📋 Key Information Summary
- Constrictive pericarditis (CP) results from a thickened, fibrotic, and often calcified pericardium that restricts diastolic filling, producing signs of right-heart failure with preserved systolic function.
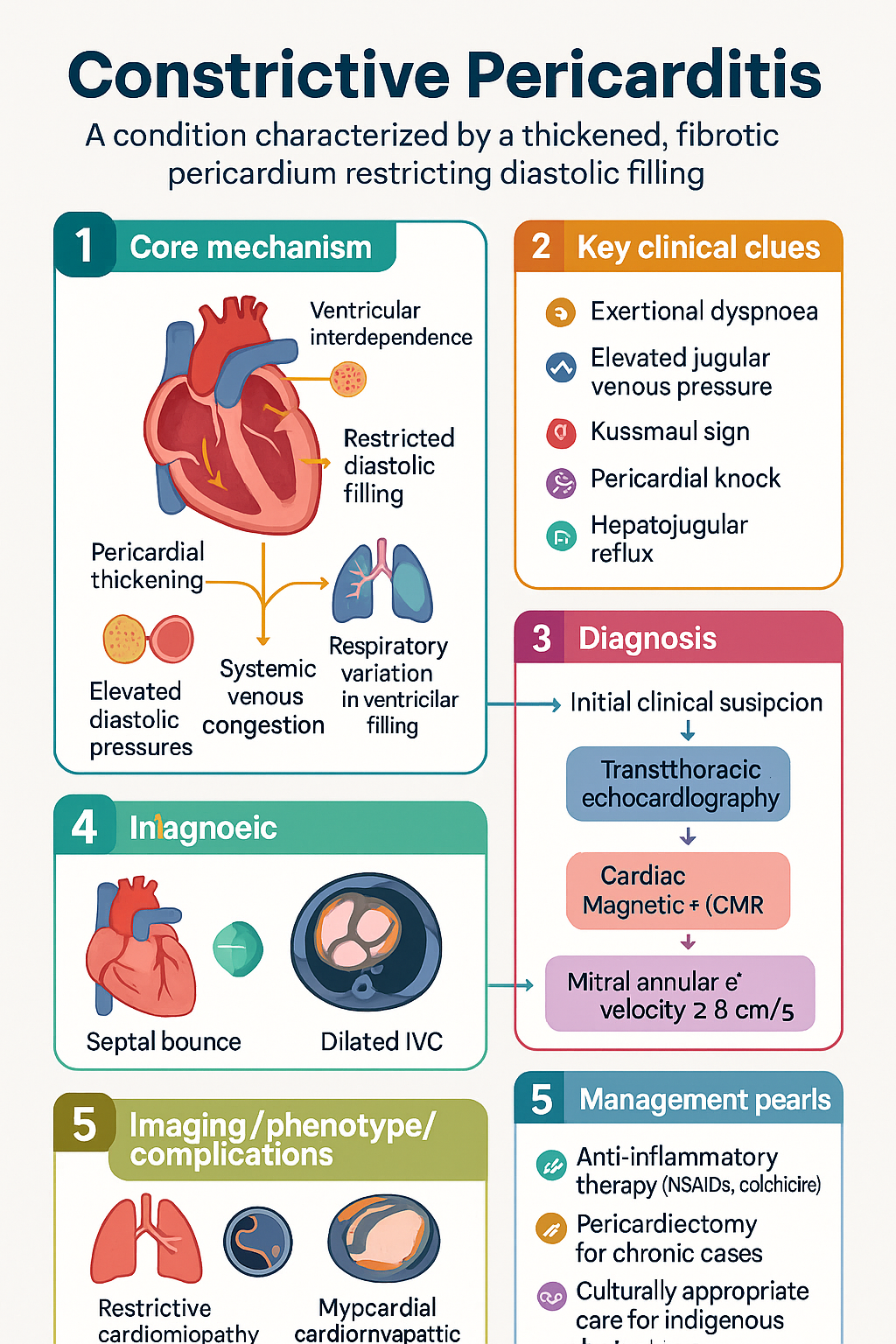
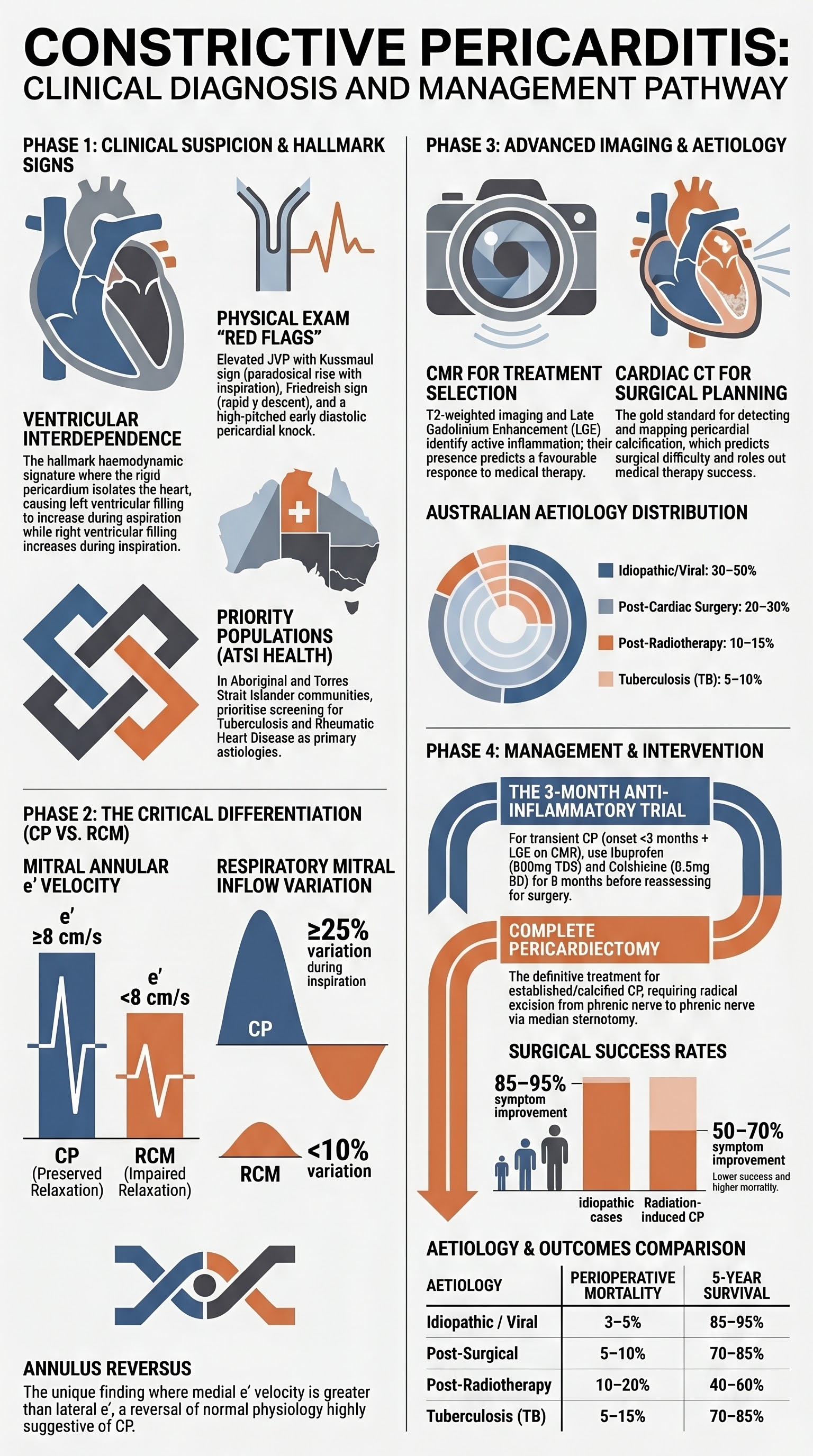
- The hallmark haemodynamic feature is ventricular interdependence — left ventricular (LV) filling increases during expiration while right ventricular (RV) filling increases during inspiration, producing discordant ventricular pressure changes.
- Differentiation from restrictive cardiomyopathy (RCM) is the single most important diagnostic challenge; echocardiographic tissue Doppler, mitral annular e′ velocity ≥8 cm/s, and CMR are key discriminators.
- Transthoracic echocardiography (TTE) is the first-line investigation; look for septal bounce, respiratory variation in mitral inflow velocity ≥25%, dilated IVC with preserved inspiratory collapse, and enhanced hepatic vein diastolic flow reversal in expiration.
