📋 Key Information Summary
- Atrial myxoma is the most common primary cardiac tumour, accounting for approximately 50% of all benign cardiac tumours in adults.
- Over 75% originate in the left atrium, classically attached to the interatrial septum at the fossa ovalis.
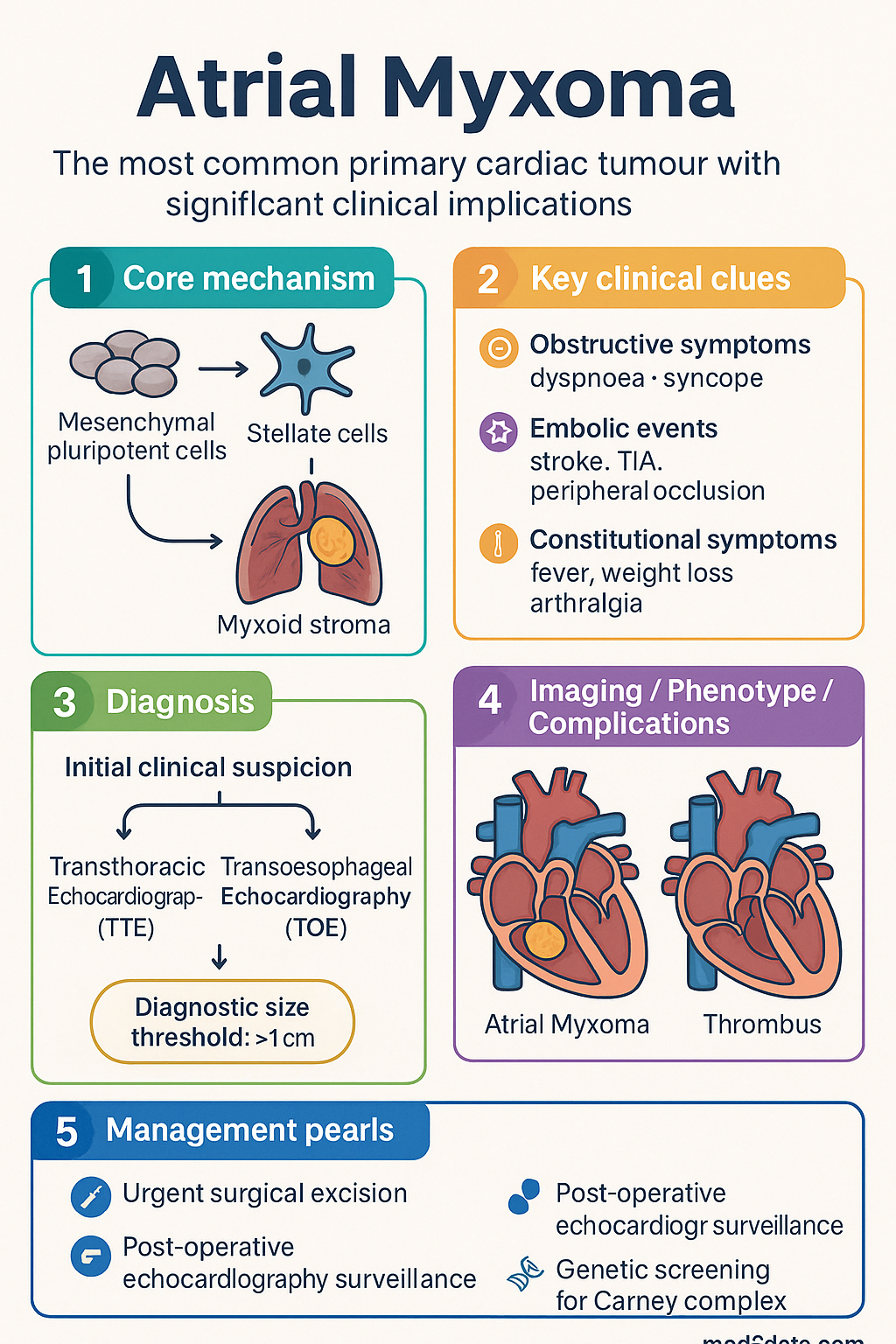
- Presentation follows a classic triad: 1) Obstructive symptoms (e.g., dyspnoea, syncope from mitral valve obstruction), 2) Embolic events (systemic or pulmonary), and 3) Constitutional symptoms (fever, weight loss, arthralgia).
- Transthoracic echocardiography (TTE) is the primary diagnostic investigation, with transoesophageal echocardiography (TOE) providing superior anatomical detail for surgical planning.
- Cardiac MRI is a valuable adjunct for tissue characterisation and assessing tumour extent, particularly in complex cases.
- The definitive treatment is urgent surgical excision via median sternotomy with cardiopulmonary bypass, regardless of tumour size or symptom severity.
- Surgery aims for complete resection with a cuff of surrounding atrial septum to minimise recurrence risk, which is low (approximately 1-3%) after complete excision.
- Post-operative surveillance with echocardiography is mandatory to monitor for recurrence, which can occur years later.
- In the Australian context, consider hereditary syndromes (e.g., Carney complex) in younger patients or those with multiple tumours, requiring genetic counselling and screening.
- Aboriginal and Torres Strait Islander patients may present later due to healthcare access barriers, leading to higher rates of complications from embolism or obstruction.
Introduction & Australian Epidemiology
Atrial myxoma is a benign primary cardiac neoplasm, representing the most common tumour of this type in the adult population. It is a clinically significant entity due to its strategic location within the heart, which can lead to life-threatening obstructive or embolic complications. In Australia, the incidence is estimated at 0.5-1 per million population per year, with a marked predilection for females (approximately 3:1 female-to-male ratio). The typical age of diagnosis is between the third and sixth decades of life, though hereditary forms associated with Carney complex may present earlier. While rare, the diagnosis must be considered in any patient presenting with unexplained embolic stroke, constitutional symptoms, or signs of intracardiac obstruction. Australian tertiary centres manage a steady caseload, with surgical outcomes being excellent.
