📋 Key Information Summary
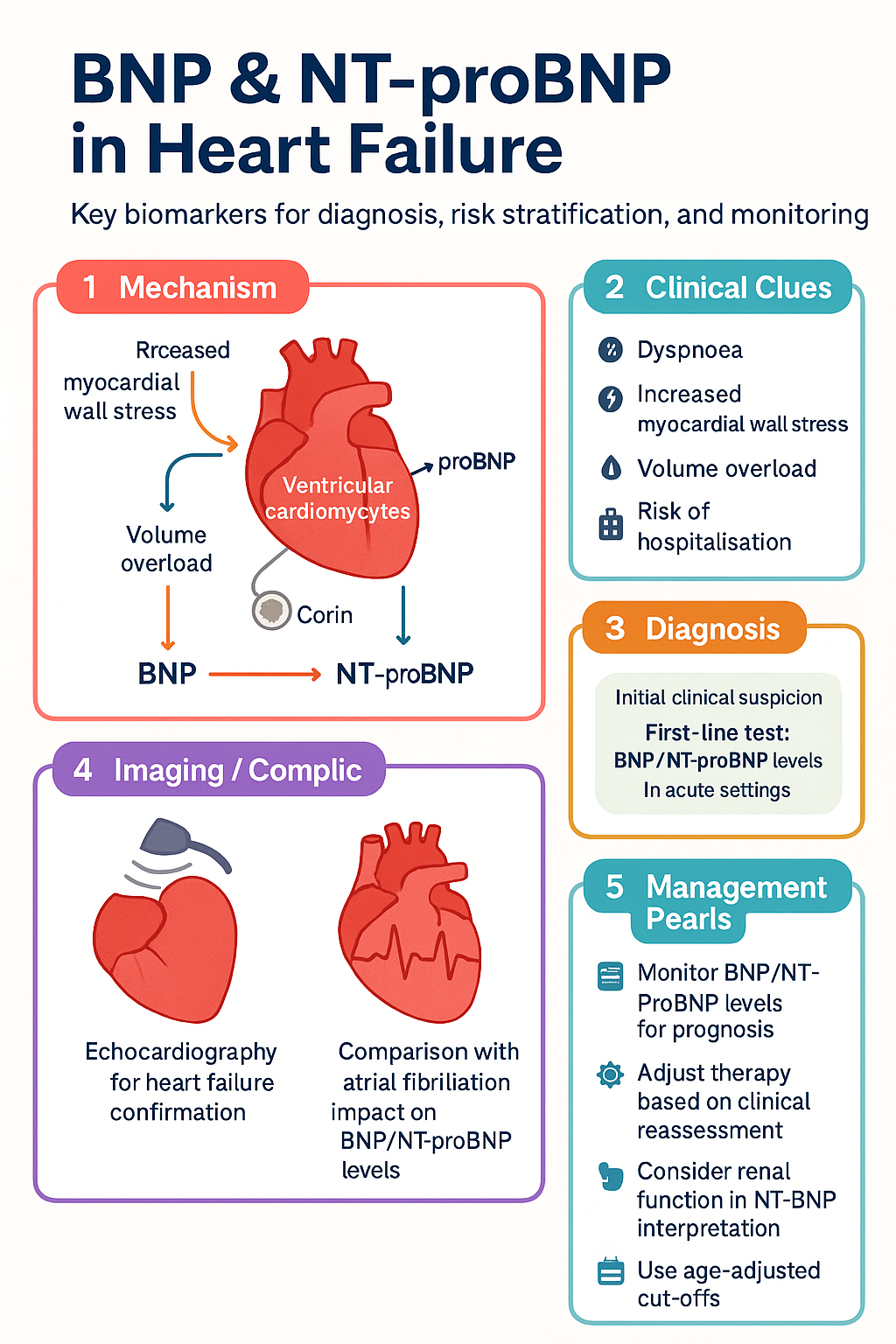
- BNP and NT-proBNP are released from ventricular cardiomyocytes in response to increased myocardial wall stress and volume overload.
- They are first-line biomarkers for diagnosing or excluding heart failure (HF) in patients presenting with dyspnoea.