- Cardiac magnetic resonance (CMR) with late gadolinium enhancement (LGE) identifies pericardial thickening (>4 mm), inflammation (oedema on T2-weighted imaging), and fibrosis, guiding candidacy for anti-inflammatory therapy versus surgery.
- CT calcium scoring of the pericardium complements CMR when heavy calcification is suspected and helps surgical planning.
- Common aetiologies include idiopathic/viral (most common in Australia), post-cardiac surgery, post-radiotherapy (especially breast and Hodgkin lymphoma), tuberculosis, autoimmune/connective-tissue diseases, and uraemia.
- Transient (effusive-constrictive) pericarditis may respond to a 2–3 month trial of anti-inflammatory therapy (NSAIDs ± colchicine ± corticosteroids) before committing to surgery.
- CMR evidence of pericardial oedema/inflammation with LGE predicts a favourable response to medical therapy; the absence of inflammation and the presence of calcification predict failure and the need for pericardiectomy.
- Complete (total) pericardiectomy is the definitive treatment for chronic, established CP; the procedure carries 5–10% perioperative mortality in experienced centres but achieves symptomatic improvement in 80–90% of patients.
- Surgery should be performed at a centre with high-volume pericardial disease expertise; incomplete pericardiectomy is associated with persistent symptoms and higher mortality.
- Aboriginal and Torres Strait Islander Australians may have higher rates of rheumatic heart disease and tuberculosis-related pericardial constriction, requiring culturally appropriate screening and management pathways.
Introduction & Australian Epidemiology
Constrictive pericarditis (CP) is an uncommon but serious condition characterised by a loss of pericardial compliance due to chronic fibrosis, thickening, and often calcification of the pericardium. The rigid pericardial shell impairs diastolic ventricular filling, leading to elevated and equalised diastolic pressures in all cardiac chambers, systemic venous congestion, and clinical features of right-sided heart failure.
CP accounts for a significant proportion of unexplained right-heart failure referrals in Australia and may be underdiagnosed due to subtle early presentation. The reported incidence in Western populations is approximately 0.2–0.4 per 1 000 hospital admissions, though true population-level data for Australia are limited. A single-centre Australian series from the Royal Melbourne Hospital found idiopathic/viral and post-cardiac surgery aetiologies to be the most common causes.
Internationally, tuberculosis remains the leading cause of CP in endemic regions (South-East Asia, sub-Saharan Africa); in Australia, it accounts for a small but clinically important minority of cases, particularly in Aboriginal and Torres Strait Islander communities and among migrants from high-burden countries. The Australian Institute of Health and Welfare (AIHW) reports an overall TB notification rate of 5–6 per 100 000 nationally, with higher rates in the Northern Territory and among Indigenous Australians.
Post-radiotherapy CP is an increasingly recognised long-term complication as cancer survivorship improves, particularly following mantle-field radiotherapy for Hodgkin lymphoma and adjuvant radiotherapy for left-sided breast carcinoma.
Diagnosis & Differentiation
Haemodynamic Principles
The pathophysiological hallmark of CP is dissociation between intrathoracic and intracardiac pressures. Because the thickened pericardium isolates the heart from respiratory changes in intrathoracic pressure, the normal augmentation of venous return to the right heart during inspiration does not transmit to the left heart. This produces ventricular interdependence — the defining haemodynamic signature of CP.
Haemodynamic Criteria (Cardiac Catheterisation)
| Parameter | Constrictive Pericarditis | Restrictive Cardiomyopathy |
|---|---|---|
| LV and RV end-diastolic pressures | Equalised (within 5 mmHg) | LV > RV by >5 mmHg |
| Ventricular interdependence | Present (discordant LV/RV systolic pressures) | Absent |
| RVEDP / RVSP ratio | ≥1/3 | <1/3 |
| Dip-and-plateau (square root sign) | Present in both ventricles | Present (LV predominant) |
| PCWP vs LVEDP | PCWP ≈ LVEDP | PCWP > LVEDP (prominent V wave) |
| Myocardial relaxation index (tau) | Normal | Prolonged |
Key Differentiating Features: CP vs RCM
Differentiating CP from restrictive cardiomyopathy (RCM) is critical because the management pathways diverge sharply — CP is potentially curable with surgery, while RCM is managed medically or with transplantation.