Pathology & Location
Atrial myxomas are gelatinous, friable tumours that arise from the endocardial layer. Histologically, they consist of stellate cells embedded in a myxoid stroma rich in glycosaminoglycans.
Pathogenesis
The exact pathogenesis is debated, but it is believed to originate from mesenchymal pluripotent cells in the subendocardium (the so-called "reserve cells"). Most are sporadic. Approximately 7% are familial, often as part of the autosomal dominant Carney complex (associated with mutations in the PRKAR1A gene), featuring multiple myxomas, skin lentigines, and endocrine overactivity.
Anatomic Location
- Left Atrium (75-80%): The most common site. Over 90% of left atrial myxomas are attached to the interatrial septum at or near the fossa ovalis. They may also arise from the posterior wall, anterior wall, or, rarely, the mitral valve leaflets.
- Right Atrium (10-20%): Attached to the interatrial septum, free wall, or tricuspid valve.
- Ventricles (Rare): May occur in either ventricle, often attached to the free wall or papillary muscles.
Clinical Triad (Obstruction, Embolism, Constitutional)
Symptoms are highly variable and can mimic other cardiac or systemic illnesses. The classic triad occurs in a minority of patients but is highly suggestive when present.
Investigations (Echo, MRI)
First-Line Imaging
-
Essential
Transthoracic Echocardiography (TTE)The initial test of choice. Myxomas typically appear as a mobile, pedunculated, heterogeneous mass, often with a stalk attached to the interatrial septum. Doppler assesses haemodynamic obstruction. TTE is highly sensitive (>95%) for left atrial myxomas but may miss small tumours or those in the right atrium.
-
Essential
Transoesophageal Echocardiography (TOE)Provides superior spatial resolution, especially for assessing tumour attachment, extent, and composition. Crucial for surgical planning. TOE is also better for detecting small tumours, right-sided lesions, and associated valvular involvement. MBS item 55121 for diagnostic TOE.
Adjunctive Imaging
-
Available
Cardiac Magnetic Resonance Imaging (CMR)Gold standard for tissue characterisation. Demonstrates heterogeneous signal on T1/T2-weighted imaging and characteristic late gadolinium enhancement pattern. Excellent for differentiating myxoma from thrombus or other tumours, and for defining extent into adjacent structures. MBS item 63346.
-
Available
CT Angiography (CCTA)Useful if CMR is contraindicated. Provides excellent anatomical detail of tumour calcification and relationship to surrounding structures.
Laboratory & Other Tests
Full blood count (may show anaemia, elevated white cell count), inflammatory markers (ESR, CRP), troponin (if embolic coronary event). Genetic testing for PRKAR1A mutation is indicated if Carney complex is suspected. All patients should have an MRI/CT of the brain if embolic stroke is suspected.
Management (Surgical Excision)
Preoperative Management
- Hospital admission. Bed rest to minimise tumour embolisation risk.
- Treatment of heart failure with diuretics if required.
- Anticoagulation is NOT routinely indicated and may increase haemorrhagic transformation risk if embolic stroke has occurred. Manage per neurology/stroke guidelines.
- Urgent referral to a cardiothoracic surgical centre with expertise in cardiac tumours.
Definitive Therapy: Surgical Excision
Postoperative & Long-Term Management
- Postoperative TOE is performed to confirm complete excision.
- Lifelong surveillance echocardiography: annually for the first 5 years, then every 2–3 years, given recurrence risk (1–3%) and potential for delayed recurrence.
- Genetic screening for Carney complex: First-degree relatives of patients with familial myxoma or multiple tumours should be screened with echocardiography.
Special Populations
Pregnancy
Paediatrics
Aboriginal and Torres Strait Islander Peoples
ATSI Health Considerations
While atrial myxoma incidence is not known to be higher in Aboriginal and Torres Strait Islander populations, significant health disparities can affect outcomes.
📚 References
- 1. Reynen K. Cardiac myxomas. N Engl J Med. 1995;333(24):1610-7.
- 2. Pinede L, Duhaut P, Loire R. Clinical presentation of left atrial cardiac myxoma. A series of 112 consecutive cases. Medicine (Baltimore). 2001;80(3):159-72.
- 3. Carney JA. Differences between nonfamilial and familial cardiac myxoma. Am J Surg Pathol. 1985;9(1):53-5.
- 4. Grebenc ML, Rosado de Christenson ML, Burke AP, Green CE, Galvin JR. Primary cardiac and pericardial neoplasms: radiologic-pathologic correlation. Radiographics. 2000;20(4):1073-103.
- 5. Bruce CJ. Cardiac tumours: diagnosis and management. Heart. 2011;97(2):151-60.
- 6. Motwani M, et al. MR imaging of cardiac tumors and masses: a review of methods and clinical applications. Radiology. 2013;268(1):26-43.
- 7. Sellke FW, del Nido PJ, Swanson SJ, eds. Sabiston & Spencer Surgery of the Chest. 9th ed. Elsevier; 2016. Chapter 102: Cardiac Tumors.
- 8. Australian Institute of Health and Welfare (AIHW). Cardiovascular disease in Aboriginal and Torres Strait Islander people. Cat. no. CVD 83. Canberra: AIHW; 2022.
- 9. Heart Foundation of Australia. Guidelines for the management of absolute cardiovascular disease risk. 2023.
- 10. National Heart Foundation of Australia and the Cardiac Society of Australia and New Zealand. Position statement on coronary artery calcium scoring for cardiovascular risk assessment. Med J Aust. 2022;217(4):187-93.