📋 Key Information Summary
- Atrial fibrillation (AF) confers a 4–5× increased stroke risk, with an annual stroke rate of ~5% in untreated non-valvular AF.
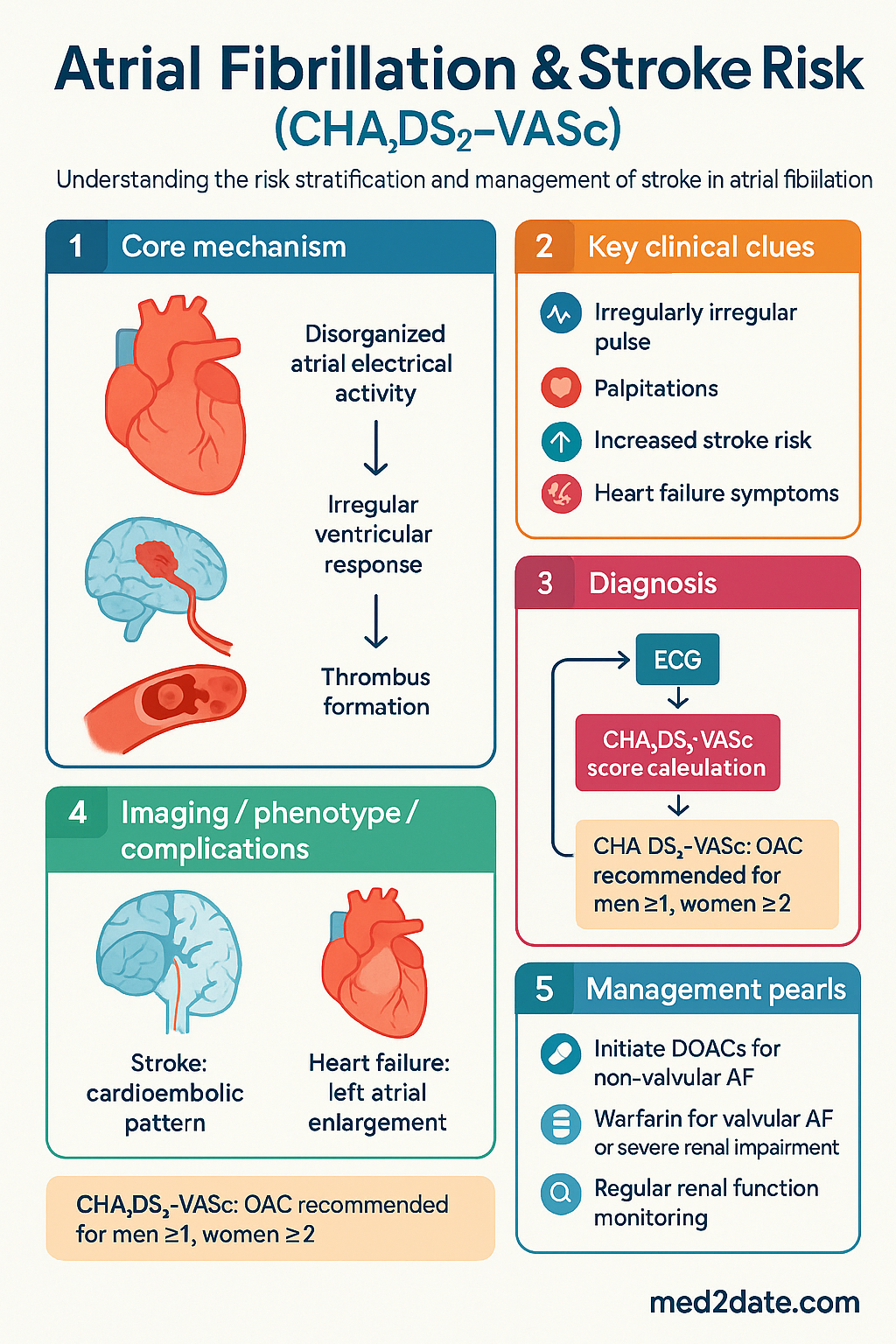
- The CHA₂DS₂-VASc score is the recommended Australian tool for stroke risk stratification in non-valvular AF.
- Oral anticoagulation (OAC) is indicated for men with CHA₂DS₂-VASc ≥1 and women with ≥2, balancing stroke prevention against bleeding risk.
- Direct oral anticoagulants (DOACs: apixaban, dabigatran, edoxaban, rivaroxaban) are first-line for most patients with non-valvular AF.
- Warfarin remains the OAC of choice for patients with mechanical heart valves, moderate-severe mitral stenosis, or severe renal impairment (eGFR <15 mL/min).
- The HAS-BLED score assesses major bleeding risk; a score ≥3 indicates 'high risk' but is not a contraindication to OAC—rather, it prompts modifiable risk factor management.
