📋 Key Information Summary
- Antibiotic prophylaxis (AP) for infective endocarditis (IE) is restricted to high-risk cardiac conditions undergoing high-risk procedures — universal AP is not recommended.
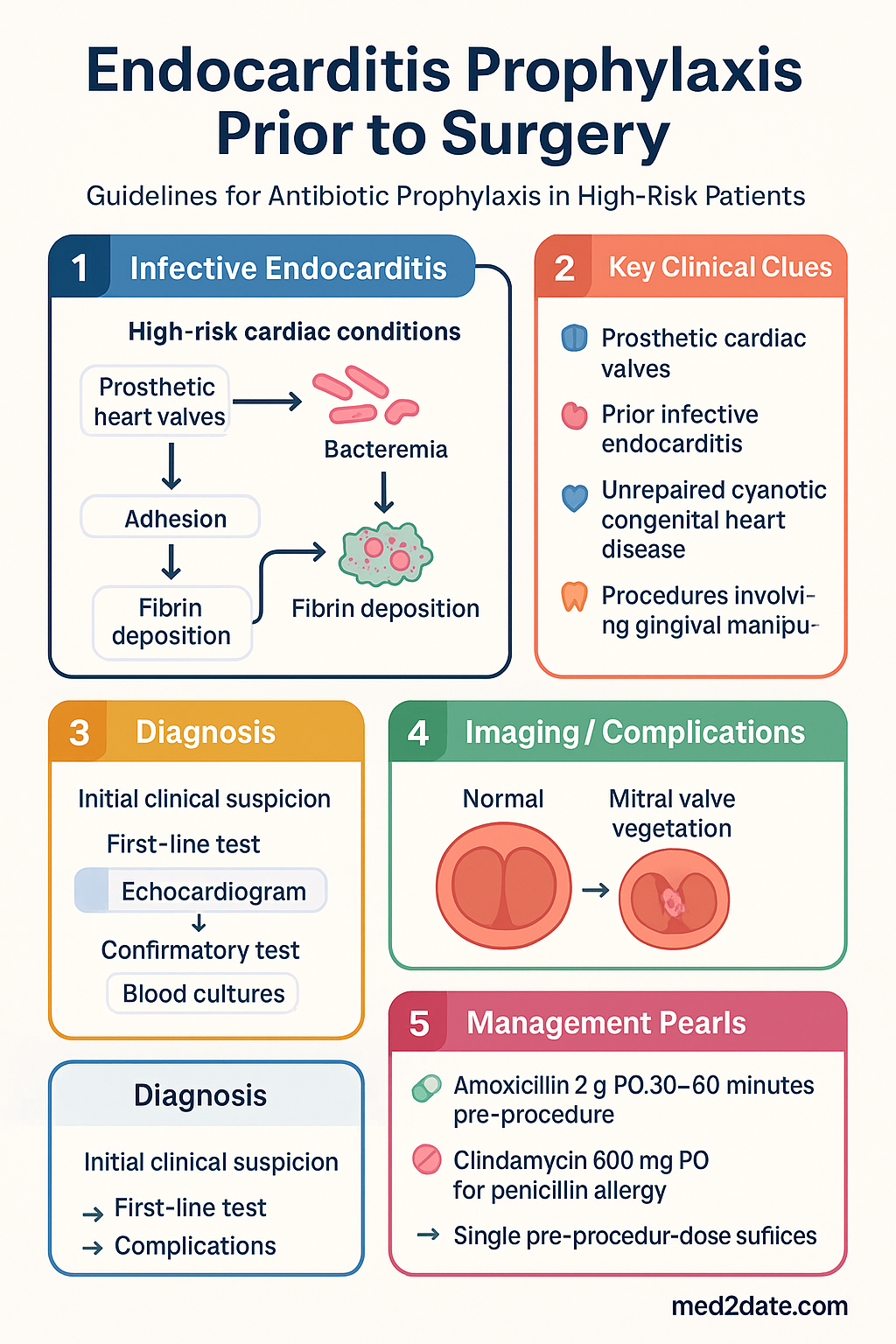
- High-risk conditions include prosthetic cardiac valves, prior infective endocarditis, and unrepaired cyanotic congenital heart disease (including palliative shunts/conduits).