| Feature | CP | RCM |
|---|---|---|
| Kussmaul sign | Often present | Usually absent |
| Pericardial knock | Present (early diastolic sound) | Absent (S3 may be present) |
| Mitral annular e′ (tissue Doppler) | ≥8 cm/s (lateral); medial e′ > lateral e′ (annulus reversus) | <8 cm/s |
| E/e′ ratio | Usually normal (<15) | Often elevated (>15) |
| Respiratory mitral inflow variation | ≥25% decrease during inspiration | <10% variation |
| Pericardial thickness (CT/CMR) | >4 mm (up to 20 mm) | Normal (≤2 mm) |
| Myocardial LGE on CMR | Absent (unless coexistent) | Often present (subendocardial, amyloid pattern) |
| Biopsy | Myocardium normal | Myocardial infiltrate (amyloid, sarcoid, fibrosis) |
Clinical Features
- Exertional dyspnoea progressing to dyspnoea at rest
- Peripheral oedema, ascites, hepatomegaly (right-heart failure predominant)
- Elevated jugular venous pressure (JVP) with prominent x and y descents
- Kussmaul sign (paradoxical rise in JVP with inspiration)
- Pericardial knock — high-pitched early diastolic sound best heard at the apex and lower left sternal border
- Friedreich sign — rapid y descent in the JVP waveform
- Hepatojugular reflux
- Pleural effusions (often bilateral, right > left)
- Atrial fibrillation in 20–30% (due to chronic atrial dilatation)
Imaging
Echocardiography (First-Line)
Transthoracic echocardiography (TTE) is the initial imaging modality and should be requested in all patients with suspected CP. M-mode, two-dimensional, spectral Doppler, and tissue Doppler assessments are all required.
- Septal bounce — abrupt posterior motion of the interventricular septum in early diastole, reflecting rapid ventricular filling abruptly halted by the rigid pericardium. This is the most specific 2D finding for CP.
- Ventricular septal shudder (irregular oscillation of the septum with respiration)
- Abrupt posterior wall motion flattening in diastole
- Dilated IVC (>21 mm) with reduced inspiratory collapse (<50%) — indicates elevated RA pressure
- Pericardial thickening may be visible, particularly in the AV groove
- Preserved or hyperdynamic LV systolic function (EF normal or increased)
- Respiratory variation in mitral inflow velocity ≥25% — peak E velocity decreases by ≥25% during inspiration compared to expiration. (In RCM, variation is <10%.)
- Respiratory variation in tricuspid inflow velocity ≥40% (increases with inspiration)
- Hepatic vein Doppler: prominent diastolic flow reversal during expiration (pathognomonic)
- Tissue Doppler e′ velocity ≥8 cm/s at the lateral mitral annulus (preserved myocardial relaxation)
- Annulus reversus — medial e′ > lateral e′ (normally lateral > medial; reversal is highly suggestive of CP)
- E/e′ ratio typically <15 (unlike RCM where it is elevated)
Cardiac Magnetic Resonance (CMR)
CMR is the investigation of choice for confirming the diagnosis, assessing pericardial inflammation, and guiding treatment decisions (medical vs surgical). It should be performed in all patients with suspected CP unless contraindicated.
- Pericardial thickness — measured on dark-blood spin-echo sequences; >4 mm is abnormal (normal ≤2 mm). CP typically 4–20 mm.
- Pericardial adhesions (cine SSFP: tethering of myocardium to pericardium)
- Dilated IVC and hepatic veins
- Bow-shaped ventricular septum on cine imaging
- T2-weighted imaging (oedema) — high signal within pericardium indicates active inflammation; favours response to anti-inflammatory therapy.
- Late gadolinium enhancement (LGE) of the pericardium indicates gadolinium accumulation in inflamed/fibrotic tissue. Pericardial LGE is associated with transient constriction and a higher likelihood of response to medical therapy.
- Absence of pericardial LGE + calcification on CT = established fibrosis → unlikely to respond to anti-inflammatory treatment → pericardiectomy.
- CMR feature tracking and strain analysis may identify coexistent myocardial disease (mixed constrictive-restrictive physiology).