- In the acute setting, a BNP <100 pg/mL or NT-proBNP <300 pg/mL has a high negative predictive value for excluding acute HF.
- For chronic HF in the community, lower diagnostic thresholds apply (e.g., BNP <35 pg/mL or NT-proBNP <125 pg/mL) to rule out HF.
- Elevated levels correlate with HF severity, prognosis, and risk of hospitalisation or death.
- Serial measurement can guide therapy in selected patients, though routine use for titration is not universally recommended.
- Levels are influenced by age, sex, renal function, and obesity—interpretation must be context-dependent.
- NT-proBNP has a longer half-life and is more affected by renal impairment than BNP.
- Both assays are widely available in Australia (MBS rebate applies) and results are typically available within 1-2 hours.
- A normal natriuretic peptide level makes a diagnosis of symptomatic HF very unlikely, but an elevated level requires echocardiographic confirmation.
Introduction & Australian Epidemiology
B-type natriuretic peptide (BNP) and its inactive N-terminal fragment (NT-proBNP) are cardiac biomarkers released primarily by ventricular cardiomyocytes in response to increased wall stress, pressure, or volume overload. They play a pivotal role in the diagnosis, risk stratification, and monitoring of heart failure (HF).
In Australia, HF affects an estimated 500,000 people, with prevalence increasing sharply with age. It is a leading cause of hospitalisation, particularly in patients over 65 years. The availability of rapid, standardised assays for BNP and NT-proBNP has transformed the assessment of patients with suspected HF, enabling faster triage in emergency departments and more objective assessment in primary care. Understanding their physiology, appropriate diagnostic thresholds, and limitations is essential for optimal patient management.
Physiology & Release
BNP is synthesised as a pre-prohormone (proBNP1-108) in ventricular cardiomyocytes. In response to increased myocardial stretch, proBNP is cleaved by the enzyme corin into the active 32-amino acid hormone BNP (BNP-32) and the biologically inactive 76-amino acid N-terminal fragment (NT-proBNP).
- BNP: Has a short half-life (~20 minutes). It exerts natriuretic, diuretic, and vasodilatory effects, acting as a physiological counter-regulator to the renin-angiotensin-aldosterone system (RAAS) and sympathetic nervous system.
- NT-proBNP: Has a longer half-life (~120 minutes) and is cleared renally. This leads to higher circulating levels and a greater influence of renal function on its concentration.
Diagnostic Cut-offs (Acute vs Chronic HF)
Diagnostic thresholds differ significantly between acute and chronic presentations. Using the correct cut-off is critical to avoid misdiagnosis.
| Clinical Setting | BNP (pg/mL) | NT-proBNP (pg/mL) | Interpretation |
|---|---|---|---|
| Acute Dyspnoea / ED | Rule-out: <100 Grey zone: 100-500 Rule-in: >500 | Rule-out: <300 Grey zone: 300-1800 (age-adjusted recommended)* Rule-in: >1800 (age <50) >2200 (age 50-75) >4500 (age >75) | High NPVs for rule-out. Age-adjusted NT-proBNP cut-offs improve specificity. |
| Chronic / Community (Primary Care) | Rule-out: <35 Indeterminate: 35-500 Suggestive: >500 | Rule-out: <125 (all ages) Indeterminate: 125-1000 Suggestive: >1000 | Lower thresholds used. A normal level makes symptomatic HF unlikely. |
Prognostic Value & Monitoring
Beyond diagnosis, natriuretic peptides are powerful prognostic markers. A single measurement at discharge or follow-up, or a change in level over time, independently predicts outcomes.
Prognostication
- Higher pre-discharge BNP/NT-proBNP levels are associated with increased risk of 30-day to 1-year mortality and rehospitalisation.
- In chronic HF, stable but elevated levels indicate worse prognosis compared to those who achieve a significant reduction with therapy.
Monitoring Therapy
The role of serial natriuretic peptide measurement to guide HF therapy (NT-proBNP-guided therapy) remains an area of active research.
