📋 Key Information Summary
- Bradyarrhythmias and conduction defects complicate 15–25% of acute myocardial infarctions, with the pattern depending on infarct location.
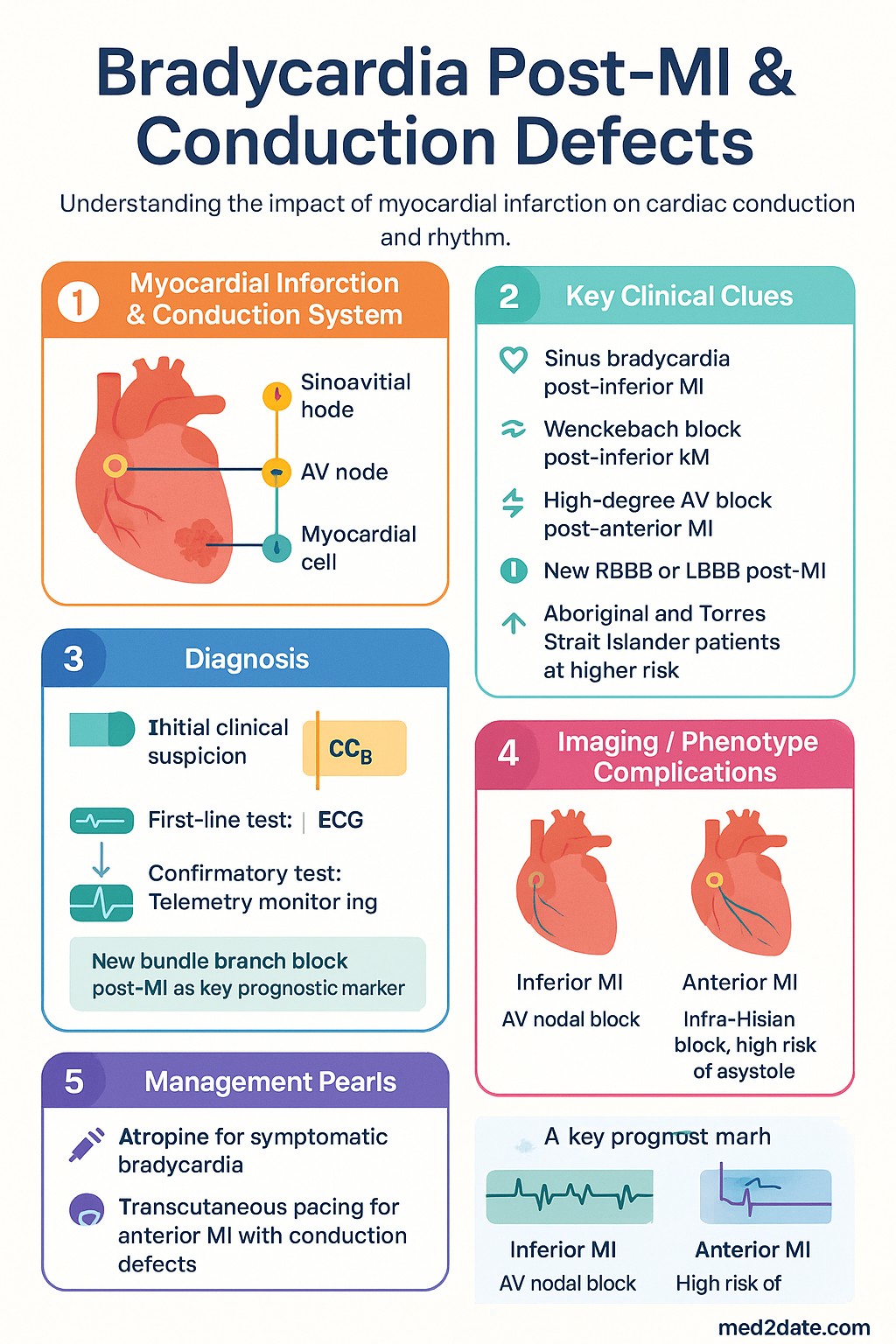
- Inferior MI typically affects the AV node via the right coronary artery, producing transient Wenckebach or second-degree AV block — usually self-limiting within 3–7 days.