Cardiac CT
ECG-gated cardiac CT provides excellent spatial resolution for pericardial assessment and is particularly valuable when CMR is contraindicated (pacemaker, ICD) or when pericardial calcification requires precise delineation for surgical planning.
- Pericardial thickness measurement (comparable accuracy to CMR)
- Pericardial calcification — CT is the gold-standard modality for detecting and mapping calcification, which is a predictor of surgical difficulty and incomplete resection
- Non-contrast CT calcium scoring of the pericardium can quantify calcification burden
- CT coronary angiography may be performed concurrently to exclude epicardial coronary disease prior to surgery
Cardiac Catheterisation
Right and left heart catheterisation remains the gold standard for haemodynamic confirmation of CP and is indicated when non-invasive assessment is equivocal or when mixed constrictive-restrictive physiology is suspected.
- Simultaneous RV and LV pressure recording to demonstrate equalised diastolic pressures
- Respiratory variation protocol: the simultaneous LV-RV systolic pressure relationship demonstrates ventricular interdependence (discordant changes with respiration)
- Volume challenge (rapid saline infusion) may unmask subclinical constriction
- Endomyocardial biopsy may be performed during the same procedure to exclude restrictive cardiomyopathy (amyloid, eosinophilic infiltrate)
Aetiology
Identifying the aetiology of constrictive pericarditis is essential because it determines prognosis, the likelihood of transient versus permanent constriction, and the role of anti-inflammatory medical therapy. Up to 30–50% of CP cases in Western populations remain idiopathic after thorough evaluation.
| Aetiology | Approximate Frequency (Australia) | Key Features | Transient Constriction Likely? |
|---|---|---|---|
| Idiopathic / viral | 30–50% | History of preceding viral illness or subclinical pericarditis; may have pericardial LGE on CMR | Yes (in early/inflammatory phase) |
| Post-cardiac surgery | 20–30% | Follows CABG, valve surgery, or pericardiotomy; onset weeks to months post-op | Yes (early presentation) |
| Post-radiotherapy | 10–15% | Latency 10–20 years after mantle-field or left breast radiotherapy; often concurrent radiation cardiomyopathy or coronary disease | Less likely (fibrotic) |
| Tuberculosis | 5–10% | Leading cause globally; higher in ATSI communities, migrants from endemic countries; calcification common; requires anti-TB therapy + surgery | No (chronic fibrotic) |
| Autoimmune / connective tissue disease | 5–8% | SLE, rheumatoid arthritis, systemic sclerosis, sarcoidosis; respond to immunosuppression | Yes (if active inflammation) |
| Uraemia / dialysis | 2–5% | Inadequate dialysis; may improve with intensified dialysis | Yes |
| Post-infectious (bacterial) | 2–5% | Following purulent pericarditis; Staphylococcus aureus, Streptococcus pneumoniae, H. influenzae (paediatric) | Variable |
| Neoplastic (pericardial carcinomatosis) | 1–3% | Lung cancer, breast cancer, melanoma, lymphoma; poor prognosis | No |
Post-Cardiac Surgery CP
Post-cardiac surgery constriction is the second most common cause in Australian practice. The pericardium is often left open after cardiac surgery (posterior pericardiotomy), and the resulting inflammatory adhesions and fibrosis between the epicardium and mediastinal structures can produce a constrictive physiology. Post-pericardiotomy syndrome (PPS), occurring in 10–40% of cardiac surgery patients, is a risk factor for subsequent CP. Early identification of PPS with anti-inflammatory treatment (NSAIDs + colchicine) may prevent progression to chronic constriction.
Radiation-Induced CP
Radiation-induced CP has a latency of 10–20 years and frequently coexists with radiation cardiomyopathy, coronary artery disease, and valvular heart disease. The pericardium is typically heavily calcified and densely adherent to the myocardium, making pericardiectomy technically demanding with higher operative risk. Patients with radiation-induced CP have worse surgical outcomes compared to idiopathic CP, with perioperative mortality of 10–20% in experienced centres.
Tuberculous CP
Tuberculous CP should be considered in patients from endemic regions, Aboriginal and Torres Strait Islander Australians (particularly in the Northern Territory and Far North Queensland), immunocompromised patients (HIV, biologic therapy), and those with a history of TB exposure. Diagnosis may require pericardial fluid analysis, adenosine deaminase (ADA) level (>40 U/L highly suggestive), GeneXpert MTB/RIF, and pericardial biopsy. Anti-TB therapy (RIPE regimen per current Australian TB guidelines) is mandatory before considering surgery.
