📋 Key Information Summary
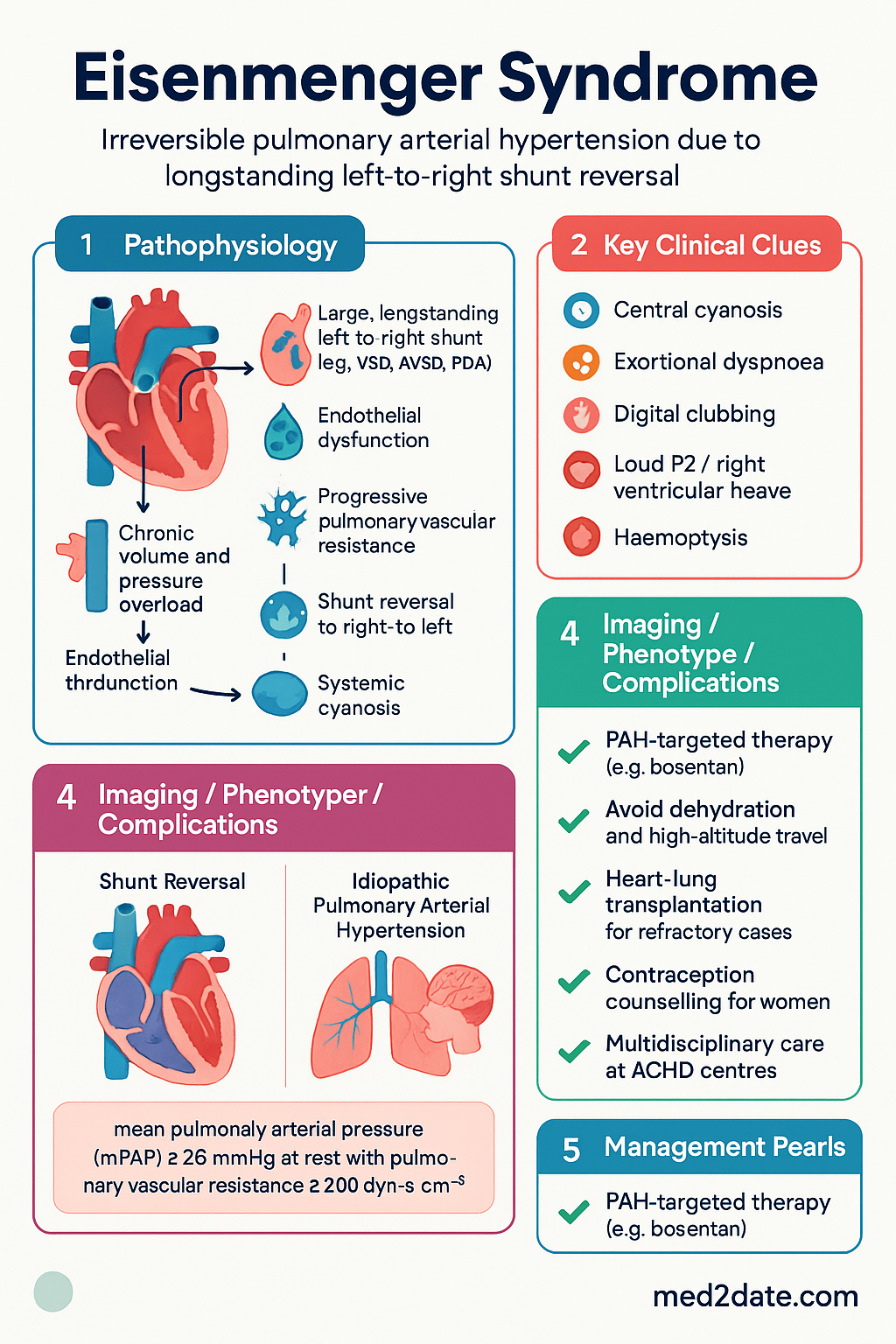
- Eisenmenger syndrome (ES) is irreversible pulmonary arterial hypertension (PAH) caused by a large, longstanding left-to-right shunt that has reversed to bidirectional or right-to-left shunting, resulting in central cyanosis.
- Most commonly arises from unrepaired large ventricular septal defect (VSD), atrioventricular septal defect (AVSD), or patent ductus arteriosus (PDA) — typically presenting in the second to fourth decade of life in Australia.
