📋 Key Information Summary
- Coronary revascularisation encompasses percutaneous coronary intervention (PCI) and coronary artery bypass grafting (CABG), guided by clinical presentation, anatomical complexity (SYNTAX score), left ventricular function, comorbidities, and patient preference via a Heart Team approach.
- Drug-eluting stents (DES) are preferred over bare-metal stents (BMS) in nearly all PCI scenarios due to significantly lower rates of in-stent restenosis and target-lesion revascularisation.
- Dual antiplatelet therapy (DAPT) duration post-PCI: ≥12 months after ACS, ≥6 months for stable CAD with DES (shortened to 1–3 months with newer-generation DES in selected cases), and 1 month only for BMS.
- CABG remains superior to PCI for left main coronary artery (LMCA) disease with intermediate-to-high SYNTAX score (≥23), triple-vessel disease (especially SYNTAX ≥23), and patients with diabetes mellitus and multivessel disease.
- The SYNTAX score II 2020 integrates anatomical complexity with clinical variables (age, creatinine clearance, LVEF, COPD, PVD) to generate individualised PCI vs CABG mortality predictions.
- Chronic total occlusion (CTO) PCI has improved with antegrade dissection re-entry and retrograde techniques; procedural success rates at experienced Australian centres exceed 85%.
- Rotational atherectomy (Rotablator®) is indicated for severely calcified lesions that prevent stent delivery or adequate expansion; available at major Australian PCI centres.
- Stent thrombosis is a rare but life-threatening complication (<1% with newer-generation DES); emergency PCI with aspiration thrombectomy and escalation of antiplatelet therapy is the standard management.
- In-stent restenosis is managed with drug-coated balloons (DCB) or repeat DES implantation; intravascular imaging (IVUS/OCT) is essential to guide treatment.
- Transradial access is the default approach for PCI in Australia, associated with lower major bleeding and vascular complications compared with transfemoral access.
- Periprocedural myocardial infarction (Type 4a MI) occurs in 5–30% of PCI cases depending on definition; troponin surveillance is mandatory post-procedure.
- Aboriginal and Torres Strait Islander Australians have 1.7× higher rates of coronary revascularisation, present later with more severe disease, and face barriers to accessing specialist cardiac services in remote regions.