- Procedures requiring prophylaxis are predominantly dental procedures involving gingival or periapical manipulation of teeth, or perforation of oral mucosa.
- Respiratory tract procedures involving incision or biopsy of mucosa (e.g., tonsillectomy, adenoidectomy) also warrant prophylaxis in high-risk patients.
- Genitourinary and gastrointestinal procedures do not routinely require IE prophylaxis — bacteraemia during these procedures has not been causally linked to IE in epidemiological studies.
- First-line regimen: Amoxicillin 2 g PO (adults) or 50 mg/kg (paediatric) 30–60 minutes pre-procedure.
- Penicillin allergy / alternative: Clindamycin 600 mg PO (adults) or 20 mg/kg (paediatric) 30–60 minutes pre-procedure.
- For patients unable to take oral medication, IV amoxicillin 2 g or IV cefazolin 1 g (if penicillin allergy non-anaphylactic) pre-procedure.
- NICE (UK) 2008 guidelines are the most restrictive, recommending no antibiotic prophylaxis at all — even for high-risk patients.
- ESC 2015 guidelines and Heart Foundation of Australia support targeted AP for high-risk groups, while emphasising oral hygiene as the primary preventive strategy.
- Two doses of post-procedure antibiotics are not recommended by current ESC or Australian guidelines — single pre-procedure dose suffices.
- Aboriginal and Torres Strait Islander peoples experience higher rates of rheumatic heart disease and should be assessed individually for AP needs.
- All patients at risk of IE should receive regular dental care, patient education about symptoms of IE, and counselling on rigorous oral hygiene.
- Australian prescribing aligns with Heart Foundation / Cardiac Society of Australia and New Zealand (CSANZ) endorsement of ESC-class principles with local adaptation.
Introduction & Australian Epidemiology
Infective endocarditis (IE) remains a life-threatening infection of the endocardial surface, typically affecting native or prosthetic heart valves, with an in-hospital mortality of 15–30% despite advances in antimicrobial therapy and surgical intervention. The paradigm for antibiotic prophylaxis (AP) has shifted markedly over the past two decades: whereas broad prophylaxis was once recommended for a wide range of cardiac and procedural combinations, current international consensus restricts AP to high-risk cardiac conditions undergoing high-risk procedures, reflecting the low attributable risk of bacteraemia from most interventions.
In Australia, IE incidence is estimated at 4–7 per 100,000 population per year, with important demographic variation. Aboriginal and Torres Strait Islander Australians experience disproportionately higher rates — approximately 3–5 times the non-Indigenous rate — driven largely by the burden of rheumatic heart disease (RHD) in remote and regional communities. The Australian Institute of Health and Welfare (AIHW) reports that RHD-associated IE remains a leading cause of cardiac morbidity in Indigenous Australians under 50 years of age.
The epidemiological shift from Streptococcus viridans-dominant IE to Staphylococcus aureus-dominant IE, observed internationally and confirmed in Australian registries, has influenced prophylaxis thinking. Health care–associated IE (including intravascular device–related and haemodialysis-associated) now accounts for a substantial proportion of cases, and these are not preventable by dental AP. Nonetheless, dental bacteraemia remains a plausible trigger for IE in susceptible individuals, and targeted AP retains a role in selected patients.
Australian clinical practice is guided by endorsement of European Society of Cardiology (ESC) principles by the Heart Foundation of Australia and the Cardiac Society of Australia and New Zealand (CSANZ), while acknowledging the contrasting NICE position. This guideline synthesises the current evidence, reconciles guideline differences, and provides practical prescribing advice for Australian clinicians.
