📋 Key Information Summary
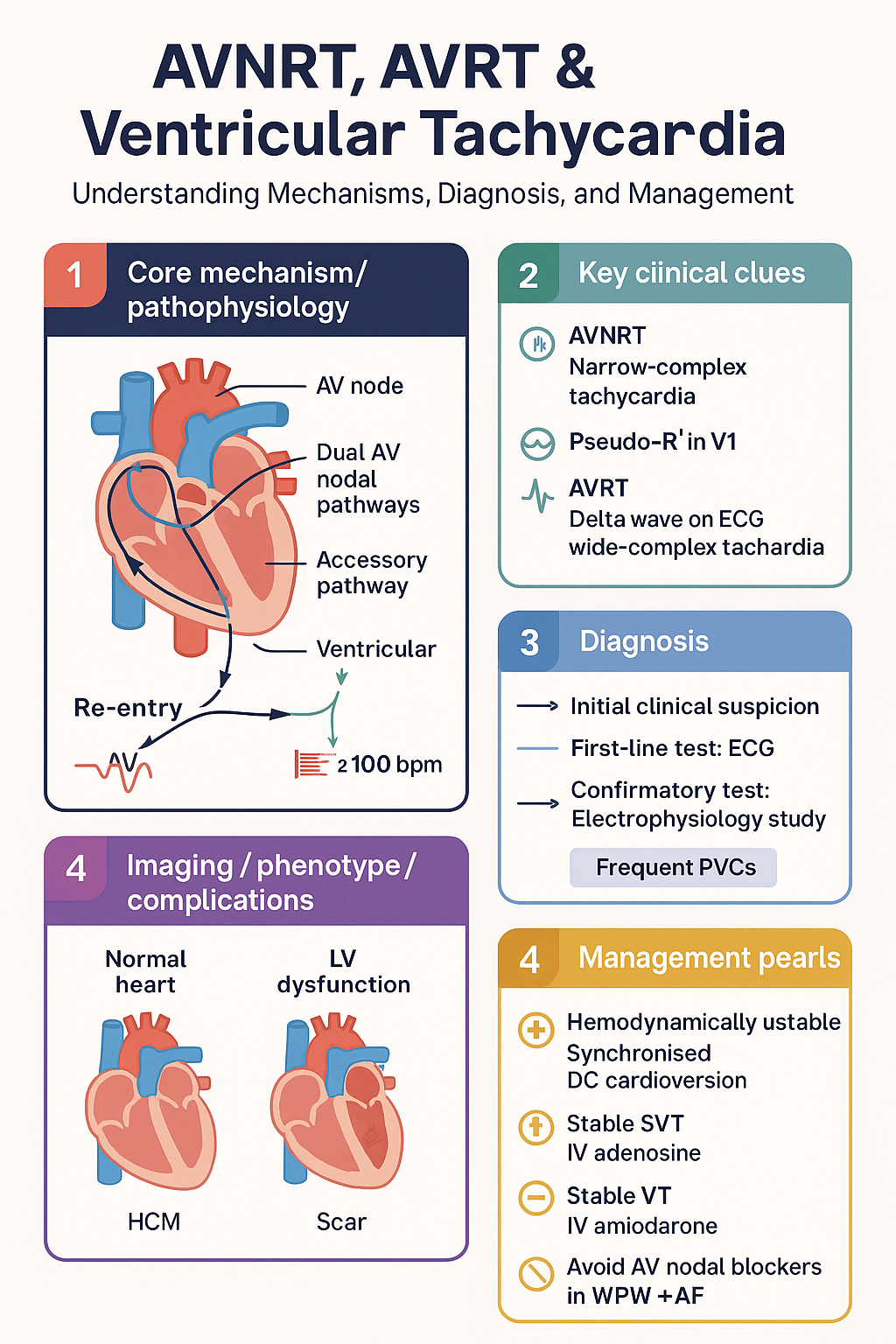
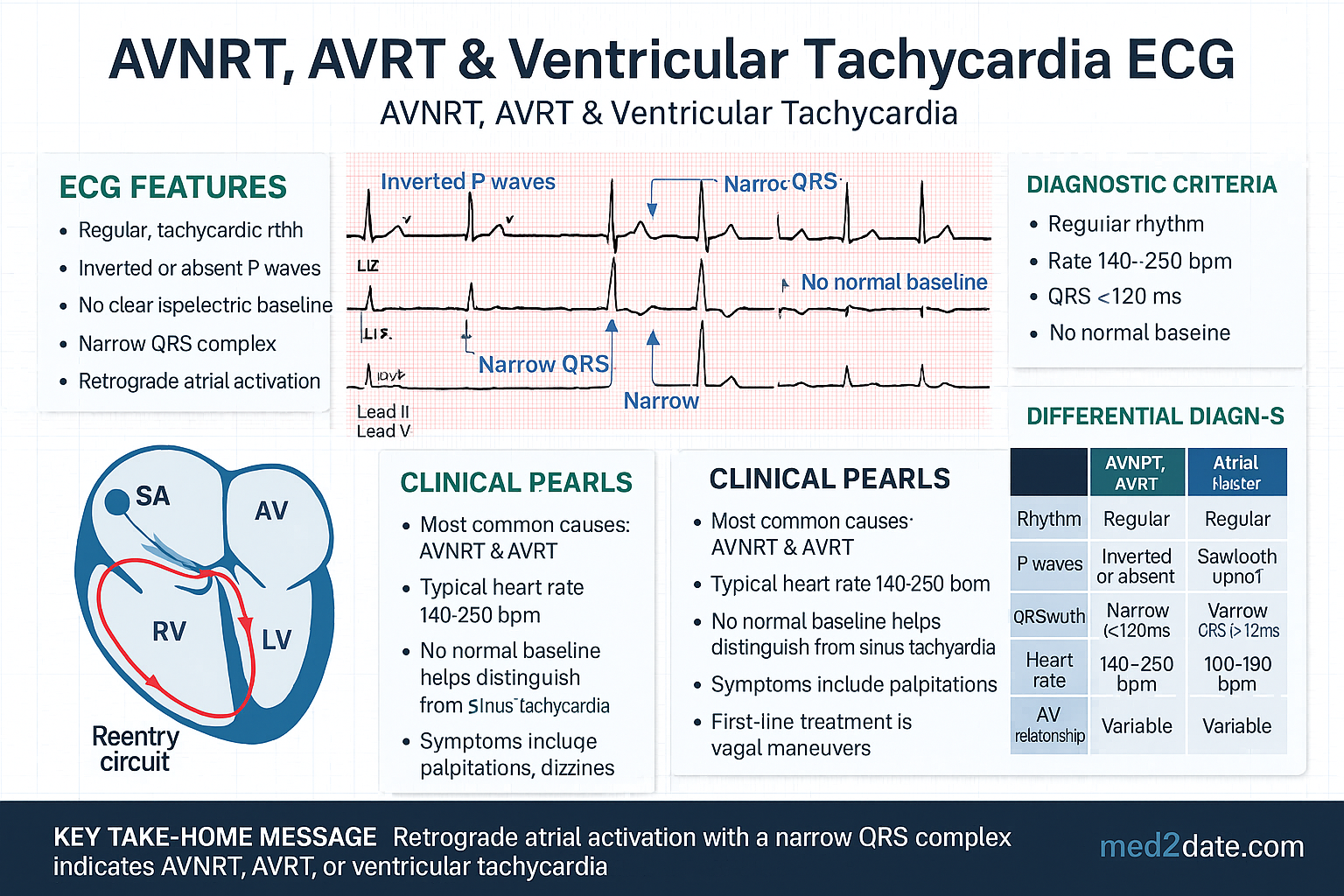
- AVNRT is the most common paroxysmal SVT — re-entry via dual AV nodal pathways; narrow-complex tachycardia ~150–250 bpm with pseudo-R′ in V1 and pseudo-S in inferior leads.
- AVRT (WPW syndrome) uses an accessory pathway — delta wave on resting ECG in pre-excitation; antidromic AVRT produces wide-complex tachycardia mimicking VT.
- Ventricular tachycardia (VT) originates below the His bundle; defined as ≥3 consecutive ventricular beats at rate ≥100 bpm; always assume VT in wide-complex tachycardia until proven otherwise.