Introduction & Australian Epidemiology
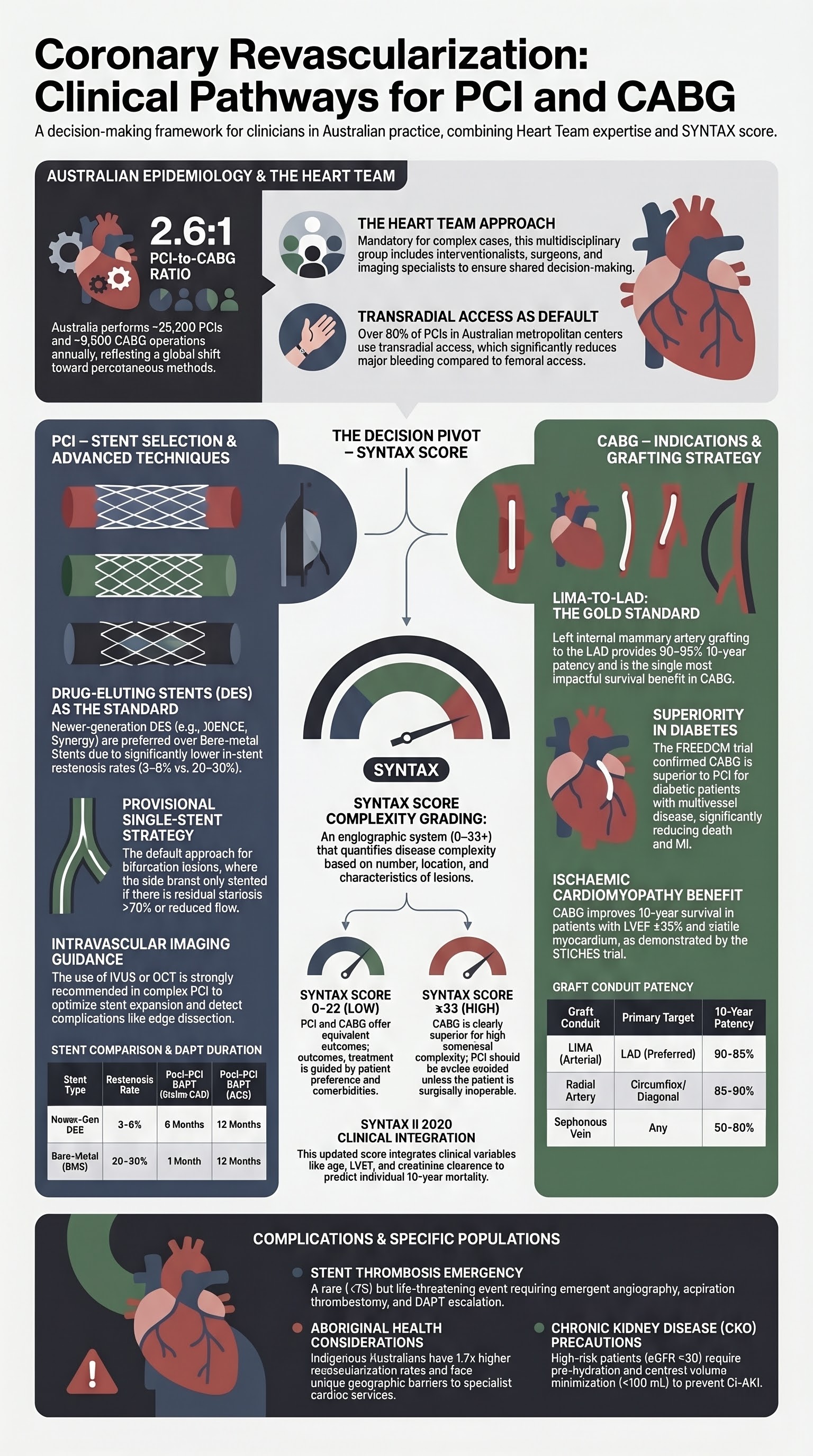
Coronary revascularisation — comprising percutaneous coronary intervention (PCI) and coronary artery bypass grafting (CABG) — is a cornerstone of management for obstructive coronary artery disease (CAD). In Australia, over 25,000 PCI procedures and approximately 10,000 CABG operations are performed annually, making revascularisation one of the most common therapeutic interventions in the health system.
The Australian Institute of Health and Welfare (AIHW) reports that ischaemic heart disease remains the leading cause of death in Australia, accounting for over 17,000 deaths in 2022. Coronary revascularisation is indicated across the spectrum of acute coronary syndromes (ACS) — ST-elevation myocardial infarction (STEMI), non-ST-elevation ACS (NSTEACS) — and chronic coronary syndromes (CCS) with refractory symptoms or high-risk anatomy despite optimal medical therapy (OMT).
Contemporary revascularisation practice in Australia is guided by the Cardiac Society of Australia and New Zealand (CSANZ) consensus statements, the European Society of Cardiology (ESC) / European Association for Cardio-Thoracic Surgery (EACTS) myocardial revascularisation guidelines, and National Heart Foundation of Australia (NHF) clinical recommendations. The multidisciplinary Heart Team — comprising interventional cardiologists, cardiac surgeons, imaging specialists, and allied health — is the recommended model for complex decision-making.
Trends in Australian practice include increasing use of newer-generation DES (everolimus- and zotarolimus-eluting), growing adoption of intravascular imaging-guided PCI (IVUS and OCT), expanding CTO programs, and an emerging role for transcatheter techniques in structural heart disease that complement traditional revascularisation.
PCI Indications & Techniques
Indications for PCI
PCI is indicated across a broad clinical spectrum:
- Primary PCI for STEMI: Emergent PCI of the culprit lesion within 120 minutes of first medical contact (FMC) is the gold standard reperfusion strategy. Door-to-balloon time target: ≤90 minutes at PCI-capable centres, ≤120 minutes for transfer patients.