High-Risk Cardiac Conditions Requiring Prophylaxis
Antibiotic prophylaxis is recommended only for patients with cardiac conditions that confer the highest risk of adverse outcomes from IE. These conditions carry a disproportionate burden of morbidity and mortality, and prophylaxis offers a favourable risk–benefit ratio in this subgroup.
| Risk Category | Conditions | Rationale |
|---|---|---|
| Highest risk |
Prosthetic heart valve (mechanical or bioprosthetic) Prosthetic material used for valve repair (annuloplasty ring, chords) Prior infective endocarditis (any episode, any organism) |
Highest mortality and recurrence risk; prosthetic material is a nidus for biofilm; prior IE implies permissive valve pathology |
| High risk |
Unrepaired cyanotic congenital heart disease (CHD), including palliative shunts and conduits Completely repaired CHD with prosthetic material or device during first 6 months post-repair Residual defects at or adjacent to prosthetic patch or device |
Turbulent flow and residual shunts predispose to endocardial infection; prosthetic device surfaces are vulnerable during endothelialisation |
| Additional consideration | Cardiac transplant recipients who develop valvulopathy | Immunosuppression plus valvular dysfunction increases susceptibility |
Rheumatic heart disease (RHD) — special consideration in Australia: While RHD without prosthetic material is no longer universally classified as high-risk, Australian clinicians — particularly those practising in Aboriginal and Torres Strait Islander communities — should exercise clinical judgement. Patients with RHD and significant valvular regurgitation, particularly those awaiting surgery or with haemodynamically significant lesions, may benefit from individualised risk assessment for AP. RHDAustralia guidelines emphasise maintaining a low threshold for AP in this population, given the high background IE incidence.
Procedures Requiring Prophylaxis
Prophylaxis is directed at procedures known to cause significant bacteraemia with organisms capable of colonising damaged endocardium. The evidence base derives from observational studies of bacteraemia frequency and timing, as no randomised controlled trials of AP have been conducted (nor are they likely to be feasible given the low incidence of IE).
Antibiotic Regimens
Prophylaxis is a single dose of antibiotic administered 30–60 minutes prior to the procedure. No additional post-procedure doses are recommended by current ESC or Australian guidelines.
Alternative Regimens — Patients Unable to Take Oral Medication
| Scenario | Drug | Adult Dose | Paediatric Dose | Route |
|---|---|---|---|---|
| NPO / sedated patient | Amoxicillin | 2 g IV | 50 mg/kg IV (max 2 g) | IV over 30 min |
| Penicillin allergy (non-anaphylactic) | Cefazolin | 1 g IV | 25 mg/kg IV (max 1 g) | IV or IM |
| Penicillin allergy (anaphylactic) — IV | Clindamycin | 600 mg IV | 20 mg/kg IV (max 600 mg) | IV over 20 min |
| Vancomycin allergy / intolerant | Teicoplanin | 400 mg IV | 10 mg/kg IV (max 400 mg) | IV over 30 min |
NICE vs ESC Guidelines — Key Differences
The divergent positions of the European Society of Cardiology (ESC 2015) and the UK National Institute for Health and Care Excellence (NICE 2008, updated 2016) represent the most significant international disagreement in IE prophylaxis. Australian practice aligns more closely with the ESC approach, as endorsed by the Heart Foundation of Australia and CSANZ.
| Domain | ESC 2015 (European) | NICE 2008/2016 (UK) | Australian Position |
|---|---|---|---|
| Overall stance | Targeted AP for highest-risk patients | No AP for any patient, any procedure | ESC-aligned: targeted AP for high-risk |
| Basis for no AP (NICE) | Observational evidence supports benefit in high-risk; no RCT evidence exists either way | Absence of RCT evidence of AP efficacy; procedure-related bacteraemia is common and often transient | Acknowledges lack of RCT but accepts precautionary principle |
| High-risk conditions | Prosthetic valve, prior IE, cyanotic CHD | N/A — no AP given | Same as ESC |
| Dental procedures | AP for gingival/periapical/mucosal procedures in high-risk | No AP even for extractions in prosthetic valve patients | AP recommended per ESC |
| GI / GU procedures | AP not recommended | AP not recommended | AP not recommended |
| Oral hygiene emphasis | Strong emphasis alongside AP | Primary strategy (replacing AP) | Both — oral hygiene + targeted AP |
| Post-procedure doses | Not recommended (single dose) | N/A | Single dose only |
| Year of last update | 2015 | 2016 (review confirmed position) | Ongoing; aligned with ESC |
Practical Implications for Australian Clinicians
- Document the cardiac condition, the planned procedure, and the rationale for (or against) AP in the clinical record.