Medical vs Surgical Management
Transient Constriction & Anti-Inflammatory Trial
A subset of patients with subacute or early CP (particularly idiopathic, post-surgical, and autoimmune aetiologies) will have a reversible inflammatory component — so-called transient constriction. This is characterised by pericardial oedema/inflammation on CMR (T2 hyperintensity and LGE) and may resolve with medical therapy alone, avoiding the need for surgery.
Anti-Inflammatory Regimen
Following the anti-inflammatory trial, clinical reassessment at 2–3 months should include repeat TTE and ideally repeat CMR to assess for resolution of pericardial oedema and improvement in constrictive physiology. Persistent symptoms and imaging findings after an adequate anti-inflammatory trial indicate established (irreversible) CP and the need for pericardiectomy.
Pericardiectomy — Indications, Technique & Outcomes
Complete (total) pericardiectomy is the definitive treatment for chronic, established constrictive pericarditis. The goal is radical excision of the pericardium from phrenic nerve to phrenic nerve, including all calcified and fibrotic tissue.
Indications for Pericardiectomy
- Established CP with NYHA Class II–IV symptoms refractory to medical therapy
- Persistent constrictive physiology after a 2–3 month anti-inflammatory trial (confirmed by imaging and haemodynamics)
- Heavily calcified pericardium without CMR evidence of active inflammation (anti-inflammatory therapy will not help)
- Tuberculous CP after completion of anti-TB therapy with persistent constriction
- Progressive symptoms despite optimal diuretic and heart-failure management
Contraindications & Relative Contraindications
- Severe right ventricular systolic dysfunction (RV fractional area change <20%) — poor myocardial contractility will not recover after pericardial stripping
- Extensive myocardial fibrosis (radiation cardiomyopathy with concurrent myocardial disease)
- Severe pulmonary hypertension (RVSP >60 mmHg) unrelated to CP
- Advanced malignancy with short life expectancy
- Frailty and prohibitive surgical risk
Surgical Approach
Surgical Outcomes
| Outcome | Idiopathic / Viral CP | Post-Surgical CP | Radiation CP | TB CP |
|---|---|---|---|---|
| Perioperative mortality | 3–5% | 5–10% | 10–20% | 5–15% |
| Symptom improvement | 85–95% | 70–85% | 50–70% | 75–90% |
| 5-year survival | 85–95% | 70–85% | 40–60% | 70–85% |
| Persistent symptoms | 5–10% | 15–25% | 25–40% | 10–20% |
Medical Management of Symptoms (Bridge & Non-Surgical Candidates)
Diuretics are the mainstay of symptomatic management in CP and are used both as a bridge to surgery and for patients who are not surgical candidates. Loop diuretics (furosemide) and mineralocorticoid receptor antagonists (spironolactone) should be used judiciously to relieve congestion without causing underfilling of the constrained ventricles, which can precipitate low cardiac output.
Treatment Decision Algorithm
Monitoring
During Medical Therapy
- Clinical review every 2–4 weeks during anti-inflammatory trial — weight, blood pressure, JVP assessment, peripheral oedema grading, exercise tolerance
- Inflammatory markers (CRP, ESR) at baseline, 4 weeks, and 12 weeks to guide tapering of anti-inflammatory therapy
- Renal function (eGFR, electrolytes) at 1–2 weekly intervals during diuretic titration
- Repeat TTE at 3 months to assess for resolution of constrictive physiology
- Repeat CMR at 3 months (if available) to assess pericardial oedema, LGE, and thickness — guides decision to continue medical therapy or proceed to surgery
Post-Pericardiectomy
- ICU monitoring for 24–48 hours post-operatively with invasive haemodynamic monitoring (arterial line, CVC)
- Watch for low cardiac output syndrome — may occur in 10–20% of patients due to chronic myocardial atrophy beneath the pericardium
- Chest drain output monitoring; bleeding risk is elevated due to extensive dissection
- TTE prior to discharge and at 1, 3, 6, and 12 months post-operatively
- Gradual uptitration of exercise based on symptoms; formal cardiac rehabilitation recommended
- Long-term follow-up for atrial fibrillation (20–30% develop new-onset AF), recurrence of constriction (rare with complete pericardiectomy, 2–5%), and ongoing aetiology-specific management
Special Populations
Pregnancy
Paediatrics
Elderly
Renal Impairment
Hepatic Impairment
Immunocompromised
Aboriginal and Torres Strait Islander Health Considerations
Constrictive pericarditis in Aboriginal and Torres Strait Islander Australians is disproportionately associated with rheumatic heart disease (RHD) and tuberculosis, both of which have significantly higher prevalence in Indigenous compared to non-Indigenous Australians. The AIHW reports that the rate of acute rheumatic fever (ARF) in Aboriginal and Torres Strait Islander Australians is 56 times higher than in non-Indigenous Australians, with the highest burden in the Northern Territory, Western Australia, and Far North Queensland.