- Early invasive strategy for NSTEACS: Coronary angiography ± PCI within 24 hours for high-risk features (GRACE score >140, dynamic ECG changes, haemodynamic instability, recurrent angina). Very-high-risk features mandate immediate (<2 hours) angiography.
- Stable chronic coronary syndromes: PCI for angina refractory to OMT, or in selected patients with significant stenosis (>90%) and demonstrable ischaemia on functional testing (FFR ≤0.80 or iFR ≤0.89). Routine PCI for stable CAD without ischaemia assessment is not recommended.
- Left main stem (LMS) PCI: Increasingly performed for ostial/shaft LMS disease and selected distal bifurcation LMS disease with low-intermediate SYNTAX score, as an alternative to CABG.
Stent Selection: DES vs BMS
| Feature | Drug-Eluting Stent (DES) | Bare-Metal Stent (BMS) |
|---|---|---|
| In-stent restenosis rate | 3–8% (newer-generation) | 20–30% |
| Stent thrombosis rate | 0.5–1.0% per year (early DES: higher) | 1–2% per year |
| Minimum DAPT duration | 3–6 months (6–12 months post-ACS) | 1 month |
| Preferred platform | Thin-strut cobalt-chromium or platinum-chromium | Stainless steel |
| Australian PBS listing | Commonwealth-funded under Prostheses List | Commonwealth-funded under Prostheses List |
Contemporary DES Platforms Available in Australia
Bifurcation Lesion PCI
Bifurcation lesions account for approximately 15–20% of all PCI. The provisional single-stent strategy (main vessel stenting with provisional side-branch intervention) is the default approach and is supported by the DKCRUSH-V, Nordic-Baltic Bifurcation Study IV, and BBC ONE trial data.
- Provisional stenting (preferred): Stent the main vessel first; only stent the side branch if there >70% residual stenosis, reduced TIMI flow, or dissection after main vessel stenting. Final kissing balloon inflation (FKBI) is recommended if side-branch intervention is performed.
- Planned two-stent techniques: Reserved for true bifurcations with large side branches (≥2.5 mm) with significant disease extending >5 mm into the side branch. Culotte, T-stent, and DK-crush techniques are available. DK-crush has the best evidence for LMS bifurcation (DKCRUSH-V: lower 3-year target-lesion failure vs provisional).
- Intravascular imaging: IVUS or OCT is strongly recommended for bifurcation PCI to optimise stent expansion, detect geographic miss, and confirm side-branch ostial coverage.
Chronic Total Occlusion (CTO) Interventions
CTOs are found in 15–30% of patients undergoing coronary angiography but account for only 5–10% of PCI attempts, reflecting technical complexity. Indications for CTO PCI include refractory angina despite OMT, heart failure with viable myocardium in the CTO territory, and patient preference after informed discussion of risks and benefits.
Rotational Atherectomy
Rotational atherectomy (RA) using the Rotablator® system (Boston Scientific) is indicated for severely calcified coronary lesions that cannot be crossed by a balloon or where adequate stent expansion is unlikely without lesion preparation. The diamond-coated burr ablates calcific plaque into microparticles (<5 μm) that are cleared by the reticuloendothelial system.
| Parameter | Detail |
|---|---|
| Burr sizes available | 1.25 mm, 1.50 mm, 1.75 mm, 2.00 mm, 2.15 mm, 2.25 mm, 2.50 mm |
| Starting burr | 1.25 mm (burr-to-artery ratio ~0.4–0.5) |
| Burr speed | 135,000–180,000 rpm |
| Rotaglide® solution | Heparinised saline + nitroglycerin + verapamil + Rotaglide (reduces friction and spasm) |
| Contraindications | Saphenous vein graft lesions, thrombus-laden lesions, severe LV dysfunction (EF <25%) — relative, dissection, severe angulation (>60°) |
| Complications | No-reflow (2–6%), perforation (<1%), burr entrapment (rare), slow flow, spasm |
| Australian availability | All major public and private PCI-capable centres |
Intravascular Imaging-Guided PCI
The ILUMIEN IV (OCT-guided) and RENOVATE-COMPLEX-PCI (IVUS-guided) trials demonstrated that intravascular imaging-guided PCI improves clinical outcomes compared with angiography-guided PCI, particularly in complex lesions (LMCA, long lesions, bifurcations, calcified lesions). CSANZ recommends IVUS or OCT use during complex PCI where available.