- Diagnosis requires: (1) an underlying congenital systemic-to-pulmonary shunt, (2) severe PAH with pulmonary vascular resistance >800 dyn·s·cm⁻⁵, and (3) bidirectional or right-to-left shunting at rest.
- Closure of the underlying defect is CONTRAINDICATED once Eisenmenger physiology is established — surgical or percutaneous closure worsens right ventricular failure and may be fatal.
- Doppler echocardiography is the primary non-invasive diagnostic tool; right heart catheterisation is the gold standard for confirming haemodynamics and reversibility testing.
- Complications include haemoptysis (most common cause of death), brain abscess, stroke, arrhythmias (particularly atrial), iron-deficiency anaemia, gout, cholelithiasis, and erythrocytosis with hyperviscosity.
- PAH-targeted therapy (endothelin receptor antagonists, PDE-5 inhibitors, prostanoids) improves functional class and exercise capacity — bosentan has the strongest trial evidence in ES (BREATHE-5 trial).
- Avoid dehydration, phlebotomy (unless symptomatic hyperviscosity with haematocrit >65%), high-altitude travel, general anaesthesia where possible, and nephrotoxic agents.
- Heart–lung transplantation or bilateral lung transplantation with intracardiac repair is the definitive treatment for refractory disease; timing of referral is critical (NYHA III–IV, recurrent haemoptysis).
- Women with Eisenmenger syndrome have a 30–50% maternal mortality rate with pregnancy — contraception counselling and avoidance of oestrogen-containing preparations is essential.
- Pregnancy is absolutely contraindicated (WHO Category IV); long-acting reversible contraception (LARC) with progesterone-only methods or copper IUD is recommended.
- Endocarditis prophylaxis is no longer routinely recommended per ESC/AHA 2020 guidelines, but should be considered on a case-by-case basis in prosthetic material or prior endocarditis.
- Iron-deficiency anaemia must be corrected with intravenous iron (avoid phlebotomy); routine venesection is harmful and worsens hyperviscosity symptoms.
- Multidisciplinary care at a specialised adult congenital heart disease (ACHD) centre (e.g., Royal Adelaide Hospital, Westmead Hospital, Monash Heart) is essential for ongoing management.
Introduction & Australian Epidemiology
Eisenmenger syndrome is a severe, progressive condition characterised by irreversible pulmonary arterial hypertension (PAH) arising from a longstanding, large congenital systemic-to-pulmonary shunt. The progressive rise in pulmonary vascular resistance ultimately exceeds systemic vascular resistance, causing shunt reversal to bidirectional or right-to-left flow. The resultant central cyanosis and multi-organ sequelae define the syndrome.
The condition was first described by Paul Wood in 1958, building on Victor Eisenmenger's original 1897 case report of a patient with a large VSD and pulmonary hypertension. Eisenmenger syndrome represents the end-stage consequence of unrepaired congenital heart disease (CHD) and is now increasingly seen in low- and middle-income countries or in patients whose defects were undiagnosed or managed conservatively in the pre-surgical era.
Australian epidemiology:
- The prevalence of Eisenmenger syndrome has declined dramatically in Australia due to universal neonatal screening, early echocardiographic diagnosis, and timely surgical repair of large defects.
- An estimated 200–400 adults with Eisenmenger syndrome are living in Australia, managed primarily through specialised Adult Congenital Heart Disease (ACHD) centres.
- Median age at diagnosis in Australian cohorts is 25–35 years; patients born before the era of routine paediatric cardiac surgery (pre-1980s) are the most affected.
- VSD (40–50%) is the most common underlying defect, followed by AVSD (20–25%), PDA (10–15%), and ASD (rarely — only large, longstanding secundum or primum defects).
- In Aboriginal and Torres Strait Islander communities, delayed access to paediatric cardiac services in remote and regional areas may contribute to higher rates of undiagnosed CHD and late presentation (see ATSI section).
- Survival has improved with PAH-targeted therapies: 10-year survival is approximately 70–80% with modern treatment compared to 40–50% in historical series.
- Key Australian referral centres include the Adult Congenital Heart Disease service at Royal Adelaide Hospital, Westmead Adult Congenital Heart Centre (Sydney), Monash Heart (Melbourne), and the Queensland Adult Congenital Heart Service.
