📋 Key Information Summary
- Hypertension affects ~6 million Australian adults and is the leading modifiable risk factor for cardiovascular disease, stroke, and chronic kidney disease.
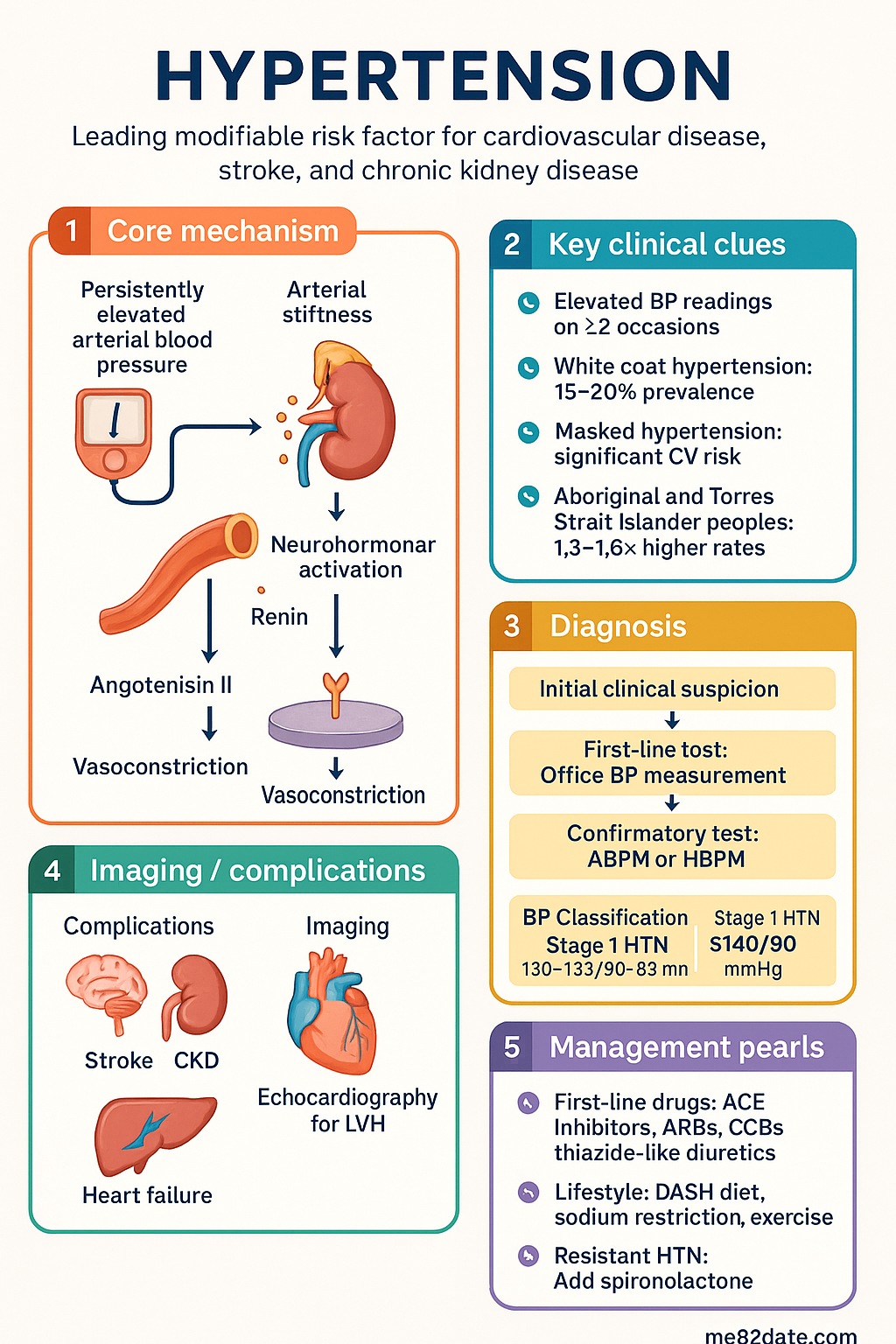