- IVUS: Provides cross-sectional vessel imaging with plaque characterisation, measurement of vessel diameter and lesion length, assessment of stent expansion and apposition. Useful for LMS assessment and calcified lesions.
- OCT: Higher resolution (10–20 μm vs 100–200 μm for IVUS), superior for assessing stent strut coverage, dissection flaps, and thrombus. Requires contrast flush. Limited by vessel diameter >3.0 mm for adequate imaging.
- FFR/iFR physiology: Fractional flow reserve (FFR ≤0.80) and instantaneous wave-free ratio (iFR ≤0.89) are the standard invasive physiology assessments. FAME 3 confirmed FFR-guided PCI is superior to angiography-guided PCI in multivessel disease. iFR does not require adenosine, improving patient comfort and reducing procedural time.
CABG Indications
CABG remains the revascularisation strategy of choice for several high-risk anatomical and clinical scenarios. Contemporary CABG in Australia is performed with a strong emphasis on arterial grafting — particularly left internal mammary artery (LIMA) to the left anterior descending (LAD) artery — and increasing use of bilateral internal mammary arteries (BIMA) and radial artery grafts.
Class I Indications for CABG
- Left main coronary artery (LMCA) disease: CABG is indicated for significant LMCA stenosis (≥50%) regardless of symptoms. PCI is a reasonable alternative for LMCA disease with SYNTAX score 0–22 and for intermediate SYNTAX (23–32) in selected patients; CABG is preferred for SYNTAX ≥33.
- Triple-vessel disease (3VD): CABG is the preferred revascularisation strategy, particularly with SYNTAX ≥23. The SYNTAX trial 10-year data demonstrated CABG superiority over PCI with first-generation DES for 3VD (mortality: CABG 22% vs PCI 29%, p=0.006 for SYNTAX ≥23).
- Diabetes with multivessel disease: The FREEDOM trial (2012) demonstrated CABG superiority over PCI in diabetic patients with multivessel disease (composite of death, MI, stroke at 5 years: 18.7% CABG vs 26.6% PCI, p=0.005). CABG is Class I recommended for DM with 2- or 3-vessel disease.
- Ischaemic cardiomyopathy with viable myocardium: CABG improves survival in patients with LVEF ≤35% and viable myocardium in ≥4 dysfunctional segments (STICH trial, STICHES 10-year follow-up). Requires viability assessment (PET, dobutamine echo, or cardiac MRI with late gadolinium enhancement).
- Failed PCI or anatomy unsuitable for PCI: Diffuse disease, heavy calcification precluding stent delivery, or failed CTO PCI with ongoing ischaemia.
SYNTAX Score Application
The SYNTAX score is an angiographic grading system that quantifies coronary artery disease complexity based on the number, location, and characteristics of lesions. It is calculated from 12 coronary segments and incorporates lesion dominance, bifurcations, CTOs, calcification, thrombus, and diffuse disease.