- Anterior MI affects the infra-Hisian conduction system (bundle branches), causing higher-degree blocks with a 30–40% in-hospital mortality and higher risk of sudden cardiac death.
- Sinus bradycardia is the most common rhythm disturbance post-inferior MI; atropine 600 µg IV is first-line if haemodynamically significant.
- Type I second-degree AV block (Wenckebach) post-inferior MI is usually benign; Type II second-degree or complete heart block post-anterior MI mandates urgent evaluation for pacing.
- New right bundle branch block (RBBB) post-MI doubles mortality; new left bundle branch block (LBBB) carries even worse prognosis due to extensive anterior wall damage.
- Transcutaneous pacing pads should be applied prophylactically in anterior MI with any conduction abnormality; do not wait for haemodynamic deterioration.
- Temporary transvenous pacing is indicated for symptomatic bradycardia unresponsive to atropine, or any high-grade AV block in anterior MI.
- Permanent pacemaker implantation is indicated if high-degree AV block persists beyond 7–14 days post-infarction, or if infra-Hisian block is demonstrated on electrophysiology testing.
- All patients with new conduction defects post-MI require continuous telemetry monitoring and cardiology review; early coronary reperfusion remains the most effective strategy to prevent conduction complications.
- Avoid AV-nodal blocking agents (beta-blockers, digoxin, amiodarone, non-dihydropyridine CCBs) in the acute setting of high-degree AV block post-MI.
- Aboriginal and Torres Strait Islander patients experience higher rates of STEMI, delayed presentation, and reduced access to reperfusion therapy — increasing their risk of conduction complications.
Introduction & Australian Epidemiology
Bradyarrhythmias and conduction defects are among the most common rhythm disturbances encountered in acute myocardial infarction (MI). Their occurrence, pattern, severity, and prognosis are critically dependent on the infarct territory and the specific conduction structures affected by ischaemia or necrosis.
Conduction abnormalities complicate approximately 15–25% of all acute MIs. Sinus bradycardia and first-degree AV block occur in up to 15% of inferior MIs, while high-grade AV block (second-degree Type II or third-degree) affects approximately 3–5% of all MI presentations. New bundle branch block occurs in 10–15% of anterior MIs and is a powerful predictor of adverse outcomes.
In Australia, myocardial infarction remains a leading cause of morbidity and mortality, with over 57,000 hospitalisations annually according to the Australian Institute of Health and Welfare (AIHW). The pattern of conduction complications observed in Australian practice broadly mirrors international data, though regional variations exist due to differences in reperfusion timeliness and access to percutaneous coronary intervention (PCI), particularly in rural and remote settings.
Understanding the distinction between inferior (AV-nodal) and anterior (infra-Hisian) conduction defects is essential for risk stratification, guiding monitoring intensity, and determining the need for temporary or permanent cardiac pacing.
Inferior vs Anterior MI Conduction Defects
The conduction system's blood supply determines the pattern of post-MI conduction disturbance. Recognising whether conduction abnormalities arise from inferior or anterior infarction is critical for prognosis and management.
Inferior MI — AV Nodal Level
In approximately 90% of individuals, the AV node and proximal His bundle are supplied by the posterior descending artery (PDA), a branch of the right coronary artery (RCA). Inferior STEMI therefore preferentially causes ischaemia at the AV nodal level. The resulting blocks — first-degree AV block, Wenckebach (Mobitz Type I), and transient complete heart block — are typically due to enhanced vagal tone and reversible ischaemia rather than permanent necrosis.
- First-degree AV block occurs in 10–15% of inferior MIs.
- Second-degree Type I (Wenckebach) occurs in 5–10%.
- Complete heart block occurs in 5–10%, usually preceded by Wenckebach.
- Escape rhythm is typically narrow complex (junctional) at 40–60 bpm.
- Block is usually transient, resolving within 3–7 days; permanent pacing is rarely needed.
- In-hospital mortality associated with AV block in inferior MI is approximately 15–20%, largely due to larger infarct size rather than the block itself.
Anterior MI — Infra-Hisian Level
Anterior MI, typically from left anterior descending (LAD) artery occlusion, causes necrosis of the interventricular septum and damage to the bundle of His and its branches (right bundle branch, left anterior and posterior fascicles). This produces infra-Hisian block, which is inherently more dangerous because:
- The escape rhythm originates from ventricular myocardium (wide complex, slow, unreliable at 20–40 bpm).