- Rhythm control strategies (pharmacological or catheter ablation) may be pursued for symptom improvement but do not replace the need for anticoagulation based on stroke risk.
- Cardioversion (electrical or pharmacological) requires at least 3 weeks of therapeutic anticoagulation prior, or transoesophageal echocardiography (TOE) to exclude left atrial thrombus.
- Special considerations apply for Aboriginal and Torres Strait Islander peoples, who experience higher AF prevalence and stroke mortality with reduced access to specialist care.
- Regular monitoring of renal function (at least annually) is essential for DOAC dose adjustment and ongoing safety.
- Reversal agents are available for all DOACs (idarucizumab for dabigatran; andexanet alfa for factor Xa inhibitors) and vitamin K for warfarin.
- Patient education on adherence, signs of stroke/TIA, and bleeding is critical, alongside a personalised management plan.
Introduction & Australian Epidemiology
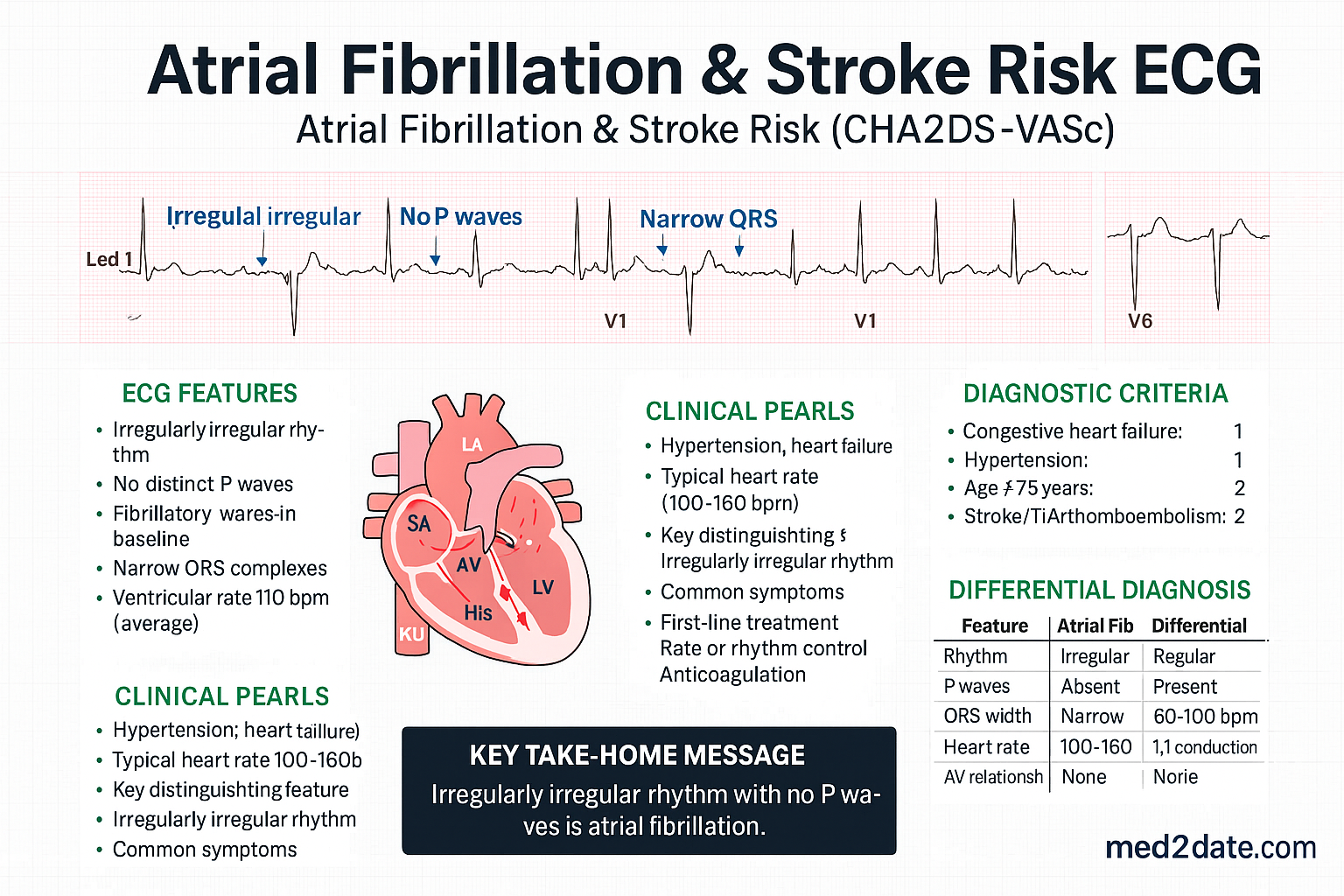
Atrial fibrillation (AF) is the most common sustained cardiac arrhythmia, characterised by disorganised atrial electrical activity leading to an irregularly irregular ventricular response. In Australia, AF prevalence increases with age, affecting approximately 2–4% of the adult population overall and >10% of those aged ≥80 years. The condition significantly elevates the risk of cardioembolic stroke, heart failure, and mortality.