Pathophysiology (Shunt Reversal)
The pathophysiology of Eisenmenger syndrome is a progressive, staged process driven by chronic volume and pressure overload of the pulmonary vasculature.
Stages of Pulmonary Vascular Remodelling
Key Pathophysiological Concepts
| Mechanism | Consequence | Clinical Relevance |
|---|---|---|
| Endothelial dysfunction | Reduced NO, prostacyclin; increased endothelin-1, thromboxane A₂ | Target for PAH-specific therapy (bosentan, sildenafil, epoprostenol) |
| Plexiform arteriopathy | Obliterative lesions in small pulmonary arteries | Irreversible — explains why shunt closure is contraindicated |
| Right-to-left shunting | Systemic desaturation, erythrocytosis, secondary polycythaemia | Iron deficiency worsens hyperviscosity despite lower Hb |
| RV pressure overload | RV hypertrophy → dilatation → systolic failure | Prognostic marker; serial echo assessment essential |
| Chronic hypoxaemia | Clubbing, gout, cholelithiasis, coagulopathy | Multi-organ complications drive morbidity |
| Thrombotic tendency | In-situ pulmonary artery thrombosis, paradoxical embolism | Anticoagulation controversial — case-by-case decision |
Clinical Features & Complications
Presenting Features
Patients typically present in the second to fourth decade with progressive exertional dyspnoea and central cyanosis. The clinical presentation is heterogeneous and depends on the degree of shunt reversal, compensatory erythrocytosis, and downstream organ damage.
| Symptom / Sign | Mechanism | Prevalence |
|---|---|---|
| Central cyanosis | Right-to-left shunting, desaturated blood reaching systemic circulation | 100% |
| Exertional dyspnoea | Reduced cardiac output, increased R→L shunt during exercise | 90–95% |
| Digital clubbing | Chronic hypoxaemia, capillary proliferation | 70–80% |
| Fatigue / exercise intolerance | Low cardiac output, impaired oxygen delivery | 80–90% |
| Haemoptysis | Rupture of fragile bronchial collaterals or pulmonary arterioles | 20–30% |
| Palpitations / syncope | Arrhythmias (atrial flutter/fibrillation), reduced cerebral perfusion | 25–35% |
| Peripheral oedema | Right ventricular failure, elevated CVP | 30–50% |
| Loud P2 / right ventricular heave | Pulmonary hypertension, RV hypertrophy | 95% |
| Systolic murmur (tricuspid regurgitation) | RV dilatation, annular dilatation | 60–70% |
Major Complications
Additional Complications
- Arrhythmias: Atrial flutter and fibrillation occur in 20–40%; ventricular arrhythmias are less common but carry high mortality. Treatment is challenging — digoxin and beta-blockers may worsen RV function.
- Stroke / paradoxical embolism: Right-to-left shunt permits venous thrombi to enter systemic circulation. Annual stroke risk 1–3%.
- Paradoxical embolism via PFO or septal defect: Deep venous thrombosis must be aggressively treated and prevented.
- Iron-deficiency anaemia: Occurs in up to 30% of patients due to chronic consumption, phlebotomy, GI bleeding, or menorrhagia. Confounds the clinical picture by lowering Hb while worsening hyperviscosity through microcytosis.
- Hyperuricaemia and gout: Increased red cell turnover leads to hyperuricaemia; gout flares occur in 10–20% of patients.
- Cholelithiasis: Bilirubin overproduction from chronic haemolysis causes pigment gallstones.
- Renal dysfunction: Chronic hypoxaemia, reduced renal blood flow, and renal tubular acidosis. Nephrolithiasis from hyperuricosuria.
- Coagulopathy: Paradoxical combination of thrombotic tendency (in-situ PA thrombosis) and bleeding risk (thrombocytopenia, acquired von Willebrand syndrome).
- Infective endocarditis: Risk persists with turbulent flow across the defect.
Investigations & Diagnosis
Diagnostic Criteria
Diagnosis of Eisenmenger syndrome requires all three of:
- An underlying congenital systemic-to-pulmonary shunt (VSD, AVSD, PDA, ASD, or complex CHD)
- Severe PAH — mean pulmonary arterial pressure (mPAP) ≥25 mmHg at rest with pulmonary vascular resistance >800 dyn·s·cm⁻⁵ (10 Wood units)
- Bidirectional or right-to-left shunting at rest (cyanosis, SpO₂ <95% room air)
Baseline & Ongoing Investigations
Management — PAH Therapy, Transplant & Supportive Care
General Principles & Avoidance Measures
- All care should be coordinated through a specialised ACHD centre with PAH expertise.