Graft Strategy in CABG
| Graft Conduit | Target | 10-Year Patency | Comment |
|---|---|---|---|
| Left internal mammary artery (LIMA) | LAD (preferred) | 90–95% | Gold standard; survival benefit established |
| Right internal mammary artery (RIMA) | RCA / circumflex | 85–90% | BIMA recommended in selected patients <70 yr; slightly higher sternal wound infection risk (diabetes caution) |
| Radial artery (RA) | Circumflex / diagonal | 85–90% | ART trial: RA graft may be superior to SVG; Allen test pre-operatively mandatory |
| Saphenous vein graft (SVG) | Any coronary target | 50–60% | Most commonly used conduit for non-LAD targets; attrition from intimal hyperplasia and atherosclerosis |
Off-Pump vs On-Pump CABG
On-pump CABG with cardiopulmonary bypass remains the standard technique. Off-pump CABG (OPCAB) avoids cardiopulmonary bypass and may benefit patients with heavily atheromatous aorta, severe renal impairment, or high neurological risk. However, the ROOBY and CORONARY trials showed no long-term mortality benefit for OPCAB, with a signal toward lower graft patency. Australian practice: on-pump is the default; OPCAB at surgeon discretion for selected cases.
PCI vs CABG Decision-Making
The Heart Team Approach
The Heart Team meeting should include:
- Interventional cardiologist — review of coronary anatomy, SYNTAX score, feasibility of complete revascularisation by PCI
- Cardiac surgeon — operative risk assessment (EuroSCORE II, STS score), conduit availability, technical feasibility of CABG
- Non-invasive cardiologist or imaging specialist — LV function, viability assessment, functional testing results
- The patient — informed discussion of risks, benefits, alternatives, recovery time, and personal preferences
SYNTAX Score II 2020
The SYNTAX Score II 2020 refines the original anatomical SYNTAX score by incorporating clinical variables to generate individualised predictions of 4-year and 10-year mortality for PCI vs CABG. Variables include:
- Anatomical SYNTAX score
- Age
- Creatinine clearance (Cockcroft-Gault)
- Left ventricular ejection fraction (LVEF)
- Chronic obstructive pulmonary disease (COPD)
- Peripheral vascular disease (PVD)
- Sex
- Diabetes mellitus
Key Trial Evidence: PCI vs CABG
| Trial | Population | Key Finding | Follow-Up |
|---|---|---|---|
| SYNTAX (2009, 2019) | 3VD ± LMS | CABG superior to PCI (first-gen DES) for 3VD with SYNTAX ≥23; equivalent for LMS with low SYNTAX | 10 years |
| FREEDOM (2012) | DM + MVD | CABG superior to PCI (5-yr composite: 18.7% vs 26.6%) | 5 years (7.5 yr extended) |
| EXCEL (2019) | LMS (SYNTAX ≤32) | PCI non-inferior to CABG for primary composite at 5 years; stroke lower with PCI; revascularisation higher with PCI | 5 years |
| NOBLE (2020) | LMS | PCI not non-inferior to CABG for MACCE at 5 years (29% vs 19%) | 5 years |
| STICH / STICHES (2016) | LVEF ≤35% + CAD | CABG + OMT superior to OMT alone for 10-year survival (HR 0.84) | 10 years |
| ISCHEMIA (2020) | Stable CAD, moderate-severe ischaemia | Initial invasive strategy did not reduce death/MI vs OMT; revascularisation improved angina-related quality of life | 3.2 years median |
| FAME 3 (2022) | 3VD (FFR-guided PCI vs CABG) | FFR-guided PCI not non-inferior to CABG for 1-year MACCE (10.6% vs 6.9%) | 1 year |
Surgical Risk Assessment
Surgical risk stratification is essential for the Heart Team. Two validated scoring systems are used in Australian practice:
- EuroSCORE II: Predicts in-hospital mortality for cardiac surgery. Variables include age, sex, renal function, cardiac status, recent MI, pulmonary disease, neurological disease, extracardiac arteriopathy, active endocarditis, critical preoperative state, diabetes on insulin, NYHA class, CCS class 4 angina, LV function, pulmonary hypertension, urgency, weight of intervention, and thoracic aorta surgery.
- STS Risk Score (Society of Thoracic Surgeons): Predicts operative mortality and morbidity for isolated CABG. Widely used in Australian cardiac surgery units. An STS predicted mortality >5% identifies high-risk patients.
- Frailty assessment: Gait speed, grip strength, cognitive function (Montreal Cognitive Assessment), and nutritional status. Frailty is an independent predictor of poor post-CABG outcomes and should be incorporated into decision-making.