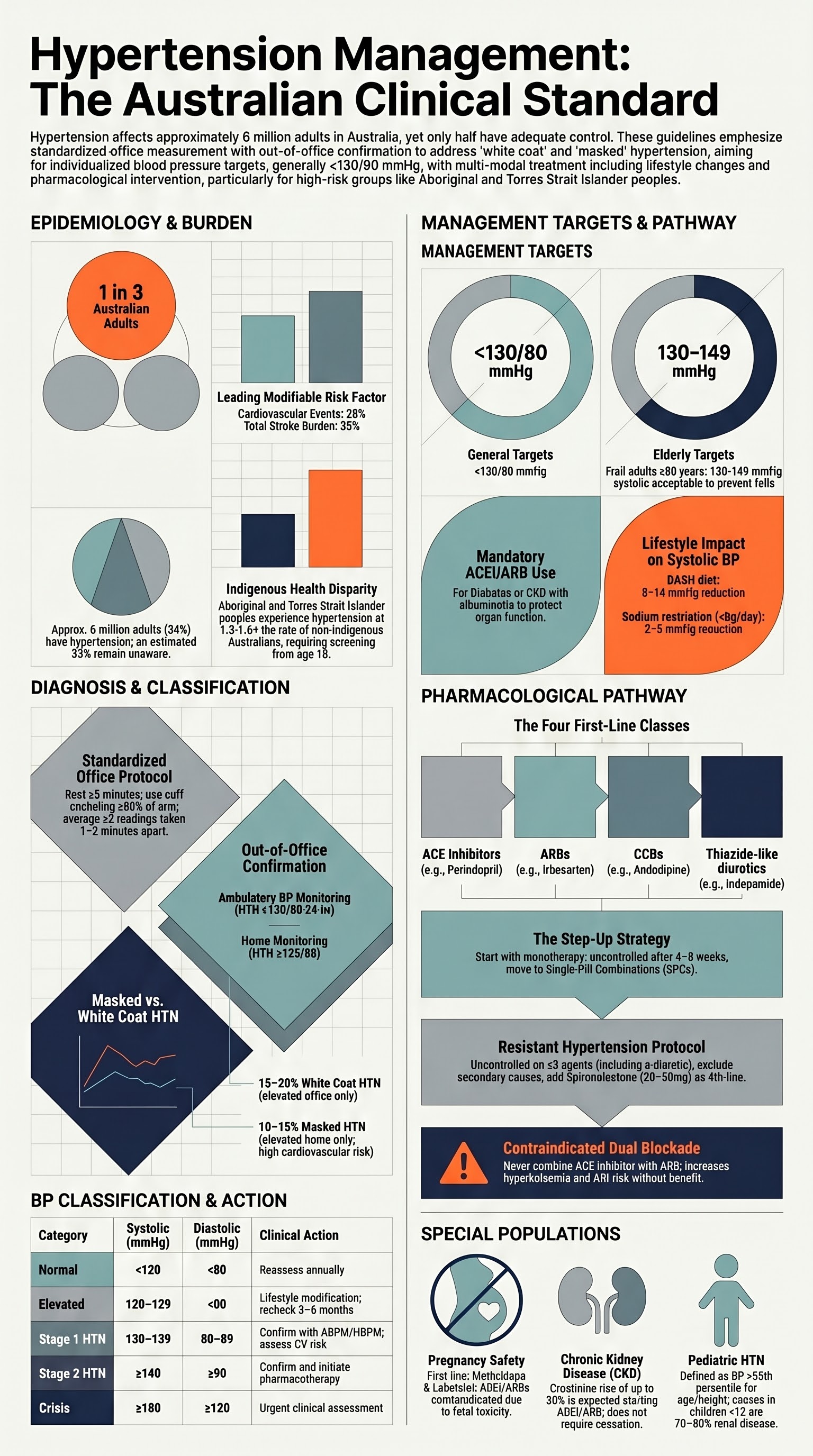
- Diagnosis requires ≥2 elevated readings on ≥2 separate occasions using a validated, calibrated device with correct cuff size; confirm with ambulatory BP monitoring (ABPM) or home BP monitoring (HBPM) where possible.
