📋 Key Information Summary
- Cardiac tamponade is a life-threatening condition caused by accumulation of fluid in the pericardial space, compressing the heart and impairing diastolic filling.
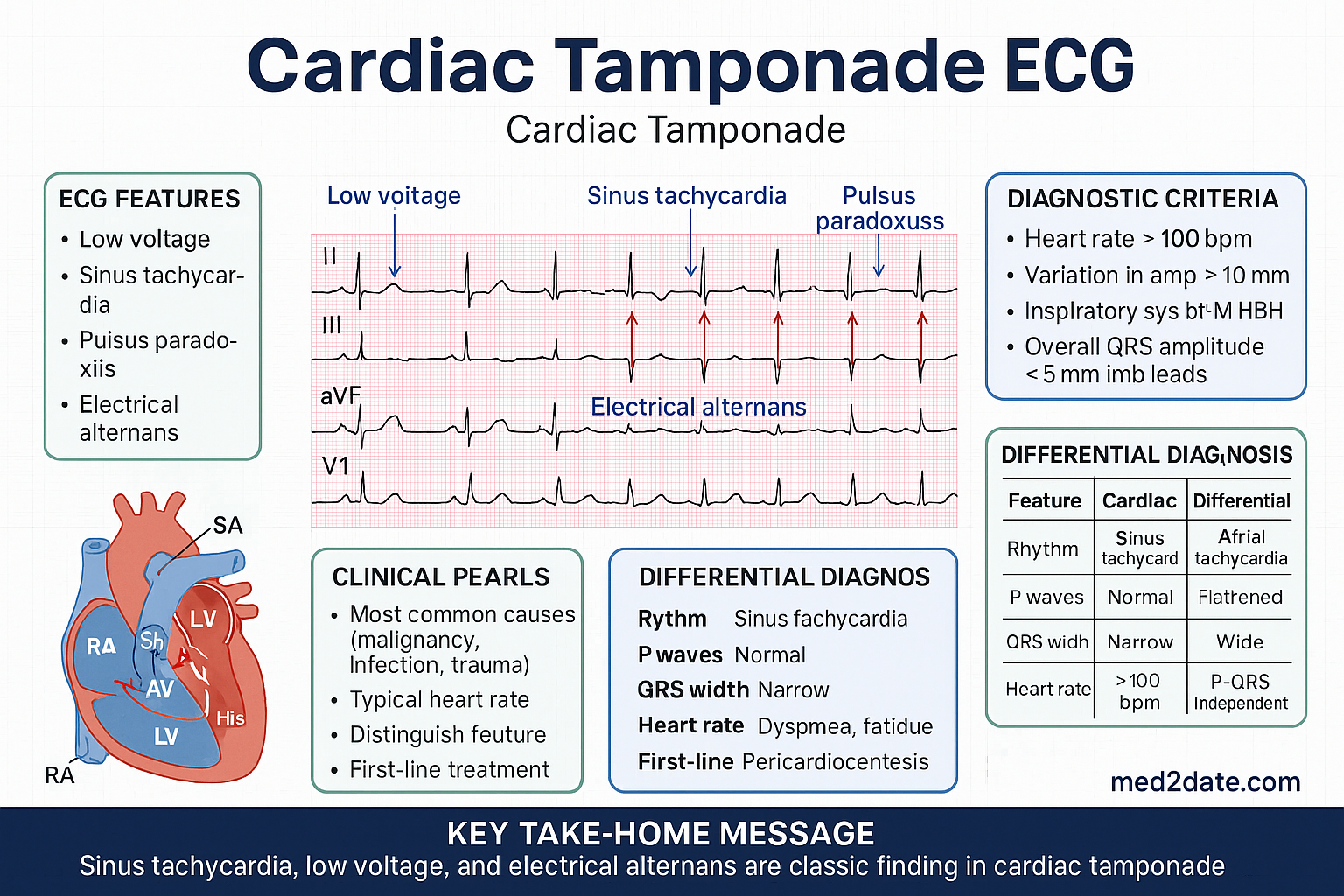
