📋 Key Information Summary
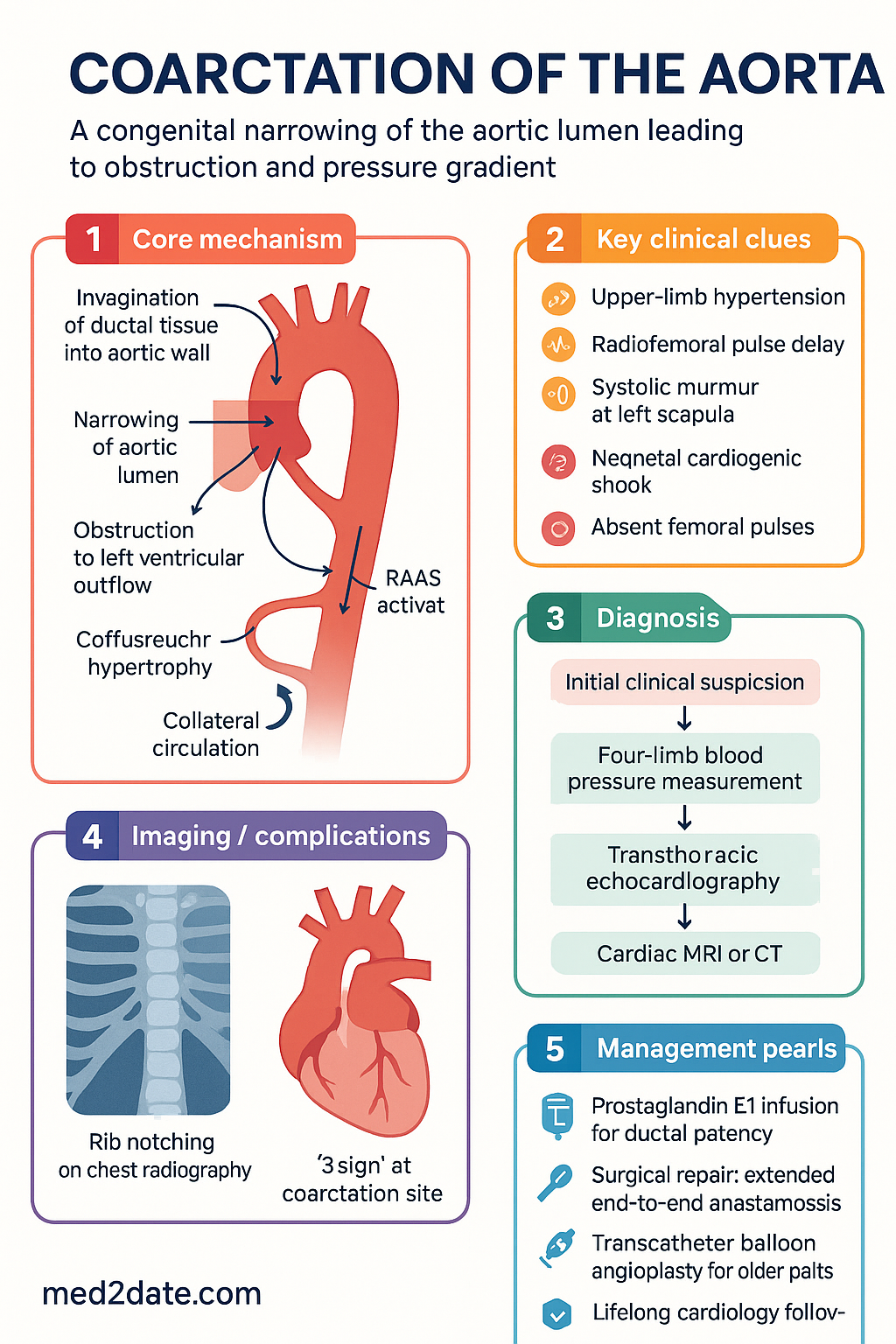
- Definition: Coarctation of the aorta (CoA) is a discrete narrowing of the aortic lumen, most commonly at the isthmus (junction of the ductus arteriosus and the aorta), producing an obstruction to left ventricular outflow and a pressure gradient between the upper and lower body.