- Classification: Normal <120/80, Elevated 120–129/<80, Stage 1 HTN 130–139/80–89, Stage 2 HTN ≥140/90 mmHg; hypertensive crisis ≥180/120 mmHg.
- White coat hypertension (elevated office, normal out-of-office) affects ~15–20% of patients and does not mandate drug therapy in most cases; masked hypertension (normal office, elevated out-of-office) carries significant CV risk and requires treatment.
- General BP target is <130/80 mmHg for most adults; in frail elderly ≥80 years, a systolic target of 130–149 mmHg may be acceptable to avoid hypotension and falls.
- First-line antihypertensives: ACE inhibitors (e.g. perindopril, ramipril), ARBs (e.g. irbesartan, telmisartan), dihydropyridine CCBs (e.g. amlodipine), and thiazide-like diuretics (e.g. indapamide); all are PBS-listed as general benefits or authority required.
- If monotherapy fails at adequate dose within 4–8 weeks, step up to dual therapy; many patients will ultimately require ≥2 agents — single-pill combinations improve adherence.
- Resistant hypertension (BP uncontrolled on ≥3 agents including a diuretic) requires exclusion of secondary causes, medication non-adherence, and lifestyle factors; add spironolactone 25–50 mg OD as 4th-line agent.
- Screen for secondary hypertension when: onset <30 years, sudden worsening, resistant HTN, hypokalaemia, or clinical features of endocrine disease (phaeochromocytoma, Cushing's, primary aldosteronism).
- In pregnancy, methyldopa and labetalol are first-line; ACEi/ARBs are contraindicated. Labetalol is PBS authority-required for hypertension in pregnancy.
- Aboriginal and Torres Strait Islander peoples experience hypertension at 1.3–1.6× the rate of non-Indigenous Australians; earlier screening from age 18, culturally safe care, and addressing social determinants are essential.
- Lifestyle modifications (sodium restriction <5 g/day, DASH diet, ≥150 min/week exercise, weight loss, alcohol ≤10 standard drinks/week, smoking cessation) reduce systolic BP by 5–15 mmHg and should be recommended to every patient.
Introduction & Australian Epidemiology
Hypertension is defined as a persistently elevated arterial blood pressure (BP) and represents the single greatest modifiable risk factor for cardiovascular morbidity and mortality worldwide. In Australia, it is estimated that approximately 34% of adults (6 million people) have hypertension, yet only half are adequately controlled. Hypertension accounts for the largest burden of disease in Australia when expressed as disability-adjusted life years (DALYs).
The Australian Institute of Health and Welfare (AIHW) reports that hypertension contributes to approximately 28% of all cardiovascular events, 37% of ischaemic heart disease, and 35% of stroke burden in Australia. The prevalence increases with age: from ~10% in adults aged 25–34 to >60% in those aged ≥65 years. Men are more commonly affected than women until the age of 65, after which the prevalence in women exceeds that of men.
Aboriginal and Torres Strait Islander peoples experience hypertension at significantly higher rates (1.3–1.6× non-Indigenous Australians), with earlier onset, worse control, and disproportionate end-organ damage including higher rates of CKD, stroke, and heart failure. Remote and rural communities face additional barriers to screening, diagnosis, and long-term management.
The Australian cardiovascular risk calculator (Absolute Cardiovascular Disease Risk — ACVD calculator, endorsed by the National Vascular Disease Prevention Alliance) integrates BP with age, sex, smoking, diabetes, lipid levels, and family history to estimate 5-year risk of a cardiovascular event. Blood pressure management should always be contextualised within this global risk framework.