- There is a high risk of asystole due to extensive conduction tissue destruction.
- New RBBB occurs in 10–15% of anterior MIs; new LBBB in 5–10%.
- Bifascicular block (RBBB + left anterior or posterior fascicular block) post-MI carries a 20–30% risk of progression to complete heart block.
- Trifascicular block (RBBB + alternating LAFB/LPFB, or RBBB + first-degree AV block) has the highest risk of progression.
- In-hospital mortality with complete heart block in anterior MI is 40–70%.
- Prophylactic temporary pacing is frequently indicated.
| Feature | Inferior MI | Anterior MI |
|---|---|---|
| Level of block | AV node (supra-Hisian) | Infra-Hisian (His–Purkinje) |
| Artery involved | RCA / PDA (90%) | LAD |
| Common block types | 1° AVB, Wenckebach, transient CHB | New RBBB/LBBB, bifascicular, CHB |
| Escape rhythm | Narrow, junctional, 40–60 bpm | Wide, ventricular, 20–40 bpm |
| Duration | Usually transient (3–7 days) | Often permanent |
| Permanent pacing | Rarely required | Frequently required |
| Mortality with CHB | 15–20% | 40–70% |
| Atropine responsive | Usually yes | Often ineffective |
Sinus Bradycardia & AV Block Post-MI
Sinus Bradycardia
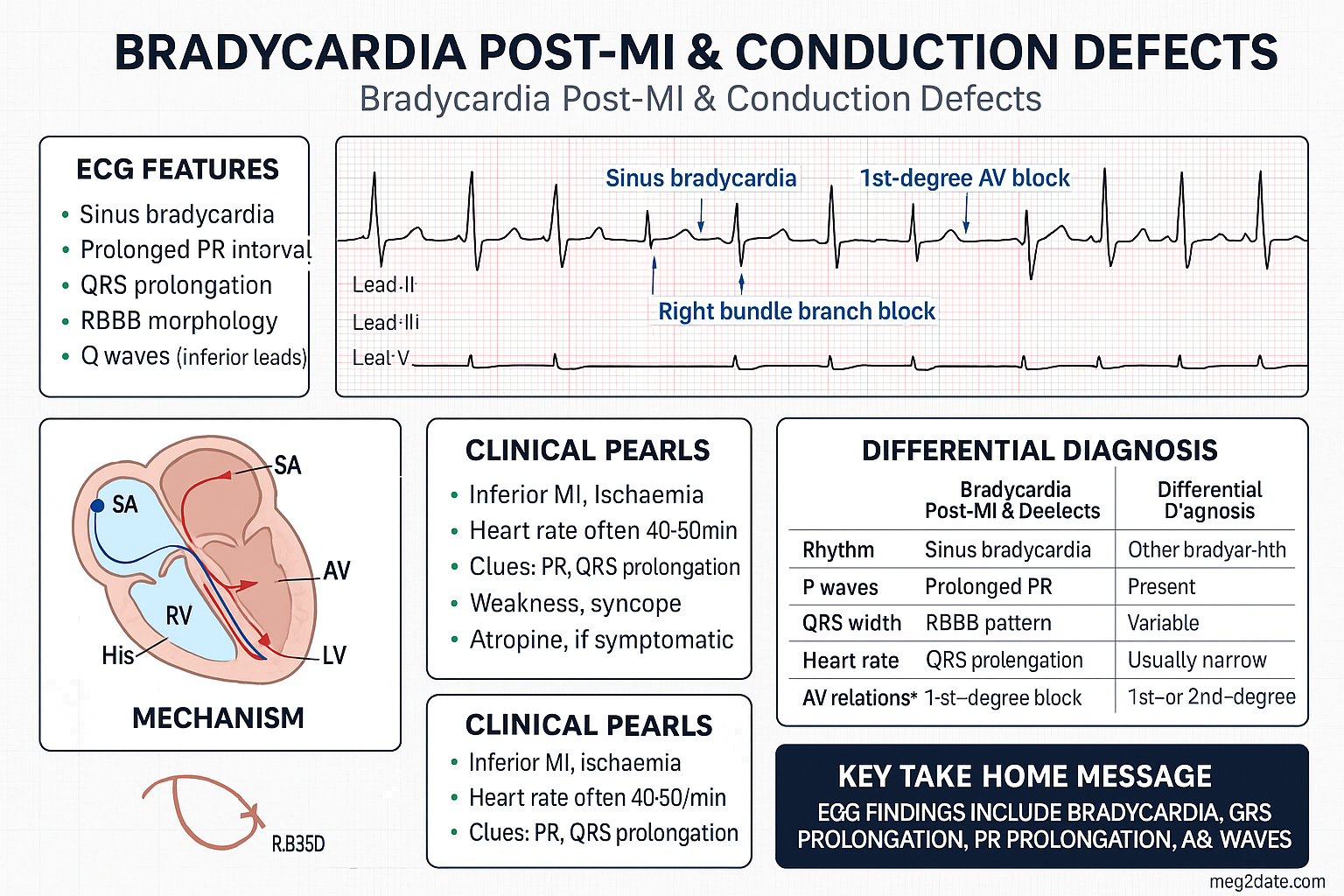
Sinus bradycardia (heart rate <60 bpm with normal P-wave morphology) is the most common arrhythmia following inferior MI, occurring in up to 40% of cases. It results from increased vagal tone (Bezold–Jarisch reflex), direct sinus node ischaemia, or the effect of reperfusion following thrombolysis or primary PCI.
Management approach:
- Asymptomatic: Observe; no specific treatment required. Avoid reflexively giving atropine.
- Haemodynamically significant (symptomatic hypotension, altered consciousness, ongoing chest pain, or signs of heart failure):
- Atropine sulfate 600 µg IV bolus; may repeat every 3–5 minutes to a maximum of 3 mg.
- Note: Atropine is less effective for infra-Hisian block.
- Refractory: Transcutaneous pacing (TCP) or isoprenaline infusion 1–4 µg/min IV as a bridge to transvenous pacing.
First-Degree AV Block
