📋 Key Information Summary
- Heart failure (HF) is a complex clinical syndrome resulting from structural or functional cardiac impairment, leading to impaired ventricular filling or ejection.
- The New York Heart Association (NYHA) functional classification grades HF severity from Class I (no limitation) to Class IV (symptoms at rest).
- Affects ~500,000 Australians; incidence rises sharply with age (>5% in those >75 years). Leading cause of hospitalisation in older Australians.
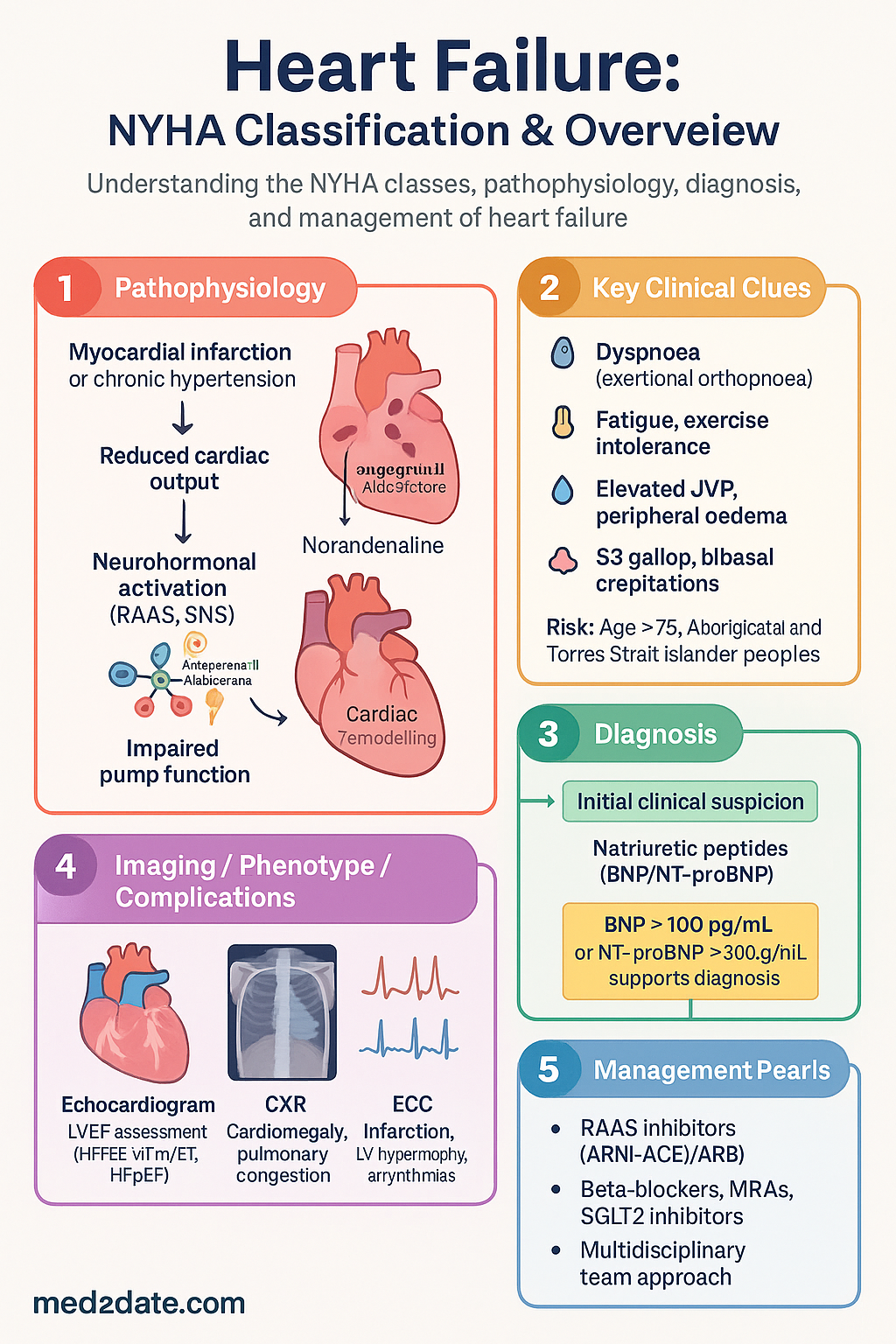
- Primary pathophysiology involves neurohormonal activation (RAAS, SNS) leading to adverse cardiac remodelling.
- Diagnosis requires integration of symptoms, signs (e.g., elevated JVP, peripheral oedema), natriuretic peptides (BNP/NT-proBNP), and echocardiography.
- BNP >100 pg/mL or NT-proBNP >300 pg/mL supports diagnosis; higher levels correlate with severity and prognosis.
