📋 Key Information Summary
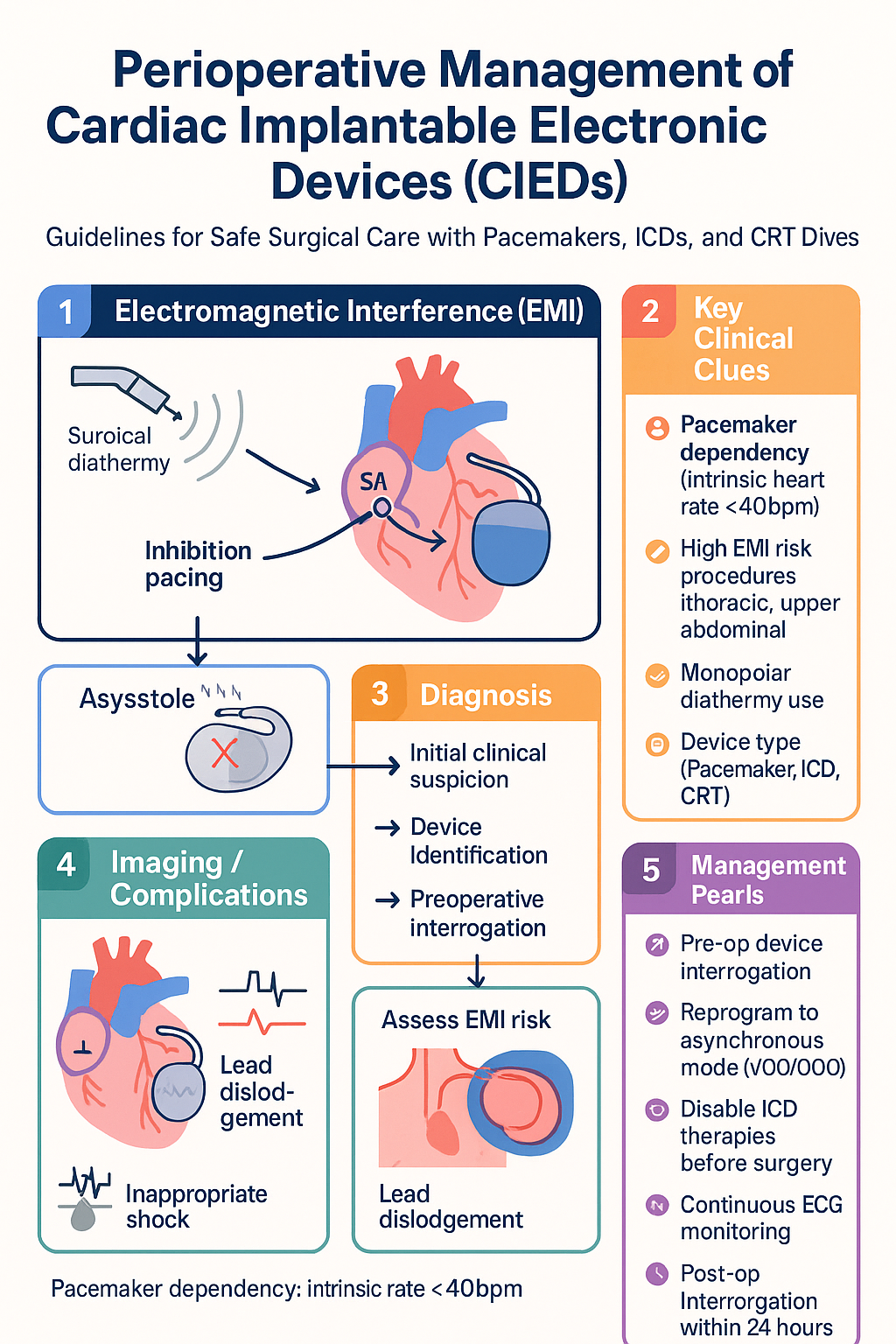
- All patients with cardiac implantable electronic devices (CIEDs) require preoperative device identification — confirm manufacturer, model, type (pacemaker, ICD, CRT), and dependency status.
- The NBG (North American Society of Pacing and Electrophysiology / British Pacing and Electrophysiology Group) five-letter code classifies pacing mode — chambers paced, sensed, response, rate modulation, and multisite pacing.
- Patients who are pacemaker-dependent (no intrinsic rhythm ≥40 bpm at rest) require specific perioperative plans — reprogramming to asynchronous mode (VOO/DOO) or magnet placement before diathermy.