PR interval >200 ms. Occurs in 10–15% of MIs. Generally benign. Monitor on telemetry; review AV-nodal blocking medications. No specific treatment unless associated with haemodynamic compromise or progression to higher-degree block.
Second-Degree AV Block — Type I (Wenckebach / Mobitz I)
Progressive PR prolongation with eventual dropped QRS. Level of block is almost always at the AV node. Common in inferior MI. Usually self-limiting.
- Asymptomatic: Monitor on telemetry; no treatment.
- Symptomatic: Atropine 600 µg IV; if ineffective, transcutaneous pacing.
- Permanent pacing rarely required unless block persists >14 days with symptoms.
Second-Degree AV Block — Type II (Mobitz II)
Sudden dropped QRS without progressive PR prolongation. Level of block is infra-Hisian. High risk of progression to complete heart block.
Third-Degree (Complete) AV Block
Complete dissociation between atrial and ventricular activity. In inferior MI, the escape rhythm is typically junctional (narrow complex, 40–60 bpm) and the block may be transient. In anterior MI, the escape rhythm is ventricular (wide, slow, 20–40 bpm) and unreliable — high risk of asystole.
- Immediate: ABCs, IV access, continuous monitoring.
- Atropine 600 µg IV (may work in AV-nodal block; often ineffective in infra-Hisian block).
- Transcutaneous pacing — commence immediately if haemodynamically compromised or anterior MI.
- Transvenous temporary pacing — definitive treatment; arrange urgently.
- Dopamine 5–20 µg/kg/min or adrenaline infusion as bridge if pacing unavailable.
Bundle Branch Block Post-MI
New-onset bundle branch block (BBB) in the context of acute MI is a marker of extensive myocardial necrosis involving the interventricular septum. It indicates damage to the infra-Hisian conduction system and carries significant prognostic implications.
Right Bundle Branch Block (RBBB)
New RBBB occurs in 10–15% of anterior MIs and 1–2% of inferior MIs. The right bundle branch is a relatively long, thin structure supplied by the septal perforators of the LAD, making it vulnerable to anterior MI.
- ECG criteria: QRS ≥120 ms, RSR' pattern in V1–V2 (M-shaped), wide S wave in I and V6.
- New RBBB post-MI doubles in-hospital mortality (OR 2.0–2.7).