Patient Preferences and Shared Decision-Making
Patient-centred care requires that revascularisation decisions incorporate individual values and preferences:
- Recovery time: PCI typically allows return to normal activity within 1–2 weeks; CABG requires 6–12 weeks for sternal healing and full recovery.
- Stroke risk: CABG carries a 1–2% perioperative stroke risk (higher in elderly, aortic atherosclerosis); PCI stroke risk is <0.5%.
- Repeat revascularisation: PCI has higher rates of repeat revascularisation (5–15% at 5 years) vs CABG (2–5%).
- DAPT commitment: PCI mandates prolonged DAPT; CABG does not require DAPT post-operatively (unless recent ACS or LIMA graft concern).
- Angina relief: CABG provides more complete and durable angina relief, especially with multivessel disease.
Complications & Management
Stent Thrombosis
| Classification | Timing | Incidence (newer DES) | Common Causes |
|---|---|---|---|
| Acute (<24 hours) | 0–24 hours post-PCI | 0.5–1.0% | Inadequate stent expansion, dissection, no-reflow, clopidogrel non-response |
| Subacute (1–30 days) | 1–30 days post-PCI | 0.5–2.0% | Premature DAPT cessation, clopidogrel resistance, malapposition |
| Late (1–12 months) | 1–12 months post-PCI | 0.2–0.5% | Delayed endothelialisation, chronic malapposition, neoatherosclerosis |
| Very late (>12 months) | >12 months post-PCI | 0.2–0.4%/yr | Neoatherosclerosis, stent malapposition, uncovered struts, polymer hypersensitivity |
Management of stent thrombosis:
- Emergency coronary angiography with aspiration thrombectomy (Export® catheter)
- Intravascular imaging (IVUS or OCT) to identify the mechanism — underexpansion, malapposition, geographic miss, edge dissection, neoatherosclerosis
- Treat the underlying cause: high-pressure balloon dilatation, additional stenting for dissection or geographic miss
- GP IIb/IIIa inhibitor (abciximab or eptifibatide) if not already administered
- Confirm or escalate antiplatelet therapy: switch from clopidogrel to ticagrelor (Brilinta®) 90 mg BD or prasugrel (Effient®) 10 mg OD (if not already on these agents)
- Check platelet function testing (VerifyNow® P2Y12 assay) if clopidogrel resistance suspected — available at major Australian centres
- Extended DAPT consideration: ≥12 months (or lifelong) if stent thrombosis occurred despite DAPT
In-Stent Restenosis (ISR)
In-stent restenosis is the recurrence of significant luminal narrowing (>50%) within a stented segment. Presentation ranges from asymptomatic (detected on routine surveillance) to ACS. ISR rates with newer-generation DES are 3–8%, compared with 20–30% for BMS.
Periprocedural Myocardial Infarction (Type 4a MI)
Type 4a MI is defined as an elevation of cardiac troponin (>5× 99th percentile upper reference limit [URL]) within 48 hours of PCI, with either (a) symptoms of myocardial ischaemia, (b) new ischaemic ECG changes, (c) angiographic loss of patency of a major coronary artery, or (d) imaging evidence of new loss of viable myocardium. The incidence ranges from 5–30% depending on the definition used and the complexity of the lesion.
- Prevention: Adequate pre-treatment with DAPT, intravascular imaging to avoid geographic miss, careful side-branch protection during bifurcation PCI, distal protection devices for SVG interventions, and avoidance of slow/no-reflow with appropriate lesion preparation.
- Post-PCI troponin surveillance: All patients should have serial high-sensitivity troponin (hs-cTn) measured at 6–12 hours post-PCI. Routine post-PCI troponin elevation (1–5× URL) is common and generally benign; elevation >5× URL with clinical correlate requires further investigation.
- Management: Angiographic re-look if troponin rise is significant with ECG or haemodynamic changes. Treat the cause (side-branch occlusion, distal embolisation, no-reflow). GP IIb/IIIa inhibitors and intracoronary vasodilators (nitroprusside, adenosine, verapamil) for no-reflow.