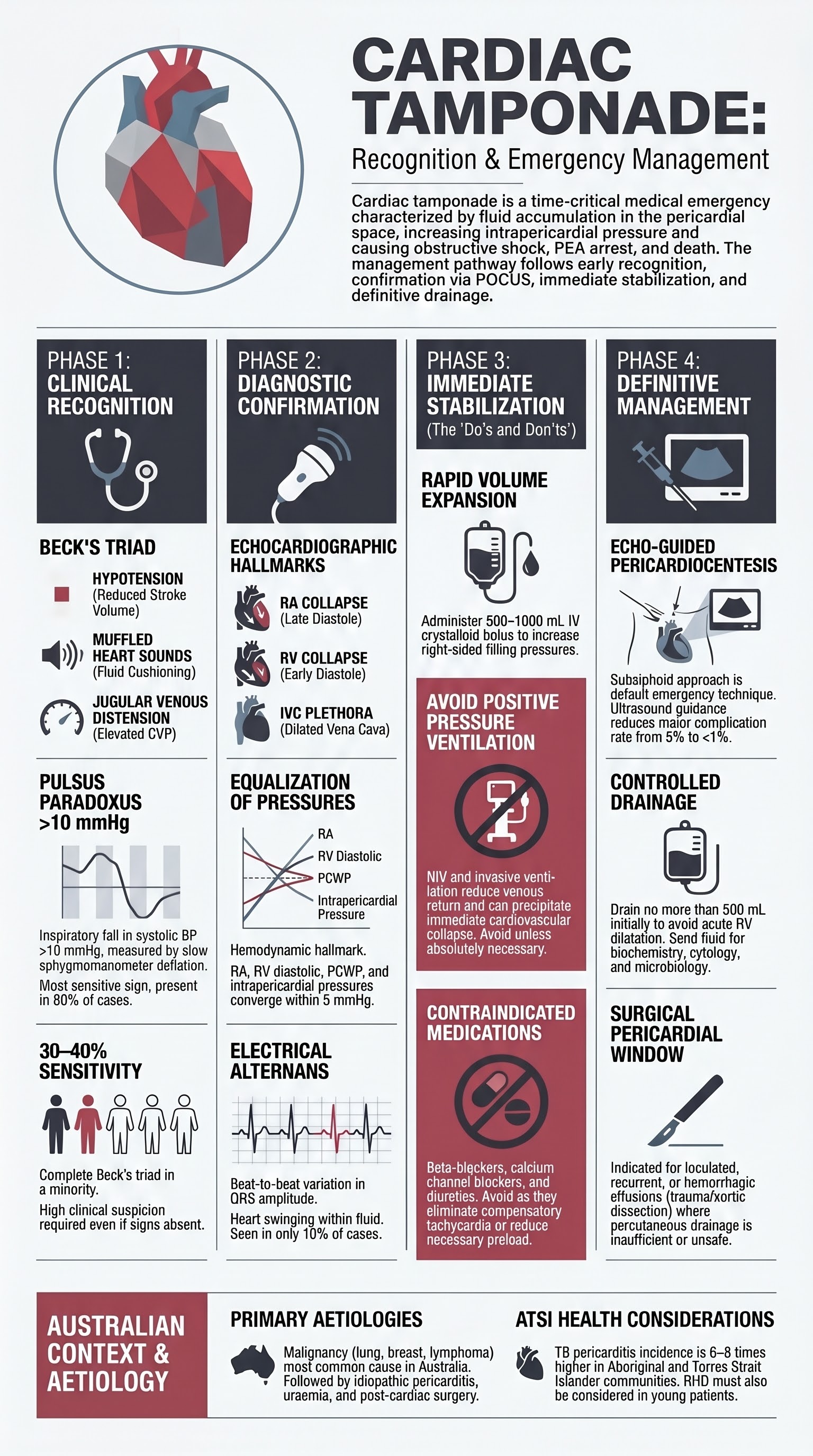
- Beck's triad — hypotension, muffled heart sounds, and jugular venous distension — is the classic clinical triad but is present in only a minority of patients at initial presentation.