- Immediate assessment includes ECG, CXR, troponin (to exclude acute coronary syndrome), and baseline bloods (FBC, eGFR, LFTs, TFTs).
- Echocardiography is essential to determine left ventricular ejection fraction (LVEF), categorising HF as reduced (HFrEF, ≤40%), mildly reduced (HFmrEF, 41-49%), or preserved (HFpEF, ≥50%).
- Management is guided by NYHA class and LVEF, with foundational therapy for HFrEF including RAAS inhibitors (ARNI or ACEi/ARB), beta-blockers, MRAs, and SGLT2 inhibitors.
- Aboriginal and Torres Strait Islander peoples experience higher HF prevalence, younger age of onset, and poorer outcomes due to systemic inequities.
- A multidisciplinary team approach, including heart failure nurse specialists, is recommended for optimal care.
- Patient education on daily weight monitoring, fluid restriction, symptom recognition, and medication adherence is critical.
Introduction & Australian Epidemiology
Heart failure (HF) is a major public health concern in Australia, characterised by the heart's inability to pump blood at a rate sufficient to meet the metabolic demands of the body, or to do so only at elevated filling pressures. It is a terminal pathway for various cardiovascular diseases, including ischaemic heart disease, hypertension, and valvular disorders.
In Australia, HF affects an estimated 500,000 individuals. Prevalence increases dramatically with age, from less than 1% in those under 45 years to over 5% in the population aged 75 years and older. It is the most common cause of hospitalisation in Australians over 65 years, with over 60,000 hospital separations annually, representing a significant burden on the healthcare system. Despite advances in treatment, the prognosis remains poor, with a 5-year mortality rate following diagnosis estimated at 50-60%, worse than many common cancers.
The NYHA functional classification, as detailed below, provides a simple, clinically useful framework for grading symptom severity, assessing treatment response, and guiding prognosis. This overview will detail the NYHA classes, the fundamental pathophysiological processes driving HF, and the systematic approach to diagnosis and initial assessment in the Australian context.
NYHA Functional Classification
The New York Heart Association (NYHA) classification categorises HF based on the patient's symptomatic limitation of physical activity. It is subjective and clinician-assessed, but remains widely used for treatment stratification and clinical communication.
| Class | Functional Capacity | Objective Assessment |
|---|---|---|
| I | No limitation of physical activity. Ordinary physical activity does not cause undue dyspnoea, fatigue, or palpitations. | Cardiac disease with no objective evidence of functional limitation. |
| II | Slight limitation. Comfortable at rest, but ordinary physical activity results in dyspnoea, fatigue, or palpitations. | Objective evidence of minimal cardiac disease (e.g., mild left ventricular dysfunction on echo, minimal fluid on CXR). |
| III | Marked limitation. Comfortable at rest, but less than ordinary activity causes dyspnoea, fatigue, or palpitations. | Objective evidence of moderately severe cardiac disease (e.g., moderate LV dysfunction, pulmonary congestion). |
| IV | Unable to carry out any physical activity without discomfort. Symptoms of cardiac insufficiency at rest. If any activity is undertaken, discomfort increases. | Objective evidence of severe cardiac disease (e.g., severe LV dysfunction, pulmonary oedema). |
Pathophysiology of Heart Failure
HF is a progressive disorder. The initial index event (e.g., myocardial infarction) or chronic load (e.g., hypertension) leads to a reduction in cardiac output. This triggers a series of compensatory neurohormonal responses that, while initially adaptive, become maladaptive and drive disease progression through a process known as cardiac remodelling.
Cardiac Remodelling: This involves changes in ventricular size, shape, and function. Key features include:
- Myocyte hypertrophy: Increased cell size to enhance contractile force, but at the cost of increased oxygen demand and potential for dysfunction.
- Myocyte apoptosis and necrosis: Progressive loss of functional myocytes.
- Altered extracellular matrix: Increased collagen deposition (fibrosis), leading to increased myocardial stiffness and impaired relaxation (diastolic dysfunction).
- Ventricular dilation: A spherical change in shape that increases wall stress (LaPlace's law) and reduces mechanical efficiency.
This remodelling creates a vicious cycle: impaired pump function → neurohormonal activation → further remodelling → worsening pump function.
Neurohormonal Activation (RAAS, SNS)
Two key interconnected systems are central to HF progression:
- Low cardiac output is sensed by baroreceptors, triggering increased sympathetic outflow.
- Effects: Increased heart rate, contractility, and vasoconstriction (afterload increase) to maintain perfusion.
- Long-term harm: Direct myocardial toxicity, increased myocardial oxygen demand, arrhythmogenesis, and further activation of RAAS.