- ICD tachyarrhythmia therapies MUST be disabled before any procedure involving electrocautery; failure to do so risks inappropriate shock or device damage.
- Electromagnetic interference (EMI) from surgical diathermy is the primary perioperative CIED hazard — monopolar diathermy poses higher risk than bipolar.
- Bipolar diathermy is preferred over monopolar when feasible; if monopoly is essential, ensure the dispersive pad is positioned so current does not cross the CIED generator or lead vector.
- CRT and CRT-D patients require both bradycardia and tachycardia function management; coordinate preoperative interrogation with the device clinic.
- Post-operative device interrogation is mandatory after any procedure where EMI risk was present — confirm normal sensing, pacing thresholds, and re-enable tachy therapies if appropriate.
- CIED-dependent patients undergoing high-risk procedures (upper abdominal, thoracic, or any case with anticipated monopolar diathermy near the device) should have continuous ECG monitoring and defibrillation pads placed.
- A surgical CIED management plan should be documented at least 2 weeks before elective surgery — engage the device clinic early.
- Magnet application provides a temporary asynchronous pacing response in most pacemakers but does NOT disable ICD therapies — specialist reprogramming is required for ICDs.
- Post-operative programming to original mode should be completed within 24 hours — asynchronous pacing in a non-dependent patient risks competitive rhythms.
Introduction & Australian Epidemiology
The perioperative management of cardiac implantable electronic devices (CIEDs) — including permanent pacemakers (PPMs), implantable cardioverter-defibrillators (ICDs), and cardiac resynchronisation therapy (CRT/CRT-D) devices — is an increasingly common clinical challenge. As the population ages and device implantation rates rise, anaesthetists, surgeons, and cardiologists must collaborate to ensure safe operative care for patients with these devices.
Perioperative management of pacemakers and ICDs requires careful planning to avoid electromagnetic interference (EMI); device-dependent patients need particular consideration. EMI from surgical diathermy can cause inappropriate inhibition of pacing output, reprogramming to noise-reversion mode, inappropriate ICD shock delivery, or permanent device damage. The risk is highest with monopolar electrocautery applied near the device or its lead system.
In Australia, approximately 25,000–30,000 new CIED implantations are performed annually, with permanent pacemakers accounting for roughly 70% of implants and ICDs/CRT devices making up the remainder. Data from the Australian Institute of Health and Welfare (AIHW) indicate that device implantation rates increase with age, peaking in the 75–84-year cohort. Aboriginal and Torres Strait Islander peoples experience a younger age of cardiovascular disease onset and may require device implantation at earlier ages, though access to device services remains inequitable in remote and regional areas.
This guideline provides evidence-based recommendations for the perioperative management of CIEDs, incorporating Australian practice standards from the Cardiac Society of Australia and New Zealand (CSANZ), the Australian and New Zealand College of Anaesthetists (ANZCA), and relevant international consensus documents.
Pacing Modes & Codes (NBG)
The revised NASPE/BPEG Generic (NBG) Pacemaker Code, last updated in 2002, provides a five-position system for describing pacemaker and ICD function. Understanding this code is essential for perioperative planning, as it determines how the device will interact with surgical electromagnetic fields.
| Position | I — Chamber(s) Paced | II — Chamber(s) Sensed | III — Response to Sensing | IV — Rate Modulation | V — Multisite Pacing |
|---|---|---|---|---|---|
| Letters | O = None A = Atrium V = Ventricle D = Dual (A+V) |
O = None A = Atrium V = Ventricle D = Dual |
O = None T = Triggered I = Inhibited D = Dual (T+I) |
O = None R = Rate modulation |
O = None A = Atrial V = Ventricular D = Dual |
Common Pacing Modes — Perioperative Relevance
| Mode | Code | Description | EMI Risk | Perioperative Action |
|---|---|---|---|---|
| Dual chamber | DDD / DDDR | Standard dual-chamber sensing and pacing with optional rate response | High — EMI sensed as atrial/ventricular activity → inhibition | Reprogram to DOO/VOO if diathermy near device |
| Ventricular demand | VVI / VVIR | Ventricle-only sensing and pacing; inhibited by sensed events | High — EMI → pacing inhibition | Reprogram to VOO for monopolar diathermy |
| Asynchronous dual | DOO | Both chambers paced at fixed rate; no sensing | Minimal — not inhibited by EMI | Preferred for device-dependent patients undergoing surgery |
| Asynchronous ventricular | VOO | Ventricle paced at fixed rate; no sensing | Minimal | Alternative if DOO not available |
| Atrial asynchronous | AOO | Atrium paced at fixed rate; no sensing | Minimal | Rarely used; risk of competitive rhythm |
Rate-Modulated Pacing (RR)
Rate-modulated pacing uses sensors (accelerometer, minute ventilation, or combined) to increase pacing rate with activity. Perioperatively, diaphragmatic stimulation from mechanical ventilation or shivering can be misinterpreted by the minute-ventilation sensor, causing inappropriately rapid pacing. Consider disabling rate modulation for procedures where mechanical ventilation or neuromuscular blockade will be used.