- Avoid dehydration (reduces preload, worsens R→L shunt).
- Avoid high-altitude travel (>1500 m) — reduced FiO₂ worsens hypoxaemia and increases PVR.
- Avoid strenuous isometric exercise; encourage moderate aerobic activity within symptom limits.
- Use local or regional anaesthesia where possible; general anaesthesia carries very high risk.
- Pre-operative assessment for any procedure must include anaesthetic/cardiology review at an ACHD centre.
- Annual influenza vaccination and pneumococcal vaccination (per ATAGI schedule).
- Smoking cessation — absolute requirement.
PAH-Targeted Therapy
Three major pathways are targeted by current PAH therapies: the endothelin pathway, the NO–cGMP pathway, and the prostacyclin pathway. Evidence in Eisenmenger syndrome, while extrapolated from broader PAH trials, supports initiation of therapy in symptomatic patients (WHO/NYHA functional class II–IV).
Combination Therapy Strategy
Current ESC/ERS guidelines recommend initial combination therapy (ERA + PDE-5 inhibitor) for PAH patients in WHO/NYHA functional class II–IV, with escalation to triple therapy (adding prostanoid) if response is inadequate. This strategy is applied to Eisenmenger syndrome patients based on extrapolation and expert consensus:
Management of Specific Complications
| Complication | Management |
|---|---|
| Iron-deficiency anaemia | IV iron infusion (ferric carboxymaltose 500–1000 mg IV, or iron polymaltose). Target ferritin >50 µg/L, TSAT >20%. Avoid oral iron (poor absorption, GI intolerance). NEVER venesection for anaemia. |
| Symptomatic erythrocytosis | Phlebotomy ONLY if symptomatic hyperviscosity (headache, visual changes, TIA-like symptoms) AND Hct >65%. Remove 250–500 mL, replace with isovolumic normal saline. Target Hct 55–60%. Ensure iron replete first. |
| Haemoptysis | Mild: observation, tranexamic acid 1 g IV/PO. Moderate–massive: ICU, transfusion, bronchial artery embolisation (interventional radiology). Urgent transplant reassessment. |
| Atrial arrhythmias | DC cardioversion for haemodynamic instability. Rate control with diltiazem or low-dose beta-blocker (caution — may reduce CO). Amiodarone for rhythm control. Avoid class IC agents. |
| Gout | Colchicine 500 µg OD prophylaxis; acute flares: colchicine 500 µg stat then 250 µg hourly (max 3 mg/day) or NSAIDs (short courses with caution). Allopurinol for chronic hyperuricaemia — adjust for renal function. |
| Brain abscess | IV metronidazole 400–500 mg TDS + ceftriaxone 2 g BD (or meropenem 1 g TDS if penicillin allergy). Neurosurgical drainage/aspiration. 6–8 weeks total antibiotics. MRI surveillance. |
| Anticoagulation | Not routinely recommended. Consider in: in-situ PA thrombosis, AF/Flutter (with extreme caution — bleeding risk), prior thromboembolic event. Use warfarin (INR 1.5–2.5) — DOACs less studied. Assess bleeding risk case-by-case. |
Transplantation
Heart–lung transplantation (HLT) or bilateral lung transplantation (BLT) with intracardiac repair is the only definitive treatment for Eisenmenger syndrome refractory to medical therapy. Transplant listing in Australia is managed through the Transplantation Society of Australia and New Zealand (TSANZ).
- NYHA/WHO FC III–IV despite optimal PAH therapy
- Recurrent or life-threatening haemoptysis
- Peak VO₂ <10.6 mL/kg/min on CPET
- RV failure with progressive dilatation/dysfunction
- Syncope or refractory arrhythmias
- Progressive renal or hepatic dysfunction
- NT-proBNP >1400 pg/mL (rising trend)
- Bilateral lung transplant + intracardiac repair: Preferred when RV is recoverable (preserved RV function at transplant assessment). Defect is closed at the time of transplant.
- Heart–lung transplant: Reserved for severe biventricular failure or complex anatomy not amenable to repair. Limited donor availability is the major barrier.