- Epidemiology: Accounts for approximately 5–8 % of all congenital heart defects in Australia; male-to-female ratio ≈ 2:1 (excluding Turner syndrome); incidence ~3–4 per 10,000 live births.
- Key associations: Bicuspid aortic valve (BAV) in 50–85 % of cases; Turner syndrome (45,X) in ~10–15 %; Berry (intracranial) aneurysm; patent ductus arteriosus; ventricular septal defect.
- Classical triad: Upper-limb hypertension, radiofemoral pulse delay, and systolic murmur loudest at the left scapular region.
- Critical neonatal presentation: Duct-dependent CoA presenting with cardiogenic shock, acidosis, and absent femoral pulses when the ductus arteriosus closes — a surgical emergency.
- Diagnosis: Transthoracic echocardiography (TTE) as first-line; cardiac MRI is the gold-standard for anatomical delineation in adolescents and adults; CT angiography when MRI is contraindicated.
- Haemodynamic criterion: Peak systolic gradient ≥ 20 mmHg across the coarctation site by Doppler or catheter is generally considered significant.
- Treatment options: Surgical repair (extended end-to-end anastomosis preferred in neonates and infants); transcatheter balloon angioplasty (± bare-metal stent) for older children, adolescents, and adults with recurrent or native coarctation.
- Prognosis without repair: Median age at death ~35 years due to complications including refractory hypertension, aortic dissection/rupture, intracranial aneurysm haemorrhage, coronary artery disease, and heart failure.
- Lifelong surveillance: All repaired patients require ongoing cardiology follow-up; hypertension persists in 25–70 % post-repair and requires pharmacotherapy; imaging every 5 years (MRI preferred) to monitor for re-coarctation and aortic root dilation.
- ATSI considerations: Higher rates of delayed diagnosis in remote communities; echocardiographic screening in infants with upper-limb hypertension or pulse abnormalities; culturally safe pathways through Aboriginal Medical Services.
Introduction & Australian Epidemiology
Coarctation of the aorta (CoA) is a congenital narrowing, typically located at the aortic isthmus distal to the origin of the left subclavian artery, at or near the former insertion of the ductus arteriosus. This obstruction imposes a pressure load on the left ventricle and produces a pressure gradient between the upper and lower extremities. The condition is classified by timing of presentation — neonatal (duct-dependent, critical) versus infantile (re-coarctation or late-diagnosed) versus adult (often previously undiagnosed or with residual gradient post-repair).
In Australia, CoA represents 5–8 % of all congenital heart disease, with an estimated incidence of 3–4 per 10,000 live births. The Australian Paediatric Cardiac Registry and AIHW congenital anomaly data confirm a male predominance (≈ 2:1) outside Turner syndrome. Newborn pulse-oximetry screening programmes have improved early detection of duct-dependent lesions, though isolated CoA without significant shunting may still present late with hypertension or exercise intolerance.
The Australasian Society of Cardiac and Thoracic Surgeons (ASCTS) database shows excellent outcomes for neonatal repair at Australian paediatric cardiac centres (Royal Children's Hospital Melbourne, Westmead Children's Hospital Sydney, Queensland Children's Hospital Brisbane), with operative mortality < 1 % for elective extended end-to-end anastomosis. Late complications — including re-coarctation, persistent hypertension, aortic root dilation, and Berry aneurysm — necessitate structured lifelong follow-up.
Pathophysiology & Associations
Anatomical Basis
Coarctation results from invagination of the ductal (juxtaductal) tissue into the aortic wall during perinatal life, forming a discrete posterior shelf that narrows the aortic lumen. Less commonly, tubular hypoplasia of the aortic arch or a long-segment narrowing occurs, particularly in neonates with complex intracardiac lesions.