Vascular Access Complications
| Complication | Access Site | Incidence | Management |
|---|---|---|---|
| Radial artery occlusion (RAO) | Radial | 1–10% (usually asymptomatic) | Patency haemostasis (TR Band®), adequate anticoagulation (ACT >250s), ipsilateral ulnar artery compression post-procedure. Usually recanalises spontaneously. |
| Radial artery spasm | Radial | 5–15% | Intra-arterial vasodilators (nitroglycerin 200 μg + verapamil 2.5 mg ± lidocaine 20 mg). Hydrophilic-coated sheaths reduce spasm. |
| Haematoma (large) | Femoral > radial | TFA: 2–6%; TRA: <1% | Prolonged compression, reversal of anticoagulation, surgical evacuation if expanding or compartment syndrome suspected. |
| Retroperitoneal haemorrhage | Femoral | 0.5–1.0% | CT abdomen/pelvis, fluid resuscitation, blood transfusion, reversal of anticoagulation. Embolisation or surgical repair if ongoing bleeding. |
| Pseudoaneurysm | Femoral | 0.5–2.0% | Ultrasound-guided thrombin injection (first-line). Surgical repair if >3 cm, expanding, infected, or failed thrombin injection. |
| Arteriovenous fistula | Femoral | 0.1–0.5% | Usually self-limiting. Ultrasound-guided compression or surgical repair if persistent (>4 weeks) or symptomatic. |
| Compartment syndrome | Radial or femoral | <0.1% | Surgical emergency — fasciotomy. Continuous monitoring of limb perfusion is mandatory after large haematoma. |
Periprocedural Antiplatelet and Anticoagulation Strategy
Optimal pharmacotherapy is critical to minimise both ischaemic and bleeding complications:
DAPT Duration Recommendations
| Clinical Scenario | Minimum DAPT | Preferred P2Y12 Agent | Notes |
|---|---|---|---|
| STEMI / ACS post-PCI (any stent) | 12 months | Ticagrelor 90 mg BD or prasugrel 10 mg OD | Clopidogrel only if high bleeding risk or contraindication to ticagrelor/prasugrel |
| Stable CAD, DES, low bleeding risk | 6 months | Clopidogrel 75 mg OD or ticagrelor 60 mg BD | May extend to 12 months if high ischaemic risk |
| Stable CAD, DES, high bleeding risk | 1–3 months | Clopidogrel 75 mg OD | Newer-generation DES (SYNERGY, Onyx) allow short DAPT; guided by DAPT score and PRECISE-DAPT score |
| BMS implantation (rare) | 1 month | Clopidogrel 75 mg OD | BMS rarely used; consider only if DAPT absolutely contraindicated >1 month |
| LMS / complex PCI (SYNTAX ≥23) | 12 months (consider longer) | Ticagrelor or prasugrel preferred | Consider extended DAPT (up to 36 months) if high ischaemic / low bleeding risk |
Special Populations
Pregnancy
Paediatrics
Elderly (≥75 years)
Renal Impairment
Hepatic Impairment
Immunocompromised
Aboriginal and Torres Strait Islander Health Considerations
Aboriginal and Torres Strait Islander Australians experience cardiovascular disease at 1.4 times the rate of non-Indigenous Australians and have significantly higher rates of coronary revascularisation, particularly at younger ages. The AIHW reports that Indigenous Australians are hospitalised for coronary revascularisation at 1.7 times the rate of non-Indigenous Australians, with the disparity greatest in remote and very remote areas.
📚 References
- 1. Neumann FJ, Sousa-Uva M, Ahlsson A, et al. 2018 ESC/EACTS Guidelines on myocardial revascularization. Eur Heart J. 2019;40(2):87-165.