- Associated with larger infarct size and higher risk of cardiogenic shock.
- RBBB alone does not progress to complete heart block as frequently as bifascicular block.
- Isolated new RBBB post-MI: Monitor on telemetry; consider prophylactic TCP pads if anterior MI.
Left Bundle Branch Block (LBBB)
New LBBB post-MI occurs in 5–10% of cases and signifies extensive anterior wall damage involving both fascicles. LBBB in the setting of acute MI is an independent predictor of mortality.
- ECG criteria: QRS ≥120 ms, broad/notched R wave in I, aVL, V5–V6, absent Q waves in lateral leads, ST–T discordance.
- New LBBB post-MI: in-hospital mortality 25–40%.
- LBBB can obscure ST-elevation criteria (Sgarbossa criteria apply).
- Higher risk of progression to complete heart block than isolated RBBB.
Bifascicular & Trifascicular Block
Bifascicular block (RBBB + left anterior or left posterior fascicular block) post-MI indicates damage to at least two of the three fascicular pathways. This is a high-risk finding.
- Bifascicular block: 20–30% risk of progression to complete heart block.
- Trifascicular block (RBBB + alternating hemiblock, or RBBB + first-degree AV block): highest risk — consider prophylactic temporary pacing.
- Management: Apply transcutaneous pacing pads. Continuous telemetry. Cardiology consultation. Temporary transvenous pacing if anterior MI or symptomatic.
- Permanent pacemaker considered if block persists >7–14 days post-MI or if infra-Hisian disease confirmed on EP study.
| Conduction Abnormality | Risk of CHB | Pacing Pad? | Permanent PPM Likely? |
|---|---|---|---|
| New RBBB (isolated) | Low–moderate (5–10%) | Consider if anterior MI | Usually no |
| New LBBB | Moderate (10–15%) | Yes | Possibly |
| Bifascicular block | High (20–30%) | Yes — prophylactic | Frequently |
| Trifascicular block | Very high (30–40%) | Yes — mandatory | Usually yes |
| Alternating BBB | Extreme | Yes — mandatory | Yes |
Temporary & Permanent Pacing Indications
Transcutaneous Pacing (TCP)
Transcutaneous pacing is an immediate temporising measure that can be commenced at the bedside using external defibrillator/pacer pads. It is the first-line bridge to transvenous pacing in haemodynamically significant bradycardia post-MI.
- Apply pads immediately in any anterior MI with new conduction defect — do not wait for symptoms.
- Set demand rate 60–80 bpm; increase output (mA) until electrical capture is confirmed on monitor AND pulse is palpable.
- Analgesia/sedation required — pacing is painful. Consider IV fentanyl 25–50 µg or midazolam 1–2 mg.
- Confirm capture continuously; loss of capture requires immediate troubleshooting.
- TCP is a bridge — arrange transvenous pacing within hours if bradycardia persists.
Temporary Transvenous Pacing
Temporary transvenous pacing provides more reliable capture than TCP and is the standard in-hospital bridge for post-MI bradycardia. Insertion requires central venous access (typically right internal jugular or left subclavian) and fluoroscopic or echocardiographic guidance.
Indications for Temporary Pacing Post-MI
| Indication | Urgency | Notes |
|---|---|---|
| Symptomatic sinus bradycardia refractory to atropine | Urgent | TCP first; transvenous as bridge |
| Complete heart block post-anterior MI | Emergent | Apply TCP immediately; transvenous ASAP |
| Mobitz Type II AV block | Emergent | High risk of sudden asystole |
| New bifascicular block in anterior MI | Urgent — prophylactic | 20–30% risk of progression |
| New trifascicular block | Emergent — prophylactic | Highest risk conduction pattern |
| Alternating RBBB/LBBB | Emergent | Imminent risk of complete heart block |
| Bradycardia-dependent VT (torsades) | Emergent | Overdrive pacing at 90–110 bpm |
Permanent Pacemaker Post-MI
The decision to implant a permanent pacemaker post-MI is guided by the persistence of conduction abnormalities beyond the acute ischaemic phase, the level of block (AV nodal vs infra-Hisian), and the presence of symptoms.
| Indication for Permanent PPM | Class |
|---|---|
| Persistent third-degree AV block post-MI beyond 7–14 days | Class I |
| Persistent Mobitz Type II AV block post-MI | Class I |
| Transient high-degree AV block with new BBB (residual bifascicular block) | Class IIa |
| Persistent first-degree AV block with new BBB | Class IIb |
| Persistent second-degree Type I AV block (asymptomatic) | Class IIb |
| Transient AV block without BBB (resolved) | Not indicated (Class III) |
Device selection:
- Dual-chamber (DDD/DDR): Preferred if intact sinus node function; maintains AV synchrony.