Magnet Response
Application of a ring magnet (≥80 Gauss) over the CIED generator triggers a manufacturer-specific magnet response:
- Most pacemakers: Switch to asynchronous pacing (VOO/DOO/AOO) at a fixed magnet rate (typically 80–100 bpm).
- Medtronic pacemakers: Magnet rate indicates battery status — 85 bpm (ERI), 100 bpm (normal).
- ICDs: Magnet may suspend tachyarrhythmia detection in some devices (e.g., Biotronik, Abbott/St. Jude Medical), but NOT in Medtronic or Boston Scientific ICDs — these still deliver shocks with a magnet applied.
Perioperative Pacemaker Management
Structured perioperative management reduces the risk of device malfunction, inappropriate therapy delivery, and haemodynamic compromise. A systematic approach involving preoperative assessment, intraoperative management, and post-operative device interrogation is essential.
Step 1 — Preoperative Assessment (≥2 Weeks Before Surgery)
Surgical EMI Risk Stratification
Intraoperative Management
- Non-dependent patients: Monitor with continuous ECG. Magnet available at bedside. Reprogram only if significant EMI causes inappropriate inhibition.
- Dependent patients: Reprogram to VOO or DOO before incision. Use bipolar diathermy if possible. If monopolar required, keep diathermy bursts short (<5 s) with ≥10-second intervals.
- Place the dispersive (grounding) pad so the current path does not cross the CIED or lead vector — typically on the ipsilateral thigh for upper body surgery.
- Continuous ECG monitoring throughout; be prepared for pacing inhibition during diathermy bursts in sensing modes.
- All patients: Disable tachyarrhythmia therapies (ATP + shocks) before surgery — this requires specialist reprogramming with a programmer.
- Place external defibrillator pads (anterior–posterior) before draping if any EMI risk exists.
- If patient is pacemaker-dependent, additionally reprogram bradycardia pacing to asynchronous mode.
- Have a manual external defibrillator and crash cart immediately available.
- Re-enable ICD therapies as soon as feasible post-operatively (ideally within 24 hours).
Diathermy Best Practice
| Parameter | Recommendation |
|---|---|
| Diathermy type | Prefer bipolar over monopolar; if monopolar required, use coagulation mode where possible (lower EMI than cutting mode) |
| Dispersive pad placement | Position so current path does not cross CIED generator or lead vector; ipsilateral thigh or ipsilateral buttock preferred |
| Diathermy bursts | Short bursts (<5 seconds); intervals ≥10 seconds between bursts |
| Distance from CIED | Maintain ≥15 cm between diathermy active electrode and CIED generator |
| Power setting | Use the lowest effective power setting |
Post-Operative Management
- Device interrogation is mandatory within 24 hours (ideally same day) after any moderate- or high-risk procedure.
- Confirm: pacing thresholds within acceptable range, sensing appropriate, lead impedance stable, battery status unchanged, and no inappropriate mode changes.
- Restore original programming — re-enable rate modulation, reprogram from asynchronous mode back to DDD/VVI as appropriate.
- For ICDs: re-enable tachyarrhythmia therapies (ATP + shocks) immediately after confirmed haemodynamic stability.
- Monitor for delayed complications: lead dislodgement (presenting as loss of capture or inappropriate sensing), pocket haematoma, or infection at the surgical site.
- Document all programming changes in the device clinic records and patient notes.
ICD & CRT Perioperative Considerations
Implantable cardioverter-defibrillators (ICDs) and cardiac resynchronisation therapy devices (CRT-P, CRT-D) present additional perioperative complexity beyond standard pacemakers due to their tachyarrhythmia detection and high-voltage therapy delivery capabilities.