Without anticoagulation, AF carries an annual stroke risk of approximately 5%, with strokes tending to be more severe and disabling than non-AF-related strokes. The landmark meta-analysis by Hart et al. demonstrated that adjusted-dose warfarin reduces stroke risk by 64%, while antiplatelet therapy alone reduces it by only 22%. The advent of direct oral anticoagulants (DOACs) has provided options with superior safety profiles, leading to their adoption as first-line therapy for non-valvular AF in Australian and international guidelines.
In Australia, AF management is guided by the National Heart Foundation of Australia/Cardiac Society of Australia and New Zealand (CSANZ) guidelines, which endorse the CHA₂DS₂-VASc score for risk stratification and recommend a patient-centred approach to anticoagulation, integrating bleeding risk assessment (HAS-BLED) and regular review.
Stroke Risk Stratification (CHA₂DS₂-VASc Score)
The CHA₂DS₂-VASc score is the validated tool recommended by Australian guidelines for estimating stroke risk in patients with non-valvular AF. It expands upon the older CHADS₂ score by incorporating additional common risk factors.
| Letter | Risk Factor | Points |
|---|---|---|
| C | Congestive heart failure (or left ventricular systolic dysfunction) | 1 |
| H | Hypertension | 1 |
| A₂ | Age ≥75 years | 2 |
| D | Diabetes mellitus | 1 |
| S₂ | Stroke, TIA, or thromboembolism history | 2 |
| V | Vascular disease (e.g., prior MI, peripheral arterial disease, aortic plaque) | 1 |
| A | Age 65–74 years | 1 |
| Sc | Sex category (female sex) | 1 |
Interpretation & Anticoagulation Recommendation (non-valvular AF):
- Score 0 (men) or 1 (women, solely for sex): No antithrombotic therapy.
- Score 1 (men) or 2 (women, with ≥1 non-sex point): OAC recommended.
- Score ≥2 (men) or ≥3 (women): OAC strongly recommended.
Note: The score does not apply to patients with valvular AF (mechanical valve or at least moderate mitral stenosis), who require warfarin. It also does not capture all factors (e.g., chronic kidney disease, biomarkers like elevated NT-proBNP), which may inform individualised decisions.
Bleeding Risk Assessment (HAS-BLED)
The HAS-BLED score is a practical tool to quantify major bleeding risk in AF patients on anticoagulation. Its primary role is to identify modifiable bleeding risk factors, not to withhold anticoagulation in patients who otherwise have an indication.
| Letter | Clinical Characteristic | Points |
|---|---|---|
| H | Hypension (uncontrolled, >160 mmHg systolic) | 1 |
| A | Abnormal renal function (dialysis, transplant, Cr ≥200 µmol/L) and/or liver function (cirrhosis, bilirubin >2× ULN, AST/ALT >3× ULN) | 1 or 2 |
| S | Stroke history | 1 |
| B | Bleeding history or predisposition (e.g., prior major bleed, anaemia) | 1 |
| L | Labile INR (TTR <60% if on warfarin) | 1 |
| E | Elderly (age >65 years) | 1 |
| D | Drugs (antiplatelets, NSAIDs) and/or alcohol (≥8 drinks/week) | 1 or 2 |
Interpretation:
- Score 0–2: Low-moderate bleeding risk.
- Score ≥3: High bleeding risk. This should prompt: 1) Correction of modifiable factors (e.g., strict blood pressure control, treat anaemia, avoid concomitant NSAIDs/antiplatelets if possible, improve warfarin TTR). 2) More frequent review and monitoring. 3) Consideration of a DOAC over warfarin where appropriate (DOACs have a lower risk of intracranial haemorrhage).
Anticoagulation Choices (Warfarin vs DOACs)
Choice of oral anticoagulant is individualised based on patient factors, comorbidities, and preference. DOACs are preferred for non-valvular AF due to their predictable pharmacokinetics, fewer food/drug interactions, and no routine coagulation monitoring requirement.
Direct Oral Anticoagulants (DOACs)
Warfarin
Indications for Warfarin over DOACs
- Mechanical heart valve.
- Moderate to severe mitral stenosis (typically rheumatic).
- Severe chronic kidney disease (eGFR <15 mL/min or on dialysis).
- Antiphospholipid syndrome with previous thrombosis.
- Patient preference or established stable INR control.