Limitations & Confounders
BNP and NT-proBNP are not specific for HF. Several conditions can cause elevated levels, and others can cause falsely low levels. Interpretation requires careful clinical correlation.
| Confounder | Effect on BNP/NT-proBNP | Clinical Implication |
|---|---|---|
| Obesity (BMI ≥30 kg/m²) | Falsely low levels (especially NT-proBNP) | A "normal" level in an obese patient with high clinical suspicion does not exclude HF. Consider a lower threshold for echocardiography. |
| Renal Impairment (eGFR <60 mL/min) | Markedly elevated NT-proBNP; mildly elevated BNP | Use higher NT-proBNP cut-offs (e.g., >1200 pg/mL in acute setting) or prefer BNP. Always adjust for renal function. |
| Atrial Fibrillation | Elevated levels | Reduces specificity. An elevated level in AF is less discriminative for LV dysfunction. |
| Age >75 years | Elevated levels (especially NT-proBNP) | Use age-adjusted cut-offs as per table above. |
| Acute Coronary Syndromes | Elevated levels due to myocardial ischaemia/stress | Not diagnostic for HF in isolation; indicates myocardial injury and higher risk. |
| Right Heart Strain (e.g., massive PE, pulmonary hypertension) | Elevated levels | Reflects RV pressure overload, not necessarily left-sided failure. |
| Cardiac Amyloid, Constrictive Pericarditis | Elevated levels | Useful for monitoring, but not specific for HFpEF/HFrEF. |
| "Dry" or Compensated State | Levels may be normal or near-normal | A normal level does not exclude a history of HF; it reflects current volume status. |
Aboriginal and Torres Strait Islander Health
📚 References
- 1. National Heart Foundation of Australia and Cardiac Society of Australia and New Zealand. Australian Clinical Guidelines for the Management of Heart Failure. 2023 Update.
- 2. McDonagh TA, Metra M, Adamo M, et al. 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure. Eur Heart J. 2021;42(36):3599-3726.
- 3. Januzzi JL, Chen-Tournoux AA, Moe G. Amino-terminal pro-B-type natriuretic peptide testing for the diagnosis or exclusion of heart failure in patients with acute symptoms. Am J Cardiol. 2008;101(3A):29-38.
- 4. Troughton RW, Frampton CM, Brunner-La Rocca HP, et al. Effect of B-type natriuretic peptide-guided treatment of chronic heart failure on total mortality and hospitalization: an individual patient meta-analysis. Eur Heart J. 2014;35(23):1559-67.
- 5. Australian Institute of Health and Welfare (AIHW). Heart, stroke and vascular disease—Australian facts. AIHW, Canberra. 2023.
- 6. Daniels LB, Bhalla V, Clopton P, et al. B-type natriuretic peptide (BNP) levels and ethnic disparities in perceived severity of heart failure: results from the Rapid Emergency Department Heart Failure Outpatient Trial (REDHOT) multicenter study. J Card Fail. 2006;12(5):361-7.
- 7. Richards AM, Nicholls MG, Yandle TG, et al. Plasma N-terminal pro-brain natriuretic peptide and adrenomedullin: new neurohormonal predictors of left ventricular function and prognosis after myocardial infarction. Circulation. 1998;97(19):1921-9.
- 8. Maisel AS, Krishnaswamy P, Nowak RM, et al. Rapid measurement of B-type natriuretic peptide in the emergency diagnosis of heart failure. N Engl J Med. 2002;347(3):161-7.
- 9. Bhalla V, Willis S, Maisel A. B-type natriuretic peptide: the level and the drug--partners in the diagnosis of congestive heart failure. Congest Heart Fail. 2004;10(1 Suppl 1):3-14.
- 10. Medical Services Advisory Committee (MSAC). Application No. 1198. Assessment of B-type natriuretic peptide (BNP) or N-terminal proBNP for the diagnosis of heart failure. Australian Government Department of Health. 2015.
- 11. RHDAustralia (ARF/RHD writing group). The 2020 Australian guideline for prevention, diagnosis and management of acute rheumatic fever and rheumatic heart disease. 3rd edn. Menzies School of Health Research, Darwin. 2020.