- Haemodynamically unstable SVT/VT → synchronised DC cardioversion immediately (start at 120–150 J biphasic).
- Stable narrow-complex SVT → IV adenosine 6 mg rapid IV push → 12 mg → 12 mg as first-line diagnostic and therapeutic agent.
- Stable VT → IV amiodarone 300 mg over 20–60 min (or procainamide if structurally normal heart).
- ⚠️ AVNODAL blockers are CONTRAINDICATED in pre-excited AF (WPW + AF) — adenosine, verapamil, diltiazem, beta-blockers, digoxin can precipitate ventricular fibrillation and death.
- WPW + AF → procainamide IV or synchronised cardioversion; treat as VT-equivalent.
- ECG differentiation of SVT with aberrancy vs VT: favour VT if any of — capture beats, fusion beats, AV dissociation, extreme axis deviation, concordance in all precordial leads, QRS >160 ms.
- Catheter ablation is first-line long-term therapy for recurrent AVNRT, AVRT/WPW, and idiopathic VT with success rates >95% in Australian tertiary centres.
- Sustained monomorphic VT in structurally normal heart (RVOT, fascicular VT) — generally favourable prognosis; verapamil-sensitive fascicular VT responds to verapamil but NOT adenosine.
- Structural heart disease VT (ischaemic, dilated cardiomyopathy) — high risk of SCD; ICD indicated per NHFA/CSANZ guidelines if LVEF ≤35% despite ≥3 months optimal medical therapy.
- Pregnancy — adenosine remains first-line for haemodynamically stable SVT; avoid amiodarone (foetal thyroid toxicity); DC cardioversion safe in all trimesters.
- ATSI populations — higher prevalence of rheumatic heart disease predisposing to arrhythmias; reduced access to EP studies and ablation in remote communities; culturally safe pathways essential.
Introduction & Australian Epidemiology
Supraventricular tachycardias (SVTs) encompass a group of arrhythmias originating at or above the atrioventricular (AV) junction. Atrioventricular nodal re-entrant tachycardia (AVNRT) and atrioventricular re-entrant tachycardia (AVRT), including Wolff–Parkinson–White (WPW) syndrome, are the two most common paroxysmal SVTs encountered in Australian emergency departments and general practice. Ventricular tachycardia (VT) originates below the His bundle and carries a substantially higher risk of haemodynamic compromise, syncope, and sudden cardiac death (SCD).
In Australia, SVTs account for approximately 2–3 per 1,000 population, with AVNRT representing roughly 60% of paroxysmal SVTs and AVRT approximately 30%. VT incidence is estimated at 5–10 per 100,000 population per year, with the majority occurring in the context of structural heart disease — particularly ischaemic cardiomyopathy and dilated cardiomyopathy. Idiopathic VT in structurally normal hearts accounts for approximately 10% of all VT presentations.
Australian data from the AIHW National Hospital Morbidity Database indicate that arrhythmia-related admissions have increased by approximately 20% over the past decade, driven by improved detection (wearable monitors, implantable loop recorders) and an ageing population. The NHFA/CSANZ 2024 guidelines for the management of arrhythmias in Australia provide the framework for diagnosis and treatment discussed in this article.
AVNRT: Mechanism & ECG
Re-entrant Circuit
AVNRT is caused by re-entry within the AV node between two functionally distinct pathways:
- Slow pathway — inferior-posterior AV node input (compact node to coronary sinus ostium region); shorter refractory period, slow conduction velocity.
- Fast pathway — superior-anterior AV node input (compact node to Todaro tendon region); longer refractory period, fast conduction velocity.
Typical (Slow–Fast) AVNRT — ~90% of cases
Anterograde conduction via the slow pathway → retrograde conduction via the fast pathway. The P wave is buried within or immediately following the QRS complex (RP interval <70 ms). On ECG:
- Rate: 150–250 bpm (commonly 180–200 bpm).
- Narrow QRS complex (unless pre-existing bundle branch block or rate-related aberrancy).
- Pseudo-R′ wave in lead V1 (retrograde P distorting terminal QRS).
- Pseudo-S wave in leads II, III, aVF.
- No visible isoelectric segment between QRS and retrograde P.