- Single-chamber ventricular (VVI/VVIR): If persistent atrial fibrillation or atrial standstill.
- ICD (implantable cardioverter-defibrillator): Consider if LVEF ≤35% at ≥40 days post-MI (primary prevention of sudden cardiac death per MADIT-II / SCD-HeFT criteria).
- CRT (cardiac resynchronisation therapy): If LVEF ≤35%, LBBB with QRS ≥150 ms, NYHA II–IV on optimal medical therapy.
PBS notes for permanent pacemakers: Pacemaker implantation is covered under MBS item numbers for cardiac pacemaker insertion (MBS 38290–38316). Device replacement batteries/generators are also MBS-funded. ICD and CRT devices require TGA-listed devices and are covered under MBS under specific clinical criteria.
Pathophysiology
The cardiac conduction system is vulnerable to ischaemia and infarction due to its reliance on a limited blood supply. Understanding the anatomy of conduction system blood supply is fundamental to predicting the pattern of post-MI conduction disturbance.
AV Node Blood Supply
The AV node receives its blood supply from the AV nodal artery, which arises from the RCA in 90% of individuals (right-dominant circulation) and from the left circumflex artery (LCx) in 10% (left-dominant). The AV nodal artery also supplies the proximal portion of the bundle of His. Ischaemia to this region — typically from RCA occlusion causing inferior MI — produces AV-nodal-level conduction delay or block.
AV nodal ischaemia causes a relative increase in vagal tone, acetylcholine-mediated slowing of conduction through the compact AV node, and accumulation of adenosine. These effects are often reversible with reperfusion, explaining the transient nature of most inferior MI-associated AV blocks.
Bundle Branch Blood Supply
The right bundle branch (RBB) and the left anterior fascicle (LAF) are supplied by the septal perforating branches of the LAD. The left posterior fascicle (LPF) has a dual blood supply from both the LAD and the posterior descending artery, making it relatively more resistant to ischaemia. This explains why:
- RBBB is the most common new BBB post-anterior MI (thin, long, single blood supply).
- Left anterior fascicular block (LAFB) frequently accompanies RBBB (shared LAD supply).
- Isolated left posterior fascicular block (LPFB) is rare and implies very extensive damage.
- Extensive septal necrosis can destroy all three fascicles → complete infra-Hisian block.
Mechanisms of Post-MI Bradycardia
- Direct ischaemic injury: Cellular hypoxia reduces automaticity and conduction velocity.
- Increased vagal tone: The Bezold–Jarisch reflex — activation of vagal afferents by ischaemic myocardium — causes sinus bradycardia and hypotension, particularly in inferior MI.
- Adenosine release: Ischaemic cells release adenosine, which slows AV nodal conduction.
- Oedema and inflammation: Peri-infarct oedema can compress conduction tissue, causing transient block.
- Fibrosis: Late conduction abnormalities (days to weeks) result from fibrotic replacement of necrotic conduction tissue.
- Reperfusion injury: Paradoxical bradycardia can occur during successful reperfusion (PCI/thrombolysis), attributed to reactive oxygen species and calcium overload.
Clinical Presentation & Diagnostic Criteria
Clinical Features of Post-MI Bradycardia
The clinical presentation depends on the heart rate, level of AV block, ventricular escape rate, and baseline cardiac function. Many patients are asymptomatic, with bradycardia detected incidentally on telemetry.
- Asymptomatic: Common with sinus bradycardia and first-degree AV block. HR 40–60 bpm with adequate perfusion.
- Mild symptoms: Fatigue, exercise intolerance, dizziness, lightheadedness.
- Moderate symptoms: Presyncope, syncope, worsening heart failure, angina at rest.
- Severe symptoms: Cardiogenic shock, altered consciousness, seizures (Stokes–Adams attacks), cardiac arrest/asystole.