- For patients who have been advised by UK-trained clinicians that AP is unnecessary, re-discuss with the patient and their cardiologist, applying the ESC-aligned Australian position.
- For patients at moderate risk (e.g., bicuspid aortic valve with regurgitation, prior RHD) not classified as "high risk" by ESC, individualise the decision and document shared decision-making.
- Maintain a register of patients requiring AP (e.g., in the practice management software) and alert them before dental appointments.
Aboriginal and Torres Strait Islander Health Considerations
Monitoring & Follow-Up
While IE prophylaxis is a single-dose intervention, ongoing monitoring and health-system supports are essential to prevent missed prophylaxis and to detect IE early if it occurs.
Special Populations
📚 References
- 1. Habib G, Lancellotti P, Antunes MJ, et al. 2015 ESC guidelines for the management of infective endocarditis. European Heart Journal. 2015;36(44):3075–3128. doi:10.1093/eurheartj/ehv319
- 2. National Institute for Health and Care Excellence. Prophylaxis against infective endocarditis: antimicrobial prophylaxis against infective endocarditis in adults and children undergoing interventional procedures. NICE guideline CG64. 2008 (updated 2016).
- 3. National Heart Foundation of Australia. Position statement: antibiotic prophylaxis for infective endocarditis. Heart Foundation; 2022.
- 4. Heart Foundation, Cardiac Society of Australia and New Zealand. Diagnosis and management of endocarditis: Australian expert commentary on ESC 2015 guidelines. Heart, Lung and Circulation. 2016;25(7):643–648.
- 5. Australian Institute of Health and Welfare. Rheumatic heart disease and acute rheumatic fever in Australia. AIHW Cat. No. CVD 86. Canberra: AIHW; 2023.
- 6. RHDAustralia (ARF/RHD writing group). The 2020 Australian guideline for prevention, diagnosis, and management of acute rheumatic fever and rheumatic heart disease (3rd edition). Menzies School of Health Research; 2020.
- 7. Cahill TJ, Harrison JL, Jewell P, et al. Antibiotic prophylaxis for infective endocarditis: a systematic review and meta-analysis. Heart. 2017;103(12):937–944. doi:10.1136/heartjnl-2015-309102
- 8. Dayer MJ, Jones S, Prendergast B, Baddour LM, Lockhart PB, Thornhill MH. Incidence of infective endocarditis in England, 2000–13: a secular trend, interrupted time-series analysis. Lancet. 2015;385(9974):1219–1228. doi:10.1016/S0140-6736(14)62007-9
- 9. Thornhill MH, Dayer MJ, Lockhart PB, et al. Guidelines on prophylaxis to prevent infective endocarditis. British Dental Journal. 2017;223(2):80–84. doi:10.1038/sj.bdj.2017.628
- 10. Antimicrobial Expert Advisory Committee. Therapeutic guidelines: antibiotic. Version 17. Melbourne: Therapeutic Guidelines Limited; 2024. [Referenced for prescribing alignment; not cited as standalone guideline.]
- 11. Ferrieri P, Gewitz MH, Gerber MA, et al. Unique features of infective endocarditis in childhood. Circulation. 2002;105(17):2115–2126. doi:10.1161/01.CIR.0000016344.93228.EE
- 12. Patient safety alerts on antibiotic prophylaxis. Australian Commission on Safety and Quality in Health Care (ACSQHC). National Safety and Quality Health Service Standards. Sydney: ACSQHC; 2021.