- Pulsus paradoxus (an inspiratory fall in systolic BP >10 mmHg) is a sensitive clinical sign; measure with a sphygmomanometer by noting the first and last Korotkoff sounds heard during slow deflation.
- Transthoracic echocardiography (TTE) is the primary diagnostic modality: look for right atrial (RA) collapse in late diastole, right ventricular (RV) collapse in early diastole, and inferior vena cava (IVC) plethora (>50% inspiratory collapse absent).
- Hemodynamic hallmark is equalization of intracardiac pressures (RA, RV diastolic, pulmonary capillary wedge, and intrapericardial pressures all within 5 mmHg of each other) — confirmed on right heart catheterisation.
- Compensatory tachycardia and systemic vasoconstriction maintain cardiac output early; decompensation leads to obstructive shock and cardiac arrest (PEA rhythm).
- Immediate resuscitation: IV fluid bolus (500–1000 mL crystalloid), avoid positive-pressure ventilation (including non-invasive ventilation with high pressures), position patient sitting upright if tolerated.
- Definitive treatment is urgent drainage — emergency pericardiocentesis (subxiphoid approach, echo-guided preferred) or surgical pericardial window if loculated, recurrent, or haemorrhagic effusion.
- Complications of pericardiocentesis include cardiac chamber puncture, pneumothorax, coronary artery laceration, and arrhythmia — echo guidance reduces major complication rate from ~5% to <1%.
- All pericardial fluid must be sent for biochemistry (protein, LDH, glucose, ADA), cytology, microbiology (Gram stain, culture, TB culture/PCR), and cell count.
- Common aetiologies in Australia: malignancy (lung, breast, lymphoma), idiopathic/viral pericarditis, uraemia, hypothyroidism, post-cardiac surgery, and tuberculosis (especially in immunocompromised and ATSI communities).
- Monitor for reaccumulation with serial echocardiography; treat the underlying cause — antineoplastic therapy, dialysis, thyroid replacement, or anti-tuberculous therapy as appropriate.
Introduction & Australian Epidemiology
Cardiac tamponade is a medical emergency in which fluid accumulation within the pericardial sac raises intrapericardial pressure sufficiently to compress cardiac chambers, impair diastolic filling, and reduce cardiac output. If untreated, progressive obstructive shock leads to pulseless electrical activity (PEA) arrest and death.
The pericardium normally contains 15–50 mL of serous fluid. Tamponade physiology can develop acutely with as little as 100–200 mL of fluid if accumulation is rapid (e.g., traumatic haemopericardium), or may require >1–2 L if fluid accumulates slowly, allowing the pericardium to stretch and accommodate.
Australian Epidemiology
- Pericardial effusion is detected on echocardiography in approximately 3–5% of patients admitted to Australian tertiary hospitals with cardiac complaints.
- Malignancy is the most common cause of large pericardial effusions and tamponade in adults in Australia, with lung cancer, breast cancer, and lymphoma predominating.
- Post-cardiac surgery tamponade occurs in 0.5–2% of open-heart procedures; the incidence has decreased with improved surgical technique and routine post-operative echocardiography.
- Tuberculous pericarditis, though uncommon nationally, remains an important cause in immunocompromised populations and some remote communities. Australia records approximately 1,300 new TB notifications per year (AIHW, 2023).
- Uraemic pericarditis causing tamponade is seen in patients with end-stage kidney disease, particularly those with delayed or inadequate dialysis.
- Idiopathic and viral pericarditis accounts for a significant proportion of pericardial effusions, though most do not progress to tamponade.