Diagnosis & Classification
Office Blood Pressure Measurement
Accurate office BP measurement is the foundation of hypertension diagnosis. Standardised technique is essential to avoid measurement error, which is common in busy Australian general practice.
- Patient preparation: Rest quietly for ≥5 minutes in a seated position, back supported, feet flat on the floor, arm supported at heart level. Avoid caffeine, exercise, and smoking for ≥30 minutes prior.
- Cuff selection: Use an appropriately sized cuff (bladder encircling ≥80% of arm circumference). A standard adult cuff fits arm circumference 22–32 cm; large adult cuff for 32–42 cm; thigh cuff for >42 cm.
- Measurement protocol: Take ≥2 readings, 1–2 minutes apart. Average the readings. On the first visit, measure BP in both arms; use the arm with the higher reading for subsequent monitoring. A difference of >20 mmHg systolic between arms warrants investigation for subclavian stenosis or aortic coarctation.
- Device validation: Use a validated automated oscillometric device (listed on www.stridebp.org). Mercury sphygmomanometers are being phased out in Australian clinical settings. Aneroid devices require 6-monthly calibration.
Blood Pressure Classification
| Category | Systolic (mmHg) | Diastolic (mmHg) | Action |
|---|---|---|---|
| Normal | <120 | <80 | Reassess annually |
| Elevated BP | 120–129 | <80 | Lifestyle modification; recheck in 3–6 months |
| Stage 1 Hypertension | 130–139 | 80–89 | Confirm with ABPM/HBPM; assess CV risk; treat if high risk |
| Stage 2 Hypertension | ≥140 | ≥90 | Confirm; initiate pharmacotherapy + lifestyle |
| Hypertensive Crisis | ≥180 | ≥120 | Urgent assessment; differentiate emergency vs urgency |
Ambulatory Blood Pressure Monitoring (ABPM)
ABPM is the gold standard for confirming hypertension diagnosis and is recommended for all patients with an initial elevated office reading. The device records BP every 15–30 minutes during waking hours and every 30–60 minutes during sleep over 24 hours. ABPM provides:
- Daytime (awake) average: threshold for hypertension is ≥135/85 mmHg
- Night-time (asleep) average: threshold is ≥120/70 mmHg
- 24-hour average: threshold is ≥130/80 mmHg
- Nocturnal dipping pattern: a <10% fall in BP during sleep ("non-dipping") is associated with increased cardiovascular risk
ABPM is available in most Australian metropolitan pathology services and some regional centres. An MBS item (Medicare rebate) is not currently available for ABPM in Australia, meaning patients may incur out-of-pocket costs ($50–$150). The Australian Medicare Benefits Schedule does not include a specific item number for 24-hour ABPM, though advocacy for inclusion continues through the National Hypertension Taskforce.
Home Blood Pressure Monitoring (HBPM)
HBPM is a practical and cost-effective alternative to ABPM for confirming diagnosis and monitoring treatment response. Patients should use a validated, upper-arm oscillometric device and follow a standardised protocol:
- Measure twice daily (morning and evening) for 7 consecutive days
- Discard day-1 readings; average the remaining readings
- Home HTN threshold: ≥135/85 mmHg (equivalent to office ≥140/90)
Devices can be purchased at pharmacies for $60–$150. The National Prescribing Service (NPS MedicineWise) maintains a list of recommended devices for Australian consumers.