Atypical (Fast–Slow) AVNRT — ~5–10%
Anterograde via fast pathway → retrograde via slow pathway. Produces a long RP tachycardia (RP interval > PR interval). P wave visible in early diastole — may be confused with atrial tachycardia or PJRT (permanent junctional reciprocating tachycardia).
ECG Recognition Checklist
| Feature | Typical AVNRT | Atypical AVNRT |
|---|---|---|
| Circuit | Slow anterograde, fast retrograde | Fast anterograde, slow retrograde |
| RP interval | <70 ms (P buried/follows QRS) | >PR interval (long RP) |
| P-wave morphology | Pseudo-R′ V1; pseudo-S II/III/aVF | Negative P in II, III, aVF; positive in V1 |
| Prevalence | ~90% | ~5–10% |
| Adenosine response | Terminates | Terminates (may require higher dose) |
AVRT & WPW Syndrome
Anatomy of the Accessory Pathway
AVRT requires a structural accessory pathway (AP) — most commonly a free-wall or septal Kent bundle — providing a second conducting route between atria and ventricles separate from the AV node–His–Purkinje system. The AP may be:
- Manifest — conducts anterograde, producing pre-excitation (delta wave) on baseline ECG. The combination of a manifest AP + documented tachycardia = WPW syndrome.
- Concealed — conducts only retrograde; no delta wave at baseline; can still support orthodromic AVRT.
Orthodromic AVRT (~95% of AVRT)
Anterograde conduction via AV node → retrograde via AP. Produces a narrow-complex tachycardia with visible retrograde P wave (RP interval 70–90 ms, shorter than PR). The delta wave is absent during tachycardia because anterograde ventricular activation occurs through the normal conduction system.
Antidromic AVRT (~5%)
Anterograde via AP → retrograde via AV node. Produces a wide-complex tachycardia — maximally pre-excited QRS — which may be indistinguishable from VT on surface ECG. The rate is typically 200–300 bpm.
Pre-excitation ECG Features (Baseline)
- Short PR interval (<120 ms) — due to AV bypass conduction.
- Delta wave — slurred upstroke of QRS onset, widening the QRS to >110 ms.
- Secondary ST-T wave changes — discordant to the major QRS vector.
- Pathway localisation inferred from delta-wave polarity across precordial and limb leads (Arruda algorithm).
If a patient with WPW develops AF, conduction down the AP can produce ventricular rates exceeding 300 bpm with haemodynamic collapse → VF → cardiac arrest. AV nodal blockers are CONTRAINDICATED — adenosine, verapamil, diltiazem, beta-blockers, and digoxin all block the AV node, forcing all conduction through the AP and accelerating the ventricular response. Treatment: IV procainamide 15–18 mg/kg (max 50 mg/min) or synchronised DC cardioversion.
WPW + AF — ECG Recognition
- Irregularly irregular wide-complex tachycardia.
- Variable QRS morphology (fusion of AP and normal conduction).
- Very fast rate (often >220 bpm).
- Shortest pre-excited RR interval <250 ms = high risk of degeneration to VF.
Risk Stratification in WPW
Ventricular Tachycardia: Classification & ECG
Definition
Ventricular tachycardia is defined as ≥3 consecutive ventricular complexes at a rate ≥100 bpm. VT lasting <30 seconds that self-terminates is classified as non-sustained VT (NSVT); VT persisting ≥30 seconds or requiring intervention due to haemodynamic compromise is sustained VT.
Classification by Morphology
| Type | Morphology | Common Aetiology | Prognosis |
|---|---|---|---|
| Monomorphic VT | Constant QRS morphology beat-to-beat | Scar-related (ischaemic CM, DCM), RVOT-VT, fascicular VT | Variable — depends on structure |
| Polymorphic VT | Changing QRS axis/amplitude | Acute ischaemia, long QT, Brugada, catecholaminergic PMVT | High risk of degeneration to VF |
| Torsades de Pointes | Polymorphic VT with QTc prolongation | Drug-induced (sotalol, amiodarone, erythromycin), hypokalaemia, congenital LQTS | Self-terminating or degenerates to VF |
| Ventricular Fibrillation | Chaotic, no organised QRS | Ischaemia, electrical, commotio cordis | Immediate cardiac arrest |
Classification by Substrate
- Post-myocardial infarction scar (re-entrant circuit around dense scar + border zone).