Clinical Recognition
Beck's Triad
The classic triad described by Claude Beck in 1935 comprises:
Pulsus Paradoxus
Pulsus paradoxus is defined as an inspiratory decrease in systolic arterial blood pressure of >10 mmHg. It is the most sensitive clinical sign for cardiac tamponade, present in up to 80% of cases.
Measurement technique:
- Use a sphygmomanometer with the patient breathing normally (avoid deep breaths).
- Slowly deflate the cuff (2–3 mmHg per heartbeat).
- Note the pressure at which Korotkoff sounds are first heard (typically only during expiration).
- Continue deflating until Korotkoff sounds are heard throughout the respiratory cycle.
- The difference between these two values is the degree of pulsus paradoxus.
Echocardiographic Signs
Transthoracic echocardiography (TTE) is the primary diagnostic modality for cardiac tamponade. Key findings include:
| Echocardiographic Sign | Description | Sensitivity / Specificity |
|---|---|---|
| Right Atrial (RA) Collapse | Inward bowing of the RA free wall in late diastole / early systole (when RA pressure exceeds intrapericardial pressure). Duration >1/3 of the cardiac cycle is highly specific for tamponade. | Sensitivity 50–60%, Specificity ~95% |
| Right Ventricular (RV) Collapse | Inward bowing of the RV free wall in early diastole. More specific than RA collapse for tamponade physiology. Indicates higher intrapericardial pressures. | Sensitivity 60–90%, Specificity ~80–90% |
| IVC Plethora | Inferior vena cava diameter >2.1 cm with <50% inspiratory collapse (in spontaneously breathing patients). Reflects elevated right atrial pressure. | Sensitivity ~90%, Specificity ~50% |
| Respiratory Variation in Flow Velocities | >25% variation in mitral inflow E velocity and >40% variation in tricuspid inflow E velocity with respiration. Detected on pulse-wave Doppler. | Sensitivity ~80%, Specificity ~85% |
| Swinging Heart | Excessive cardiac motion within a large effusion — pendular swinging. Seen in large, often malignant effusions. | Low sensitivity; specific for large effusions |
Additional Clinical Features
- Tachycardia — compensatory increase in heart rate to maintain cardiac output.
- Tachypnoea — respiratory distress from diaphragmatic compression and reduced cardiac output.
- Electrical alternans on ECG — beat-to-beat variation in QRS amplitude caused by the heart swinging within the pericardial fluid. Highly specific but seen in only ~10% of tamponade cases. Low voltage QRS is more common.
- Pericardial knock — an early diastolic sound occasionally auscultated due to sudden cessation of ventricular filling.
- Hepatojugular reflux — sustained JVP elevation with right upper quadrant pressure (>3 cm increase sustained for >10 seconds).
- Cool peripheries, oliguria, and altered mental status indicate progressed obstructive shock.
Haemodynamic Consequences
Understanding the haemodynamic derangements of cardiac tamponade is essential for rational management. The fundamental pathophysiology is restriction of cardiac filling by elevated intrapericardial pressure.
Pathophysiology of Impaired Filling
- As pericardial fluid accumulates, intrapericardial pressure rises according to the pericardial pressure–volume relationship. The normal pericardium has limited compliance; once its reserve volume is exhausted, small additional volumes cause steep pressure increases.
- Elevated intrapericardial pressure is transmitted to all four cardiac chambers, compressing them and restricting diastolic filling.
- The right-sided chambers (RA and RV) are more compliant and therefore collapse first. Left-sided collapse occurs only in severe or rapidly accumulating tamponade.
Equalisation of Pressures
The haemodynamic hallmark of tamponade is the equalisation of intracardiac diastolic pressures with intrapericardial pressure. All of the following pressures converge to within 5 mmHg of each other:
| Pressure | Normal (mmHg) | Tamponade (mmHg) |
|---|---|---|
| Intrapericardial pressure | <0 (sub-atmospheric) | Elevated (equal to diastolic pressures) |
| Right atrial pressure (mean) | 2–6 | 12–20 |
| RV end-diastolic pressure | 1–5 | 12–20 |
| Pulmonary capillary wedge pressure | 6–12 | 12–20 |
| LV end-diastolic pressure | 5–12 | 12–20 |
Decreased Cardiac Output
- Impaired diastolic filling leads to reduced end-diastolic volume (preload).