White Coat Hypertension & Masked Hypertension
| Condition | Office BP | ABPM/HBPM | Prevalence | CV Risk | Management |
|---|---|---|---|---|---|
| White coat HTN | Elevated (≥140/90) | Normal (<135/85) | 15–20% of diagnosed HTN | Low–moderate (higher than true normotensives) | Lifestyle modification; regular monitoring; pharmacotherapy generally not required unless CV risk is high |
| Masked HTN | Normal (<140/90) | Elevated (≥135/85) | 10–15% of apparently normotensive patients | High (comparable to sustained HTN) | Lifestyle + pharmacotherapy; treat as sustained hypertension |
Investigations at Diagnosis
Blood Pressure Targets
The optimal BP target depends on patient characteristics, comorbidities, and the balance between cardiovascular benefit and risk of adverse effects (hypotension, falls, acute kidney injury). Australian guidelines (National Heart Foundation of Australia / Cardiac Society of Australia and New Zealand 2016 position statement, updated recommendations) and international trials (SPRINT, ACCORD, STEP) inform the following targets.
| Population | Systolic Target | Diastolic Target | Key Evidence / Notes |
|---|---|---|---|
| General population (most adults) | <130 mmHg | <80 mmHg | SPRINT trial; 2017 ACC/AHA guidelines; aligned with current Australian position |
| Diabetes mellitus | <130 mmHg | <80 mmHg | ACCORD, ADVANCE trials; ADS/CDA guidelines; ACEi or ARB preferred |
| Chronic kidney disease (CKD) | <130 mmHg | <80 mmHg | KDIGO 2021; ACEi or ARB mandatory if albuminuria (ACR ≥30 mg/mmol) |
| Established coronary artery disease (CAD) | <130 mmHg | <80 mmHg | Avoid SBP <110 if symptomatic hypotension; beta-blockers if post-MI |
| Post-stroke / TIA | <130 mmHg | <80 mmHg | PROGRESS trial; commence after acute phase (>48 h for ischaemic stroke) |
| Elderly <80 years | <130 mmHg | <80 mmHg | SPRINT elderly subgroup; individualise based on frailty and function |
| Elderly ≥80 years | 130–149 mmHg | <80 mmHg | HYVET trial; caution re falls, cognitive decline, renal function |
| Frail elderly / limited life expectancy | Individualised | Individualised | Avoid aggressive targets; quality-of-life considerations paramount |
Lifestyle Modification Targets
All patients with elevated BP or hypertension should receive lifestyle counselling. The expected systolic BP reductions are:
- Weight reduction: 1 mmHg per 1 kg lost (target BMI 18.5–24.9 kg/m²)
- DASH diet (high in fruits, vegetables, low-fat dairy, reduced saturated fat): 8–14 mmHg reduction
- Sodium restriction <5 g/day (≈2000 mg sodium): 2–8 mmHg reduction; aim for <1600 mg/day for greater effect
- Physical activity ≥150 min/week moderate-intensity aerobic: 4–9 mmHg reduction
- Alcohol moderation ≤10 standard drinks/week: 2–4 mmHg reduction
- Smoking cessation: Reduces overall CV risk significantly (no direct BP effect)
- Potassium-rich diet (≥90 mmol/day from food sources): 2–4 mmHg reduction
First-Line Therapies
Pharmacotherapy should be initiated for patients with sustained Stage 1 hypertension (≥130/80) who are at high absolute cardiovascular risk (≥10% 5-year ACVD risk) or who have established cardiovascular disease, diabetes, CKD, or target organ damage. For Stage 2 hypertension (≥140/90), pharmacotherapy should be started alongside lifestyle measures regardless of risk score.