RHD-related pericardial disease, while primarily valvular, may involve pericardial inflammation and subsequent constriction. Tuberculous pericarditis remains a significant concern, with the Northern Territory recording TB notification rates 6–10 times the national average. Culturally safe, community-centred approaches to diagnosis and long-term management are essential.
Quick Reference — Diagnosis & Treatment
📚 References
- 1. Adler Y, Charron P, Imazio M, et al. 2015 ESC Guidelines for the diagnosis and management of pericardial diseases. Eur Heart J. 2015;36(42):2921–2964.
- 2. Geske JB, Anavekar NS, Nishimura RA, Oh JK, Gersh BJ. Differentiation of constriction and restriction: complex cardiovascular hemodynamics. J Am Coll Cardiol. 2016;68(22):2329–2347.
- 3. Welch TD, Ling LH, Espinosa RE, et al. Echocardiographic diagnosis of constrictive pericarditis: Mayo Clinic criteria. Circ Cardiovasc Imaging. 2014;7(3):526–534.
- 4. Cremer PC, Kumar A, Kontzias A, et al. Complicated pericarditis: understanding risk factors and pathophysiology to inform imaging and treatment. J Am Coll Cardiol. 2016;68(21):2311–2328.
- 5. Klein AL, Abbara S, Agler DA, et al. American Society of Echocardiography clinical recommendations for multimodality cardiovascular imaging of patients with pericardial disease. J Am Soc Echocardiogr. 2013;26(9):965–1012.
- 6. Imazio M, Brucato A, Maestroni S, et al. Risk of constrictive pericarditis after acute pericarditis. Circulation. 2011;124(11):1270–1275.
- 7. Bertog SC, Thambidorai SK, Parakh K, et al. Constrictive pericarditis: etiology and cause-specific survival after pericardiectomy. J Am Coll Cardiol. 2004;43(8):1445–1452.
- 8. Chowdhury UK, Subramaniam GK, Kumar AS, et al. Pericardiectomy for constrictive pericarditis: a clinical, echocardiographic, and hemodynamic evaluation of two surgical techniques. Ann Thorac Surg. 2006;81(2):522–529.
- 9. Australian Institute of Health and Welfare. Acute rheumatic fever and rheumatic heart disease in Australia. AIHW; 2023.
- 10. RHDAustralia (ARF/RHD writing group). National guideline for the prevention, diagnosis and management of acute rheumatic fever and rheumatic heart disease. 3rd ed. Darwin: Menzies School of Health Research; 2020.
- 11. World Health Organization. WHO consolidated guidelines on tuberculosis: module 4 — treatment. Geneva: WHO; 2022.
- 12. Syed FF, Mayosi BM. A modern approach to tuberculous pericarditis. Prog Cardiovasc Dis. 2007;50(3):218–236.
- 13. Veress G, Feng D, Oh JK. Significant respiratory variation of mitral and tricuspid Doppler velocities in constrictive pericarditis. Circ Cardiovasc Imaging. 2020;13(5):e010278.
- 14. Cosyns B, Plein S, Nihoyanopoulos P, et al. European Association of Cardiovascular Imaging (EACVI) position paper: multimodality imaging in pericardial disease. Eur Heart J Cardiovasc Imaging. 2015;16(1):12–31.
- 15. Australian Bureau of Statistics. Estimates of Aboriginal and Torres Strait Islander Australians. ABS; 2023.