- Stroke volume falls according to the Frank-Starling mechanism.
- Cardiac output is further compromised during inspiration — venous return to the right heart increases, but the ventricular septum bulges leftward (ventricular interdependence), reducing LV filling and output. This is the mechanism of pulsus paradoxus.
- In advanced tamponade, cardiac output becomes insufficient to maintain end-organ perfusion, resulting in obstructive shock.
Compensatory Tachycardia
- Baroreceptor-mediated sympathetic activation increases heart rate to compensate for reduced stroke volume and maintain cardiac output (CO = HR × SV).
- Systemic vascular resistance (SVR) rises via catecholamine-driven vasoconstriction, maintaining blood pressure initially but reducing peripheral perfusion.
- This compensatory phase may mask the severity of haemodynamic compromise — patients can appear relatively stable until sudden decompensation.
- Beta-blockers or calcium channel blockers may blunt the compensatory tachycardia and precipitate haemodynamic collapse in patients with undiagnosed tamponade.
Progression to Obstructive Shock
Emergency Management
Cardiac tamponade is a medical emergency requiring immediate intervention. The goals of initial management are to maintain cardiac output temporise while arranging definitive pericardial drainage.
Immediate Resuscitation Measures
Medications to Avoid
| Drug / Intervention | Risk |
|---|---|
| Beta-blockers (metoprolol, atenolol, carvedilol) | Eliminate compensatory tachycardia → cardiovascular collapse |
| Non-dihydropyridine CCBs (verapamil, diltiazem) | Negative chronotrope and inotrope → haemodynamic deterioration |
| Diuretics (furosemide, hydrochlorothiazide) | Reduce preload → critically worsens cardiac output in tamponade |
| Positive-pressure ventilation (NIV, invasive with high PEEP) | Reduces venous return → precipitous fall in cardiac output |
| Vasodilators (GTN, sodium nitroprusside) | Reduce afterload and preload → worsened hypotension |
Indications for Emergent vs Urgent Drainage
Pericardiocentesis
Indications
- Cardiac tamponade (haemodynamically compromised) — emergent
- Large pericardial effusion with echocardiographic signs of impending tamponade — urgent
- Diagnostic pericardiocentesis — suspected purulent pericarditis, tuberculosis, or malignancy
- Therapeutic drainage for symptomatic large effusion (dyspnoea, chest discomfort)
- Post-cardiac surgery tamponade (if catheter drainage feasible; otherwise surgical re-exploration)
Contraindications
- Absolute: Uncontrolled bleeding diathesis (INR >2.0, platelets <50 × 10⁹/L) — unless emergent and bleeding risk is outweighed by immediate risk of death.
- Relative: Loculated effusion (may require surgical drainage), aortic dissection with haemopericardium, posterior/dominant effusion inaccessible from subxiphoid approach.
- Note: In emergent tamponade, there are virtually no absolute contraindications — delay is more dangerous than the procedure.
Technique — Subxiphoid Approach
The subxiphoid (inferior) approach is the most commonly used technique for pericardiocentesis and is the recommended default approach, particularly in emergency settings.