- Dilated cardiomyopathy (epicardial/mid-myocardial scar).
- Arrhythmogenic right ventricular cardiomyopathy (ARVC) — fat/fibro-fatty replacement of RV.
- Hypertrophic cardiomyopathy.
- Valvular heart disease, congenital heart disease post-repair.
- RVOT VT — cAMP-mediated triggered activity; LBBB morphology, inferior axis; responds to adenosine, verapamil, beta-blockers.
- Fascicular VT (Belhassen VT) — re-entry within Purkinje network; RBBB + left axis (posterior fascicular); verapamil-sensitive.
- Outflow tract VT from LV — RBBB, inferior axis.
- LV summit / aortic cusp VT.
ECG Criteria: VT vs SVT with Aberrancy
In wide-complex tachycardia, assume VT until proven otherwise. Misdiagnosis of VT as SVT with aberrancy and treatment with AV nodal blockers can be fatal. The Brugada algorithm and Vereckei criteria provide systematic ECG differentiation:
| Criterion Favours VT | Sensitivity | Specificity |
|---|---|---|
| Absence of RS in all precordial leads (Brugada step 1) | 21% | 100% |
| RS interval >100 ms in any precordial lead (Brugada step 2) | 82% | 98% |
| AV dissociation (Brugada step 3) | 82% | 98% |
| Morphology criteria in V1/V6 (Brugada step 4) | 99% | 97% |
| Extreme axis deviation (northwest axis) | ~20% | ~95% |
| Concordance (all +ve or all −ve) across precordial leads | ~20% | ~95% |
| Capture beats / Fusion beats | ~5–10% | ~100% |
| QRS duration >160 ms (if LBBB pattern) or >140 ms (if RBBB pattern) | Variable | Variable |
Specific VT ECG Patterns
| VT Origin | ECG Pattern | Treatment Sensitivity |
|---|---|---|
| RVOT | LBBB + inferior axis (positive II, III, aVF) | Adenosine, verapamil, beta-blockers; ablation >90% |
| Posterior fascicular | RBBB + left axis deviation | Verapamil IV 5–10 mg; ablation >95% |
| Anterior fascicular | RBBB + right axis deviation | Verapamil; ablation |
| LV summit / aortic cusp | RBBB or LBBB; transition V1–V2 | Ablation from aortic root |
| Scar-related (ischaemic) | Variable; RBBB or LBBB; often monomorphic | Amiodarone; ICD; substrate ablation |
Acute Management
Universal First Step: Assess Haemodynamic Stability
At presentation, determine whether the patient is haemodynamically stable (conscious, talking, SBP >90 mmHg, no pulmonary oedema, no ongoing chest pain) or unstable (altered consciousness, hypotension, pulmonary oedema, ischaemic chest pain). This determines the immediate treatment pathway.
Stable SVT (AVNRT / Orthodromic AVRT) — Acute Termination
Pre-excited AF / Antidromic AVRT (WPW + AF)
Stable VT — Acute Management
Torsades de Pointes — Specific Management
Long-term Treatment
AVNRT — Long-term Strategies
AVRT / WPW — Long-term Strategies
- Catheter ablation of accessory pathway — first-line for all symptomatic WPW and for high-risk asymptomatic WPW (short AP refractory period, pre-excited AF). Success rate: left lateral pathways >97%, septal pathways 90–95%, right free-wall 88–93%. Risk of AV block for septal pathways (para-Hisian). MBS Item 38286.
- Pill-in-the-pocket (flecainide 200–300 mg single oral dose for self-terminating AVRT episodes) — only after in-hospital observation of first dose and ECG confirmation of safe termination. Not suitable for pre-excited AF.
- Medical therapy — if ablation declined or not feasible: flecainide (no structural heart disease) or sotalol. AV nodal blockers alone are insufficient as they do not block the AP.
VT — Long-term Strategies
Implantable Cardioverter-Defibrillator (ICD)
Indications per NHFA/CSANZ 2024:
- Secondary prevention — survivors of cardiac arrest due to VT/VF (without reversible cause), sustained VT with syncope or haemodynamic compromise, or VT with LVEF ≤35%. ICD is strongly recommended.