- Post-transplant outcomes in ES: 1-year survival ~75–80%, 5-year survival ~50–60% (comparable to other PAH transplant indications).
Perioperative & Procedural Risk
Any surgical or procedural intervention in Eisenmenger syndrome carries extremely high mortality risk (estimated 7–30% for non-cardiac surgery). Key principles:
- Elective surgery should be avoided where possible.
- All procedures require pre-assessment at an ACHD centre with anaesthetic and cardiology input.
- Regional anaesthesia preferred over general anaesthesia when feasible.
- Avoid epidural anaesthesia if coagulopathy or thrombocytopenia present.
- Intraoperative monitoring: arterial line, central venous access, transoesophageal echocardiography.
- Maintain preload, avoid hypotension, avoid air bubbles in IV lines (paradoxical embolism risk).
- Postoperative HDU/ICU monitoring mandatory.
Special Populations
Aboriginal and Torres Strait Islander Health Considerations
Aboriginal and Torres Strait Islander peoples experience a higher burden of congenital heart disease and its complications, including Eisenmenger syndrome, due to systemic inequities in healthcare access, delayed diagnosis, and barriers to specialist cardiac services in remote and regional communities.
📚 References
- 1. Galiè N, Humbert M, Vachiery JL, et al. 2015 ESC/ERS Guidelines for the diagnosis and treatment of pulmonary hypertension. Eur Heart J. 2016;37(1):67–119.
- 2. Galie N, Beghetti M, Gatzoulis MA, et al. Bosentan therapy in patients with Eisenmenger syndrome: a multicentre, double-blind, randomised, placebo-controlled study (BREATHE-5). Circulation. 2006;114(1):48–54.
- 3. Baumgartner H, De Backer J, Babu-Narayan SV, et al. 2020 ESC Guidelines for the management of adult congenital heart disease. Eur Heart J. 2021;42(6):563–645.
- 4. Diller GP, Kempny A, Inuzuka R, et al. Survival prospects of treatment naïve patients with Eisenmenger syndrome: a systematic review of the literature and report of own experience. Heart. 2014;100(19):1489–1496.
- 5. Stout KK, Daniels CJ, Aboulhosn JA, et al. 2018 AHA/ACC Guideline for the Management of Adults With Congenital Heart Disease. Circulation. 2019;139(14):e698–e800.
- 6. Australian Institute of Health and Welfare (AIHW). Congenital heart disease in Australia. Cat. no. CDK 7. Canberra: AIHW; 2019.
- 7. Ladouceur M, Benoit L, Radojevic J, et al. Pregnancy outcomes in patients with pulmonary arterial hypertension associated with congenital heart disease. Heart. 2017;103(4):282–288.
- 8. Kaemmerer H, Mebus S, Schulze-Neick I, et al. The adult patient with Eisenmenger syndrome: a medical update after the Dana Meeting Part 1: epidemiology, clinical aspects and diagnostic options. Int J Cardiol. 2010;145(2):195–198.
- 9. RHDAustralia (ARF/RHD Program). The 2020 Australian guideline for prevention, diagnosis and management of acute rheumatic fever and rheumatic heart disease (3rd edition). Darwin: Menzies School of Health Research; 2020.
- 10. Mocumbi AO, Lameira E, Yaksh A, et al. Challenges on the management of congenital heart disease in developing countries. Int J Cardiol. 2011;148(3):285–288.
- 11. Australian Commission on Safety and Quality in Health Care (ACSQHC). National Safety and Quality Health Service Standards. 2nd ed. Sydney: ACSQHC; 2017.
- 12. Pulido T, Adzerikho I, Channick RN, et al. Macitentan and morbidity and mortality in pulmonary arterial hypertension (SERAPHIN). N Engl J Med. 2013;369(9):809–818.
- 13. Ghofrani HA, Galiè N, Grimminger F, et al. Riociguat for the treatment of pulmonary arterial hypertension (PATENT-1). N Engl J Med. 2013;369(4):330–340.
- 14. Sitbon O, Channick R, Chin KM, et al. Selexipag for the treatment of pulmonary arterial hypertension (GRIPHON). N Engl J Med. 2015;373(26):2522–2533.
- 15. Heart Foundation of Australia. Living well with a heart condition — pulmonary hypertension consumer guide. Melbourne: National Heart Foundation of Australia; 2021.