Imaging Guidance
| Modality | Advantages | Limitations |
|---|---|---|
| Echocardiography-guided (preferred) | Real-time needle visualisation, identifies optimal puncture site, confirms pericardial entry, reduces complication rate (<1%), available at bedside | Operator-dependent; limited acoustic windows in obese, ventilated, or post-surgical patients |
| Fluoroscopy-guided | Useful in catheterisation laboratory setting, good for catheter positioning | Radiation exposure; requires transfer to cath lab; does not directly visualise the needle–heart relationship |
| CT-guided | Excellent for loculated, posterior, or complex effusions | Not real-time; requires transfer; time-consuming; not suitable for emergencies |
| Blind (landmark-only) | No imaging required; can be performed anywhere immediately | Higher complication rate (~5%); reserved for cardiac arrest or extreme emergencies with no imaging available |
Complications of Pericardiocentesis
| Complication | Incidence (echo-guided) | Management |
|---|---|---|
| Cardiac chamber puncture (RV most common) | 0.5–1% | Usually self-limiting; withdraw needle. Echocardiographic monitoring. Surgical repair if persistent bleeding. |
| Coronary artery laceration | <0.5% | Emergency surgical repair. Angiography and stenting if feasible. |
| Pneumothorax | 0.5–1% | Observation if small; intercostal catheter insertion if significant. |
| Arrhythmia (ventricular ectopy) | 1–3% | Withdraw needle; usually resolves. Anti-arrhythmic if sustained. |
| Recurrent effusion | 10–30% (depends on aetiology) | Repeat drainage; consider indwelling catheter, surgical pericardial window, or pericardiodesis. |
| Vagal reaction | 1–2% | Atropine 600 mcg IV if bradycardic. Trendelenburg positioning. |
Surgical Alternatives
Consider surgical drainage (pericardial window) when:
- Loculated effusion not amenable to percutaneous drainage
- Recurrent tamponade despite catheter drainage
- Haemorrhagic effusion (post-cardiac surgery, trauma, coagulopathy)
- Purulent pericarditis requiring thorough debridement
- Need for pericardial biopsy for diagnosis (suspected TB, malignancy)
- Aortic dissection with tamponade (emergent surgical repair)
Surgical approaches include subxiphoid pericardial window (local or general anaesthesia), video-assisted thoracoscopic surgery (VATS) pericardial window, and median sternotomy. The subxiphoid window is the most common surgical approach, providing reliable drainage with lower morbidity than thoracotomy.
Post-Drainage Care
Fluid Analysis
All pericardial fluid specimens should be sent for comprehensive analysis to identify the underlying aetiology:
| Investigation | Purpose | Key Findings |
|---|---|---|
| Gross appearance | Initial assessment | Serous (inflammatory/idiopathic), serosanguinous (malignancy, TB, post-MI), frankly bloody (trauma, malignancy, coagulopathy), purulent (bacterial infection), chylous (lymphatic obstruction) |
| Cell count & differential | Inflammatory vs. malignant vs. infective | Neutrophil predominance → bacterial infection; lymphocyte predominance → TB, viral, malignancy; elevated RBC → haemorrhagic |
| Protein & LDH | Exudate classification (Light's criteria adapted) | Pericardial/serum protein ratio >0.5 or pericardial/serum LDH ratio >0.6 → exudate |
| Glucose | Infection / rheumatoid | Very low (<1.1 mmol/L) → bacterial or tuberculous pericarditis, rheumatoid |
| Gram stain & culture | Bacterial infection | Low sensitivity (~50%); send blood cultures simultaneously. Consider 16S rRNA PCR. |
| AFB stain, culture & PCR | Tuberculosis | AFB culture takes 2–6 weeks; GeneXpert MTB/RIF on pericardial fluid has sensitivity ~60–70% and rapid turnaround |
| Adenosine deaminase (ADA) | TB screening | ADA >40 U/L strongly suggestive of tuberculous pericarditis in endemic populations |
| Cytology | Malignancy | Sensitivity 70–90% for malignant effusion; send ≥50 mL for optimal yield. Consider cell block preparation. |
| Fluid pH | Infection | pH <7.0 → purulent pericarditis (empyema) |
Monitoring for Reaccumulation
- Perform repeat echocardiography within 24–48 hours of drainage, then as clinically indicated (typically at 1 week, 1 month, and 3 months).
- Monitor the volume and character of fluid draining via the indwelling catheter — decreasing output suggests successful drainage; sudden cessation may indicate catheter blockage.
