
- 8. Halliday BP, Wassall R, Lota AS, et al. Withdrawal of pharmacological treatment for heart failure in patients with recovered dilated cardiomyopathy (TRED-HF): an open-label, pilot, randomised trial. Lancet. 2019;393(10166):61–73.
- 9. Caforio AL, Pankuweit S, Arbustini E, et al. Current state of knowledge on aetiology, diagnosis, management, and therapy of myocarditis: a position statement of the European Society of Cardiology Working Group on Myocardial and Pericardial Diseases. Eur Heart J. 2013;34(33):2636–2648.
- 10. Australian Institute of Health and Welfare. Heart, stroke and vascular disease — Australian facts. AIHW, Canberra; 2023.
- 11. Australian Commission on Safety and Quality in Health Care. Chronic Heart Failure Clinical Care Standard. ACSQHC, Sydney; 2024.
- 12. RHDAustralia (ARF/RHD writing group). National guideline for the prevention, diagnosis and management of acute rheumatic fever and rheumatic heart disease. 3rd ed. Darwin: Menzies School of Health Research; 2020.
- 13. Gulati G, Japp AG, Raza S, et al. Absence of myocardial fibrosis predicts favourable long-term survival in new-onset heart failure. Circ Cardiovasc Imaging. 2018;11(3):e007250.
- 14. > Januzzi JL Jr, Butler J, Zannad F, et al. Prognostic importance of NT-proBNP trajectory on sacubitril/valsartan treatment in patients with heart failure and reduced ejection fraction. JACC Heart Fail. 2021;9(11):814–824.
- 15. Ponikowski P, Voors AA, Anker SD, et al. 2016 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure. Eur Heart J. 2016;37(27):2129–2200.
- 16. Crespo-Leiro MG, Costanzo MR, Gustafsson F, et al. Advanced heart failure: a position statement of the Heart Failure Association of the European Society of Cardiology. Eur J Heart Fail. 2018;20(11):1505–1535.
- 17. Sahni S, Abegaz B, Brown NJ. Peripartum cardiomyopathy: a review. Aust N Z J Obstet Gynaecol. 2023;63(1):17–26.
- 18. Australian and New Zealand Society of Cardiac and Thoracic Surgeons (ANZSCTS). ANZSCTS Cardiac Surgery Database Project — Heart Transplant Report. Melbourne; 2023.
- 19. James PA, Semsarian C. Sudden cardiac death in the young: the increasing role of genetic testing. Med J Aust. 2023;218(7):303–309.
- 20. Semsarian C, Ingles J. Genetic testing in cardiomyopathies — practical considerations for the clinician. Heart Lung Circ. 2022;31(1):23–30.