Haemodynamic Consequences
- Proximal hypertension: Systolic and diastolic pressures rise in the ascending aorta and branches (subclavian, carotid), exposing the brain, heart, and upper body to chronic pressure overload.
- Distal hypotension: Reduced perfusion pressure in the descending aorta, mesentery, and lower extremities causes lower-limb claudication, cool extremities, and exercise intolerance.
- Collateral circulation: Chronic obstruction stimulates development of internal mammary, intercostal, scapular, and mediastinal collaterals — visible on chest radiography as rib notching in older children and adults.
- Left ventricular hypertrophy: Progressive pressure overload leads to concentric LV hypertrophy, diastolic dysfunction, and ultimately systolic heart failure if untreated.
- Activation of the RAAS: Renal under-perfusion stimulates renin release, contributing to systemic hypertension that may persist even after anatomical repair.
Associated Anomalies
| Association | Prevalence | Clinical Significance |
|---|---|---|
| Bicuspid aortic valve (BAV) | 50–85 % | Risk of aortic stenosis/regurgitation, aortopathy; requires serial echo surveillance |
| Turner syndrome (45,X) | 10–15 % of CoA patients | Mandatory karyotyping in all females with CoA; increased risk of aortic dissection, hypothyroidism, short stature |
| Intracranial (Berry) aneurysm | 5–10 % | Screen with MRA brain at diagnosis; risk of subarachnoid haemorrhage |
| Patent ductus arteriosus (PDA) | 30–40 % (neonates) | Maintains lower-body perfusion prenatally; prostaglandin bridge to surgery |
| Ventricular septal defect (VSD) | 15–25 % | Adds volume load; may require concomitant surgical repair |
| Mitral valve abnormality | ~20 % | Bicuspid mitral valve, parachute MV; contributes to diastolic dysfunction |
| Shone complex | ~5 % | Supravalvular mitral ring, parachute MV, subaortic stenosis, CoA — left-heart obstruction cascade |
Genetic Considerations
While most cases are sporadic, familial clustering suggests polygenic inheritance. NOTCH1 and other genes in the Notch-signalling pathway have been implicated in both BAV and CoA. Genetic counselling is recommended for affected families, with echocardiographic screening of first-degree relatives of CoA patients, particularly those with BAV.
Clinical Features & Diagnosis
Presentation by Age Group
Physical Examination Findings
- Blood pressure: Upper-limb systolic BP > lower-limb systolic BP by ≥ 20 mmHg (normal: leg BP ~ 10–20 mmHg > arm BP). Four-limb blood pressure measurement is essential in all hypertensive children.
- Pulse discrepancy: Delayed and diminished femoral pulses compared with radial/brachial pulses (radiofemoral delay).
- Auscultation: Systolic ejection murmur maximal at left interscapular region posteriorly; continuous murmur if significant collaterals; ejection click if BAV present.
- Bruits: Systolic or continuous bruit over collaterals in the back or chest wall.
- Signs of BAV: Early-peaking systolic murmur at the right upper sternal border; aortic regurgitation diastolic murmur.
- Turner syndrome stigmata: Short stature, webbed neck, low posterior hairline, broad chest with widely spaced nipples, cubitus valgus, lymphoedema of hands/feet.
Diagnostic Algorithm
Investigations
Management
Initial Stabilisation (Neonatal Critical CoA)
Surgical Repair
Surgery is the preferred definitive treatment for neonates, infants, and young children with native coarctation, and for patients with complex arch anatomy or associated intracardiac lesions requiring concurrent repair.
Transcatheter Intervention
Balloon angioplasty with or without stent implantation is the preferred approach for older children, adolescents, and adults with native coarctation or re-coarctation post-surgery. Procedures are performed in the cardiac catheterisation laboratory under general anaesthesia.