- Elevated levels of noradrenaline correlate directly with mortality risk.
- Reduced renal perfusion and SNS stimulation promote renin release.
- Effects: Angiotensin II causes potent vasoconstriction, aldosterone promotes sodium/water retention and potassium excretion.
- Long-term harm: Volume overload, increased preload and afterload, cardiac and vascular fibrosis, endothelial dysfunction, and hypokalaemia (arrhythmia risk).
Diagnosis & Initial Assessment
Diagnosis is based on a compatible clinical presentation supported by objective evidence of cardiac dysfunction. A systematic approach is essential.
Clinical Features (History & Examination)
- Symptoms: Dyspnoea (exertional, orthopnoea, paroxysmal nocturnal), fatigue, exercise intolerance, fluid retention (peripheral oedema, abdominal bloating), nocturia.
- Signs: Elevated jugular venous pressure (JVP), hepatojugular reflux, laterally displaced apex beat, S3 gallop, bibasal crepitations, peripheral pitting oedema.
Investigations
Aetiological Workup
Always seek the underlying cause: Ischaemic heart disease, hypertension, valvular heart disease, cardiomyopathy (dilated, hypertrophic, restrictive), myocarditis, toxins (e.g., alcohol, chemotherapy), peripartum cardiomyopathy, or high-output states.
Special Populations
Aboriginal and Torres Strait Islander peoples experience a disproportionate burden of heart failure:
Common due to cardiorenal syndrome. Requires careful dosing of diuretics and neurohormonal antagonists.
- Diuretics: May need higher loop diuretic doses (e.g., furosemide) if eGFR low. Monitor potassium.
- ACEi/ARB/ARNI: Can be started if eGFR >30 mL/min/1.73m². Initiate at low dose, monitor K+ & Cr at 1-2 weeks. May need to be temporarily withheld during acute intercurrent illness.
- MRAs: Spironolactone/eplerenone can be used if eGFR >30 mL/min/1.73m² and K+ <5.0 mmol/L. Use low dose (spironolactone 25 mg OD) with strict monitoring.
- SGLT2 Inhibitors: Dapagliflozin and empagliflozin maintain cardiorenal benefits down to eGFR ~20 mL/min/1.73m².
Paediatric HF has different aetiologies (congenital heart disease, myocarditis, cardiomyopathies). NYHA classification is less applicable; the Ross Classification (for infants) or modified NYHA for older children is used. Management is highly specialised, requiring tertiary paediatric cardiology involvement.
📚 References
- 1. Atherton JJ, Sindone A, De Pasquale CG, et al. National Heart Foundation of Australia and Cardiac Society of Australia and New Zealand: Australian clinical guidelines for the management of heart failure 2018. Med J Aust. 2018;209(8):363-369.
- 2. McDonagh TA, Metra M, Adamo M, et al. 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure. Eur Heart J. 2021;42(36):3599-3726.
- 3. Heidenreich PA, Bozkurt B, Aguilar D, et al. 2022 AHA/ACC/HFSA Guideline for the Management of Heart Failure. J Am Coll Cardiol. 2022;79(17):e263-e421.
- 4. Australian Institute of Health and Welfare (AIHW). Heart, stroke and vascular disease—Australian facts. Cat. no. CVD 87. Canberra: AIHW; 2021.
- 5. Sahle BW, Owen AJ, Mutowo MP, Krum H, Reid CM. Prevalence of heart failure in Australia: a systematic review. BMC Cardiovasc Disord. 2016;16:32.
- 6. The Criteria Committee of the New York Heart Association. Nomenclature and Criteria for Diagnosis of Diseases of the Heart and Great Vessels. 9th ed. Boston: Little, Brown & Co; 1994:253-256.
- 7. McMurray JJV, Packer M, Desai AS, et al. Angiotensin-neprilysin inhibition versus enalapril in heart failure. N Engl J Med. 2014;371(11):993-1004.
- 8. McMurray JJV, Solomon SD, Inzucchi SE, et al. Dapagliflozin in patients with heart failure and reduced ejection fraction. N Engl J Med. 2019;381(21):1995-2008.
- 9. Australian Commission on Safety and Quality in Health Care (ACSQHC). Australian Atlas of Healthcare Variation. Sydney: ACSQHC; 2017.
- 10. Brown A, Carrington MJ, Clark R, et al. Heart failure hospitalisation and mortality in Aboriginal and non-Aboriginal Australians. Int J Cardiol. 2019;285:53-59.
- 11. McDonagh TA, Metra M, Adamo M, et al. 2023 Focused Update of the 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure. Eur Heart J. 2023;44(37):3627-3639.
- 12. National Heart Foundation of Australia. Heart failure toolkit: A guide for health professionals. 2022.