ICD-Specific Perioperative Risks
- Mandatory pre-operative reprogramming: All ICD tachyarrhythmia therapies (VT zone ATP, VF zone ATP, and high-voltage shocks) must be disabled by a qualified cardiac physiologist or electrophysiologist using the device-specific programmer.
- Brady pacing: If the patient is bradycardia-dependent, reprogram the pacing component to an asynchronous mode (VOO/DOO) as for standard pacemakers.
- External defibrillation: Place external defibrillation pads (adhesive, anterior–posterior configuration) before surgical draping. Confirm the external defibrillator is charged and ready. Ensure staff are aware the device will NOT deliver therapy during the procedure.
- Magnet limitations: Magnet application does NOT reliably disable ICD therapies in Medtronic or Boston Scientific devices. Do not rely on magnet-only management for any ICD. Always use programmer-based reprogramming.
CRT/CRT-D Perioperative Management
Cardiac resynchronisation therapy devices provide both bradycardia pacing and biventricular (BiV) synchronisation. CRT-D devices additionally include ICD functions.
| Device Type | Functions to Manage | Perioperative Action |
|---|---|---|
| CRT-P | Bradycardia pacing + biventricular synchronisation | Reprogram brady pacing to asynchronous mode if dependent; consider whether loss of BiV pacing during surgery is tolerable (usually yes for short procedures) |
| CRT-D | Bradycardia pacing + BiV + ICD therapies | Disable ICD therapies (mandatory); reprogram brady pacing to asynchronous mode if dependent; place external defibrillator pads |
Emergency External Defibrillation for CIED Patients
If external defibrillation is required during surgery in a patient with a CIED:
- Use anterior–posterior pad placement (preferred) or anterior–lateral, ensuring pads are ≥8 cm from the CIED generator.
- Deliver standard biphasic shock energy (150–200 J for initial shock).
- After successful defibrillation, perform urgent device interrogation — high-voltage shocks can damage CIED circuitry or alter programming.
- If the CIED is on the ipsilateral side to the anterior pad, consider temporarily switching to lateral pad position on the contralateral side.
Electromagnetic Interference & Reprogramming
Electromagnetic interference (EMI) is the primary perioperative hazard for CIED patients. Understanding the sources, mechanisms, and management of EMI is critical for safe perioperative care.
Sources of EMI in the Operating Theatre
| EMI Source | Risk Level | Mechanism | Management |
|---|---|---|---|
| Monopolar electrocautery (diathermy) | High | Broad-spectrum RF energy; may be sensed as intrinsic cardiac activity → pacing inhibition or inappropriate ICD shock | Reprogram to asynchronous; disable ICD; bipolar preferred; pad placement |
| Bipolar electrocautery | Low | Confined current field between forceps tips; minimal EMI at distance | Usually safe; monitor ECG; keep ≥15 cm from CIED |
| Transcutaneous electrical nerve stimulation (TENS) | Moderate | Electrical signals may be sensed by device | Avoid ipsilateral placement; monitor if used |
| Electroconvulsive therapy (ECT) | Moderate | Electrical stimulation; risk of competitive pacing | Reprogram to asynchronous if dependent; continuous ECG; device interrogation post-procedure |
| Magnetic resonance imaging (MRI) | Very High | Static magnetic field + RF pulses + gradient fields → force on device, heating of leads, reprogramming | Only MRI-conditional devices with specific protocols; not typically intraoperative |
| Lithotripsy | Moderate | Shock waves may cause device malfunction or inappropriate sensing | Disable rate-modulated pacing; consider reprogramming to asynchronous if dependent; synchronise shock delivery to R-wave where possible |
| Radiofrequency ablation | High | Direct RF energy delivery; may interfere with device function | Reprogram pacemaker to asynchronous; disable ICD therapies; continuous ECG |
Reprogramming Protocols
Manufacturer-Specific Magnet Responses (ICDs)
| Manufacturer | Magnet Effect on ICD Therapies | Safe to Rely on Magnet Alone? |
|---|---|---|
| Medtronic | Therapies NOT disabled — shocks still delivered | NO |
| Boston Scientific | Therapies NOT disabled — shocks still delivered | NO |
| Abbott (St. Jude Medical) | Therapies may be suspended while magnet is in place | NO — programmer still recommended |
| Biotronik | Therapies suspended while magnet is applied | NO — programmer still recommended |
| Microport (Sorin/LivaNova) | Variable — consult specific model documentation | NO |
Special Populations
Aboriginal and Torres Strait Islander Health Considerations
Aboriginal and Torres Strait Islander peoples experience a significantly higher burden of cardiovascular disease, including rheumatic heart disease (RHD) and ischaemic cardiomyopathy, both of which are indications for CIED implantation. The incidence of acute rheumatic fever (ARF) in Indigenous Australians in northern and central Australia remains among the highest globally, and RHD-related conduction disease is a leading cause of pacemaker implantation in younger Indigenous patients.