Diagnostic ECG Criteria
| Finding | ECG Criteria | Level |
|---|---|---|
| Sinus bradycardia | Regular P waves, rate <60 bpm, normal PR | SA node |
| First-degree AV block | PR >200 ms, 1:1 conduction preserved | Usually AV node |
| Mobitz I (Wenckebach) | Progressive PR prolongation → dropped QRS; PR resets after drop | AV node |
| Mobitz II | Constant PR → sudden dropped QRS without progressive prolongation | Infra-Hisian |
| Third-degree (complete) | Complete AV dissociation; atrial rate > ventricular rate; no relationship between P and QRS | Either |
| RBBB | QRS ≥120 ms; RSR' in V1–V2; broad S in I, V6 | RBB |
| LBBB | QRS ≥120 ms; broad/notched R in I, aVL, V5–V6; absent Q laterally | LBB |
| LAFB | Left axis deviation (−45° to −90°); qI, SIII pattern; QRS <120 ms | Left anterior fascicle |
| LPFB | Right axis deviation (+120°); SI, QIII pattern; QRS <120 ms | Left posterior fascicle |
Determining the Level of Block
When the level of block is uncertain, the following features can help localise it:
- Atropine response: Improvement with atropine suggests AV-nodal block. No response suggests infra-Hisian block.
- Escape rhythm morphology: Narrow QRS (≤120 ms) = junctional (AV node level). Wide QRS (>120 ms) = ventricular (infra-Hisian).
- Escape rate: 40–60 bpm = junctional (more reliable). 20–40 bpm = ventricular (unreliable).
- His bundle electrogram: Definitive — A–H interval prolonged = AV nodal; H–V interval prolonged = infra-Hisian. (Rarely required in acute setting.)
Investigations
Investigations focus on confirming the MI diagnosis, characterising the conduction abnormality, and assessing for complications that may influence management.
Risk Stratification
Risk stratification in post-MI conduction defects integrates infarct location, conduction abnormality type, haemodynamic status, and progression pattern to determine monitoring intensity and the likelihood of requiring permanent pacing.
Predictors of Progression to High-Grade Block
- Anterior MI location (vs inferior)
- New bifascicular or trifascicular block
- Mobitz Type I progressing to Mobitz Type II or CHB
- PR interval >240 ms with new BBB
- Prior conduction disease
- LVEF <40%
- Delayed reperfusion (>12 hours from symptom onset)
- Elderly age (>75 years)
Monitoring
All patients with post-MI conduction defects require structured monitoring to detect progression, guide pacing decisions, and support medication titration.
Medication Review — Agents to Avoid in Post-MI Bradycardia
- Beta-blockers: Hold or reduce dose if HR <50 bpm or high-degree AV block. Reintroduce cautiously once rhythm stabilises (usually day 2–3 if block resolves).
- Amiodarone: Potent AV-nodal blocker. Avoid in active high-degree AV block. If needed for VT/VF, ensure temporary pacing is in place.
- Digoxin: Avoid in bradycardia/AV block post-MI.
- Non-dihydropyridine CCBs (verapamil, diltiazem): Contraindicated in bradycardia or any degree of AV block.
- Ivabradine: Contraindicated in bradycardia (HR <60 bpm).
Special Populations
ATSI Health Considerations
Aboriginal and Torres Strait Islander Australians experience significantly higher rates of cardiovascular disease, including acute myocardial infarction, at younger ages compared with non-Indigenous Australians. These disparities have direct implications for the incidence, management, and outcomes of post-MI conduction defects.
- Refer to the Australian Institute of Health and Welfare (AIHW) cardiovascular disease reports for current Indigenous health data.
- Follow RHDAustralia guidelines for management of acute coronary syndromes in Indigenous populations.
- Engage Aboriginal Health Workers in all phases of care — from acute management to cardiac rehabilitation and long-term device follow-up.
- Utilise RFDS telehealth and ECG transmission services for remote communities.
- Ensure all patients are offered culturally appropriate cardiac rehabilitation programmes.
- Flag Indigenous status in patient records to ensure appropriate follow-up pathways are initiated.
📚 References
- 1. O'Gara PT, Kushner FG, Ascheim DD, et al. 2013 ACC