Perioperative Management
A standardised bridging protocol is essential. For DOACs, omission is based on renal function and procedure bleeding risk (typically 24–48 hours for low-risk procedures, 48–96 hours for high-risk). Warfarin is ceased 5 days pre-procedure, with LMWH bridging considered only for very high thrombotic risk.
Cardioversion & Rhythm Control
Rhythm control aims to restore and maintain sinus rhythm, improving symptoms and quality of life. It does not obviate the need for anticoagulation based on CHA₂DS₂-VASc score, as stroke risk persists from the underlying atrial myopathy.
Cardioversion Strategies
Pharmacological Rhythm Control
Antiarrhythmic drugs (AADs) are used for maintenance of sinus rhythm. Choice depends on underlying structural heart disease.
| Agent | Considerations |
|---|---|
| Flecainide | 'Pill-in-the-pocket' for paroxysmal AF in structurally normal hearts. Avoid in coronary artery disease or significant LV dysfunction. |
| Amiodarone | Highly effective but limited by long-term organ toxicity (thyroid, liver, lung, cornea). Requires baseline and periodic monitoring. |
| Sotalol | Non-cardioselective beta-blocker with Class III effect. Monitor QT interval and renal function. |
| Dronedarone | Less effective than amiodarone, but fewer non-cardiac side effects. Contraindicated in NYHA Class III–IV heart failure. |
Catheter Ablation
Pulmonary vein isolation (PVI) by catheter ablation is a Class I recommendation for symptomatic paroxysmal or persistent AF refractory to AADs. It is increasingly used as first-line therapy in selected patients. The procedure carries risks (e.g., ~1% risk of significant complications like cardiac tamponade, stroke, pulmonary vein stenosis). Post-ablation, anticoagulation is typically continued for at least 2 months and then based on CHA₂DS₂-VASc score.
Special Populations
Aboriginal and Torres Strait Islander Health Considerations
Aboriginal and Torres Strait Islander peoples experience a higher prevalence of AF, earlier onset, and significantly worse cardiovascular outcomes, including a 1.5–2× higher stroke mortality compared to non-Indigenous Australians. Management must be culturally safe and address systemic barriers.
📚 References
- 1. Brieger D, Amerena J, Attia J, et al. National Heart Foundation of Australia and Cardiac Society of Australia and New Zealand: Australian Clinical Guidelines for the Diagnosis and Management of Atrial Fibrillation 2018. Heart Lung Circ. 2018;27(10):1209-1266.
- 2. Hindricks G, Potpara T, Dagres N, et al. 2020 ESC Guidelines for the diagnosis and management of atrial fibrillation developed in collaboration with the European Association for Cardio-Thoracic Surgery (EACTS). Eur Heart J. 2021;42(5):373-498.
- 3. Lip GYH, Banerjee A, Boriani G, et al. Antithrombotic Therapy for Atrial Fibrillation: CHEST Guideline and Expert Panel Report. Chest. 2018;154(5):1121-1201.
- 4. January CT, Wann LS, Calkins H, et al. 2019 AHA/ACC/HRS Focused Update of the 2014 AHA/ACC/HRS Guideline for the Management of Patients With Atrial Fibrillation. Circulation. 2019;140(2):e125-e151.
- 5. Australian Institute of Health and Welfare (AIHW). Atrial fibrillation. Cat. no. CVD 89. Canberra: AIHW; 2022.
- 6. Connolly SJ, Ezekowitz MD, Yusuf S, et al. Dabigatran versus warfarin in patients with atrial fibrillation. N Engl J Med. 2009;361(12):1139-1151.
- 7. Granger CB, Alexander JH, McMurray JJV, et al. Apixaban versus warfarin in patients with atrial fibrillation. N Engl J Med. 2011;365(11):981-992.
- 8. Patel MR, Mahaffey KW, Garg J, et al. Rivaroxaban versus warfarin in nonvalvular atrial fibrillation. N Engl J Med. 2011;365(10):883-891.
- 9. Giugliano RP, Ruff CT, Braunwald E, et al. Edoxaban versus warfarin in patients with atrial fibrillation. N Engl J Med. 2013;369(22):2093-2104.
- 10. Pisters R, Lane DA, Nieuwlaat R, et al. A novel user-friendly score (HAS-BLED) to assess 1-year risk of major bleeding in patients with atrial fibrillation: the Euro Heart Survey. Chest. 2010;138(5):1093-1100.
- 11. Calkins H, Hindricks G, Cappato R, et al. 2017 HRS/EHRA/ECAS/APHRS/SOLAECE expert consensus statement on catheter and surgical ablation of atrial fibrillation. Heart Rhythm. 2017;14(10):e275-e444.
- 12. National Aboriginal Community Controlled Health Organisation (NACCHO). Cultural safety in practice. 2023.