Monitoring
Intraoperative Monitoring
- Continuous ECG monitoring (5-lead preferred) — visualise pacing spikes and intrinsic complexes. Use a rhythm display with pacing marker channel if available.
- Pulse oximetry with plethysmograph — provides real-time confirmation of perfusion; loss of plethysmograph waveform during diathermy burst may indicate pacing inhibition.
- Invasive arterial monitoring — consider for pacemaker-dependent patients or those with haemodynamic instability; provides beat-to-beat blood pressure confirmation.
- End-tidal CO₂ — confirms cardiac output indirectly; rapid fall may indicate pacing failure.
- Palpation of pulse — manual pulse check after each diathermy burst if asynchronous mode not used.
Post-Operative Monitoring
- Continuous telemetry for ≥4 hours post-procedure in moderate- and high-risk cases.
- Device interrogation within 24 hours — confirm all parameters restored.
- Inspect CIED pocket for haematoma, swelling, or erythema if device was manipulated.
- Document pacing percentage, sensing thresholds, lead impedances, and battery status.
- For ICD patients: re-enable tachyarrhythmia therapies immediately after confirmed haemodynamic stability and adequate device parameters.
- Arrange follow-up device clinic appointment within 1–3 months as per standard schedule.
📚 References
- 1. Crossley GH, Poole JE, Rozner MA, et al. The Heart Rhythm Society (HRS)/American Society of Anesthesiologists (ASA) Expert Consensus Statement on the Perioperative Management of Patients with Implantable Defibrillators, Pacemakers and Arrhythmia Monitors. Heart Rhythm. 2011;8(7):1114-1154.
- 2. Cardiac Society of Australia and New Zealand (CSANZ). Guidelines for the Perioperative Management of Patients with Cardiac Implantable Electronic Devices. Heart Lung Circ. 2018;27(9):1081-1098.
- 3. Bernstein AD, Daubert JC, Fletcher RD, et al. The revised NASPE/BPEG generic code for antibradycardia, adaptive-rate, and multisite pacing. Pacing Clin Electrophysiol. 2002;25(2):260-264.
- 4. Australian Institute of Health and Welfare (AIHW). Cardiovascular disease: Australian facts 2023. AIHW, Canberra. 2023.
- 5. RHDAustralia (RHD Australia, ARF/RHD writing group). The 2020 Australian guideline for prevention, diagnosis and management of acute rheumatic fever and rheumatic heart disease. 3rd edition. Menzies School of Health Research, Darwin. 2020.
- 6. Australian and New Zealand College of Anaesthetists (ANZCA). PS64: Recommendations for the Perioperative Management of Patients with Cardiac Implantable Electronic Devices. ANZCA, Melbourne. 2019.
- 7. Stone KR, McPherson CA. Assessment and management of patients with pacemakers and implantable cardioverter defibrillators. Crit Care Med. 2018;46(9):1488-1497.
- 8. Buchanan GL, Chieffo A, Mehilli J, et al. The occupational effects of interventional cardiology: results from the WIN for Safety survey. EuroIntervention. 2012;8(6):658-663.
- 9. Schulman PM, Rozner MA, Sera V, Stecker EC. Patients with pacemaker or implantable cardioverter-defibrillator. Med Clin North Am. 2013;97(6):1051-1074.
- 10. National Aboriginal Community Controlled Health Organisation (NACCHO). Cardiovascular health in Aboriginal and Torres Strait Islander peoples: position statement. NACCHO, Canberra. 2022.
- 11. Boriani G, Fauchier L, Aguinaga L, et al. European Heart Rhythm Association (EHRA) consensus document on management of arrhythmias and cardiac electronic devices in the critically ill and post-surgery patient. Europace. 2019;21(1):7-16.
- 12. Australian Commission on Safety and Quality in Health Care (ACSQHC). National Safety and Quality Health Service Standards. 2nd edition. ACSQHC, Sydney. 2017.