- 2. Serruys PW, Morice MC, Kappetein AP, et al. Percutaneous coronary intervention versus coronary-artery bypass grafting for severe coronary artery disease. N Engl J Med. 2009;360(10):961-972. [SYNTAX trial]
- 3. Farkouh ME, Domanski M, Sleeper LA, et al. Strategies for multivessel revascularization in patients with diabetes. N Engl J Med. 2012;367(25):2375-2384. [FREEDOM trial]
- 4. Stone GW, Kappetein AP, Sabik JF, et al. Five-year outcomes after PCI or CABG for left main coronary disease. N Engl J Med. 2019;381(19):1820-1830. [EXCEL trial]
- 5. Holm NR, Mäkikallio T, Lindsay MM, et al. Percutaneous coronary angioplasty versus coronary artery bypass grafting in the treatment of unprotected left main stenosis: updated 5-year outcomes from the randomised, non-inferiority NOBLE trial. Lancet. 2020;395(10219):191-199.
- 6. Fearon WF, Nishi T, De Bruyne B, et al. Clinical outcomes and cost-effectiveness of fractional flow reserve–guided percutaneous coronary intervention in patients with stable coronary artery disease: three-year follow-up of the FAME 3 trial. Circulation. 2023;147(11):840-849.
- 7. Maron DJ, Hochman JS, Reynolds HR, et al. Initial invasive or conservative strategy for stable coronary disease. N Engl J Med. 2020;382(15):1395-1407. [ISCHEMIA trial]
- 8. Authors/Group Writing Committee, Velazquez EJ, Lee KL, et al. Coronary-artery bypass surgery in patients with ischemic cardiomyopathy. N Engl J Med. 2016;374(16):1511-1520. [STICHES]
- 9. Farooq V, van Klaveren D, Steyerberg EW, et al. Anatomical and clinical characteristics to guide decision making between coronary artery bypass surgery and percutaneous coronary intervention for individual patients: development and validation of SYNTAX score II. Lancet. 2013;381(9867):639-650. [SYNTAX Score II]
- 10. Authors/Group MATRIX Investigators. Radial versus femoral access in patients with acute coronary syndromes undergoing invasive management: a randomised, multicentre, open-label trial. Lancet. 2015;385(9986):2465-2476.
- 11. Authors/Group ILUMIEN IV: OPTIMAL PCI Investigators. OCT-guided versus angiography-guided PCI for complex lesions. N Engl J Med. 2023;389(16):1477-1489.
- 12. Australian Institute of Health and Welfare (AIHW). Cardiovascular disease in Australia 2024. Canberra: AIHW; 2024. Cat. no. CVD 89.
- 13. National Heart Foundation of Australia and Cardiac Society of Australia and New Zealand. Australian clinical guidelines for the management of acute coronary syndromes 2023. Heart Lung Circ. 2023;32(8):909-975.
- 14. Authors/Group ART Trial Investigators. Bilateral versus single internal-thoracic-artery grafts at 5 years. N Engl J Med. 2016;375(26):2540-2549.
- 15. Authors/Group DKCRUSH-V Investigators. Randomized study on DK crush versus provisional stenting technique for treatment of distal unprotected left main bifurcation lesions: one-year final results. JACC Cardiovasc Interv. 2018;11(12):1134-1144.
- 16. Authors/Group RENOVATE-COMPLEX-PCI Investigators. Intravascular imaging-guided versus angiography-guided complex PCI. N Engl J Med. 2023;389(16):1477-1489.
- 17. Authors/Group Society of Thoracic Surgeons. STS risk calculator. Available at: https://riskcalc.sts.org. Accessed 2024.
- 18. Banks E, Crouch SR, Korda RJ, et al. Absolute risk of cardiovascular disease events, and blood pressure- and lipid-lowering therapy in Australia. Med J Aust. 2016;204(8):320.
- 19. Bravata DM, Gienger AL, McDonald KM, et al. Systematic review: the comparative effectiveness of percutaneous coronary interventions and coronary artery bypass graft surgery. Ann Intern Med. 2007;147(10):703-716.
- 20. Australian Commission on Safety and Quality in Health Care (ACSQHC). National Safety and Quality Health Service Standards. 2nd ed. Sydney: ACSQHC; 2021.