- Primary prevention — LVEF ≤35% despite ≥3 months of optimal guideline-directed medical therapy (GDMT) in ischaemic cardiomyopathy (post-MI ≥40 days) or non-ischaemic DCM. NYHA II–III. (MADIT-II, SCD-HeFT trials).
- Subcutaneous ICD (S-ICD) — preferred in younger patients, those requiring MRI, or with limited venous access. No anti-bradycardia pacing capability.
VT Ablation
- Idiopathic VT — curative (RVOT VT, fascicular VT): success >90%, low recurrence.
- Scar-related VT — substrate modification to reduce VT burden and ICD shocks. Success 50–70% freedom from VT at 1 year. Consider early referral if ≥1 appropriate ICD shock despite amiodarone, or recurrent VT episodes requiring hospitalisation.
- VT storm (≥3 VT episodes in 24 h) — IV amiodarone + sedation (propofol/midazolam) + catheter ablation or sympathetic denervation (left cardiac sympathetic denervation, stellate ganglion block).
Quick Reference: Long-term Therapy Selection
Special Populations
Aboriginal and Torres Strait Islander Health Considerations
📚 References
- 1. Brieger DB, Chow CK, Gao L, et al. Australian Institute of Health and Welfare. Cardiovascular disease — Australian facts. AIHW Cat. no. CVD 87. Canberra: AIHW; 2023.
- 2. National Heart Foundation of Australia and Cardiac Society of Australia and New Zealand (NHFA/CSANZ). Australian clinical guidelines for the diagnosis and management of arrhythmias. Heart Lung Circ. 2024;33(1):e1–e98.
- 3. Page RL, Joglar JA, Caldwell MA, et al. 2015 ACC/AHA/HRS guideline for the management of adult patients with supraventricular tachycardia. J Am Coll Cardiol. 2016;67(13):e27–e115.
- 4. Al-Khatib SM, Stevenson WG, Ackerman MJ, et al. 2017 AHA/ACC/HRS guideline for management of patients with ventricular arrhythmias and the prevention of sudden cardiac death. Circulation. 2018;138(13):e272–e391.
- 5. Appelboam A, Reuben A, Mann C, et al. Postural modification to the standard Valsalva manoeuvre for emergency treatment of supraventricular tachycardias (REVERT): a randomised controlled trial. Lancet. 2015;386(10005):1747–1753.
- 6. Brugada P, Brugada J, Mont L, et al. A new approach to the differential diagnosis of a regular tachycardia with a wide QRS complex. Circulation. 1991;83(5):1649–1659.
- 7. Echt DS, Liebson PR, Mitchell LB, et al. Mortality and morbidity in patients receiving encainide, flecainide, or placebo: the Cardiac Arrhythmia Suppression Trial. N Engl J Med. 1991;324(12):781–788.
- 8. Bardy GH, Lee KL, Mark DB, et al. Amiodarone or an implantable cardioverter-defibrillator for congestive heart failure (SCD-HeFT). N Engl J Med. 2005;352(3):225–237.
- 9. Moss AJ, Zareba W, Hall WJ, et al. Prophylactic implantation of a defibrillator in patients with myocardial infarction and reduced ejection fraction (MADIT-II). N Engl J Med. 2002;346(12):877–883.
- 10. RHDAustralia (a program of Menzies School of Health Research). The 2020 Australian guideline for prevention, diagnosis and management of acute rheumatic fever and rheumatic heart disease (3rd edition). Darwin: RHDAustralia; 2020.
- 11. Cronin EM, Bogun FM, Maury P, et al. 2019 HRS/EHRA/APHRS/LAHRS expert consensus statement on catheter ablation of ventricular arrhythmias. Heart Rhythm. 2020;17(1):e2–e154.
- 12. Australian Commission on Safety and Quality in Health Care (ACSQHC). National Safety and Quality Health Service Standards. 2nd ed. Sydney: ACSQHC; 2021.
- 13. AIHW. Aboriginal and Torres Strait Islander health performance framework 2020 summary report. Cat. no. IHPF 2. Canberra: AIHW; 2020.