Choice of Intervention — Decision Framework
| Patient Group | Preferred Intervention | Rationale |
|---|---|---|
| Neonate / Infant < 1 year | Surgery — extended end-to-end anastomosis | Small vessel size precludes stent; lowest re-coarctation rate; concomitant repair of VSD/PDA |
| Child 1–8 years / < 25 kg | Surgery preferred; balloon angioplasty for re-coarctation | Vessels too small for adult stents; surgery has durable results |
| Child > 8 years / > 25 kg | Balloon angioplasty ± stent | Sufficient vessel size; less invasive; rapid recovery |
| Adolescent / Adult | Stent implantation (covered stent preferred) | Excellent gradient reduction; lower complication rate than surgery in adults; covered stent reduces aneurysm risk |
| Re-coarctation post-surgery | Balloon angioplasty ± stent | Reoperation carries higher morbidity; transcatheter approach preferred |
| CoA with complex arch / Shone complex | Surgery (staged if necessary) | Requires arch reconstruction; transcatheter not feasible |
Antihypertensive Pharmacotherapy
Hypertension persists in 25–70 % of patients after successful coarctation repair. Pharmacotherapy is essential and may be required lifelong. Beta-blockers are generally preferred as first-line agents.
Special Populations
Aboriginal and Torres Strait Islander Health Considerations
📚 References
- 1. Baumgartner H, De Backer J, Babu-Narayan SV, et al. 2020 ESC Guidelines for the management of adult congenital heart disease. European Heart Journal. 2021;42(6):563–645.
- 2. Stout KK, Daniels CJ, Aboulhosn JA, et al. 2018 AHA/ACC Guideline for the Management of Adults with Congenital Heart Disease. Circulation. 2019;139(14):e698–e800.
- 3. Feltes TF, Bacha E, Beekman RH, et al. Indications for cardiac catheterization and intervention in pediatric cardiac disease: a scientific statement from the AHA. Circulation. 2011;123(22):2607–2652.
- 4. Australian Institute of Health and Welfare (AIHW). Congenital heart disease in Australia. Cat. no. CVD 89. Canberra: AIHW; 2023.
- 5. Brown ML, Burkhart HM, Connolly HM, et al. Coarctation of the aorta: lifelong surveillance is mandatory following surgical repair. Journal of the American College of Cardiology. 2013;62(11):1020–1025.
- 6. Kenny D, Hijazi ZM. Coarctation of the aorta: from fetal life to adulthood. Cardiology Journal. 2011;18(5):487–495.
- 7. Carr JA. The results of catheter-based therapy compared with surgical repair of adult aortic coarctation. Journal of the American College of Cardiology. 2006;47(6):1101–1107.
- 8. Rao PS. Balloon angioplasty of native coarctation of the aorta. Journal of Interventional Cardiology. 2015;28(2):189–200.
- 9. Warnes CA, Williams RG, Bashore TM, et al. ACC/AHA 2008 Guidelines for the Management of Adults with Congenital Heart Disease. Journal of the American College of Cardiology. 2008;52(23):e143–e263.
- 10. Regitz-Zagrosek V, Roos-Hesselink JW, Bauersachs J, et al. 2018 ESC Guidelines for the management of cardiovascular diseases during pregnancy. European Heart Journal. 2018;39(34):3165–3241.
- 11. Australian Institute of Health and Welfare (AIHW). Aboriginal and Torres Strait Islander health performance framework: cardiovascular disease. Canberra: AIHW; 2023.
- 12. Royal Australasian College of Physicians (RACP). Transition to adult health services for young people with chronic conditions. Sydney: RACP; 2018.
- 13. Maron BJ, Zipes DP, Kovacs RJ. Eligibility and disqualification recommendations for competitive athletes with cardiovascular abnormalities: Preamble, principles, and general considerations. Journal of the American College of Cardiology. 2015;66(21):2343–2349.