- The pericardial catheter is typically removed when drainage volume falls to <25–50 mL per 24 hours and repeat echocardiography shows no significant reaccumulation.
- Patients should be monitored in a high-dependency or cardiac monitoring setting for at least 24 hours post-drainage, with continuous telemetry and frequent vital sign assessment.
- Recurrence rates vary by aetiology: idiopathic/viral (~10–15%), malignancy (~30–50% without definitive treatment), uraemic (responds to dialysis), TB (responds to anti-tuberculous therapy).
Addressing Underlying Aetiology
Discharge Planning & Follow-Up
- Ensure the underlying aetiology has been identified and treatment initiated before discharge (or a clear management plan is in place).
- Arrange cardiology follow-up within 1–2 weeks of discharge with repeat echocardiography.
- Provide the patient with written warning signs of recurrence: increasing dyspnoea, chest pain, presyncope, palpitations, peripheral oedema.
- Advise the patient to present to the emergency department immediately if symptoms recur.
- For patients on NSAIDs/colchicine, schedule GP review at 2 and 6 weeks to assess response and monitor renal function.
Special Populations
Aboriginal and Torres Strait Islander Health Considerations
📚 References
- 1. Adler Y, Charron P, Imazio M, et al. 2015 ESC Guidelines for the diagnosis and management of pericardial diseases. Eur Heart J. 2015;36(42):2921–2964.
- 2. Spodick DH. Acute cardiac tamponade. N Engl J Med. 2003;349(7):684–690.
- 3. Imazio M, Adler Y. Management of pericardial effusion. Eur Heart J. 2013;34(16):1186–1197.
- 4. Klein AL, Abbara S, Agler DA, et al. American Society of Echocardiography clinical recommendations for multimodality cardiovascular imaging of patients with pericardial disease. J Am Soc Echocardiogr. 2013;26(9):965–1012.e15.
- 5. Tsang TSM, Enriquez-Sarano M, Freeman WK, et al. Consecutive 1127 therapeutic echocardiographically guided pericardiocenteses: clinical profile, practice patterns, and outcomes spanning 21 years. Mayo Clin Proc. 2002;77(5):429–436.
- 6. Rabindranath KS, Shrestha B, Papineni S, et al. Echocardiography-guided pericardiocentesis versus landmark-guided pericardiocentesis: a systematic review and meta-analysis. Int J Cardiol. 2017;228:729–735.
- 7. Australian Institute of Health and Welfare (AIHW). Tuberculosis notifications in Australia 2023. AIHW; 2024.
- 8. RHDAustralia (Rheumatic Heart Disease Australia). The 2020 Australian guideline for prevention, diagnosis and management of acute rheumatic fever and rheumatic heart disease. 3rd ed. Darwin: Menzies School of Health Research; 2020.
- 9. Maisch B, Seferović PM, Ristić AD, et al. Guidelines on the diagnosis and management of pericardial diseases. Eur Heart J. 2004;25(7):587–610.
- 10. Imazio M, Brucato A, Cemin R, et al. A randomized trial of colchicine for acute pericarditis (COPE trial). N Engl J Med. 2013;369(16):1522–1528.
- 11. ANZDATA Registry. 46th Annual Report 2023. Adelaide: Australia and New Zealand Dialysis and Transplant Registry; 2023.
- 12. Hancock EW. Cardiac tamponade. Med Clin North Am. 1979;63(1):223–237.
- 13. American Heart Association. Advanced Cardiovascular Life Support (ACLS) Provider Manual. Dallas: AHA; 2020.
- 14. Australian Commission on Safety and Quality in Health Care (ACSQHC). National Safety and Quality Health Service Standards. 2nd ed. Sydney: ACSQHC; 2021.
- 15. Willner DA, Goyal A, Grigorova Y, et al. Pericardiocentesis. In: StatPearls. Treasure Island (FL): StatPearls Publishing; 2024.