First-Line Drug Classes
Combination Therapy
For patients with BP ≥20/10 mmHg above target, or Stage 2 hypertension at diagnosis, initiating two first-line agents simultaneously is recommended. Single-pill combinations (SPCs) improve adherence and are preferred. Available PBS-listed combinations include:
Second-Line & Add-On Agents
Resistant Hypertension
Resistant hypertension is defined as BP above target despite the use of ≥3 antihypertensive agents at optimal doses, including a diuretic. Before diagnosing resistant hypertension, clinicians must systematically exclude:
- Pseudo-resistance: White coat effect, incorrect measurement technique, non-adherence
- Medication-related causes: NSAIDs, oral contraceptives, decongestants, corticosteroids, stimulants, SSRIs, liquorice
- Lifestyle factors: Obesity, excessive salt intake, high alcohol intake (>14 standard drinks/week), physical inactivity
- Secondary causes: Primary aldosteronism, renal artery stenosis, phaeochromocytoma, Cushing's syndrome, obstructive sleep apnoea
The PATHWAY-2 trial demonstrated that spironolactone 25–50 mg OD is the most effective add-on agent for resistant hypertension, superior to doxazosin and bisoprolol. Add spironolactone as 4th-line agent if K⁺ <4.5 mmol/L and eGFR ≥45 mL/min/1.73 m².
Referral to a hypertension specialist should be considered if BP remains uncontrolled on 4 agents. Catheter-based renal denervation remains under investigation in Australia (SPYRAL HTN-OFF MED, RADIANCE-HTN SOLO trials) and is not yet standard of care.
Secondary Hypertension
Secondary hypertension accounts for 5–10% of all hypertension cases and should be suspected in specific clinical scenarios. Identification of secondary causes is critical because targeted treatment may be curative or substantially improve blood pressure control.
When to Screen for Secondary Hypertension
- Onset of hypertension at age <30 years (especially without family history or obesity)
- Sudden worsening of previously controlled BP
- Resistant hypertension (≥3 agents including a diuretic)
- Hypertensive crisis (BP ≥180/120)
- Hypokalaemia (spontaneous or diuretic-induced)
- Abdominal bruit (renovascular disease)
- Episodic hypertension with headaches, sweating, palpitations (phaeochromocytoma)
- Features of Cushing's syndrome
- Snoring, daytime somnolence, large neck circumference (obstructive sleep apnoea)
Primary Aldosteronism (Conn's Syndrome)
Primary aldosteronism (PA) is the most common secondary cause of hypertension, affecting 5–15% of hypertensive patients. It is significantly underdiagnosed in Australia. PA causes autonomous aldosterone secretion leading to sodium retention, potassium loss, and suppressed renin.
Screening: Measure plasma aldosterone concentration (PAC) and plasma renin activity (PRA) or direct renin concentration (DRC). Calculate the aldosterone-to-renin ratio (ARR). A positive screen (ARR >70 pmol/mIU with PAC >400 pmol/L) requires confirmatory testing (oral sodium loading, IV saline infusion, or fludrocortisone suppression test) at a specialist centre.
Treatment: Unilateral aldosterone-producing adenoma (APA) — laparoscopic adrenalectomy (cures hypertension in ~50%, improves in ~40%). Bilateral adrenal hyperplasia — medical management with spironolactone 25–100 mg OD or eplerenone 25–50 mg BD (eplerenone is not PBS-listed for PA in Australia and requires private prescription).
Renovascular Hypertension
Renal artery stenosis (RAS) is the most common renovascular cause. Atherosclerotic RAS predominates in older patients (>60 years) with diffuse atherosclerosis, while fibromuscular dysplasia (FMD) is seen in younger women (<50 years).
Diagnosis: Duplex renal ultrasonography is the preferred first-line screening test (sensitivity 85–90%, specificity 90–95% for significant stenosis). CT angiography (CTA) or MR angiography (MRA) provide definitive anatomical assessment. Digital subtraction angiography (DSA) remains the gold standard but is invasive.
Treatment: Medical therapy with ACEi/ARB (with renal function monitoring) is first-line for most patients. Renal artery stenting (PTRA) is reserved for: flash pulmonary oedema, progressive renal failure on ACEi/ARB, or FMD in young patients. The ASTRAL and CORAL trials did not demonstrate benefit of routine stenting over medical therapy for atherosclerotic RAS.
Phaeochromocytoma / Paraganglioma
Phaeochromocytomas are catecholamine-secreting tumours arising from chromaffin cells of the adrenal medulla (or extra-adrenal paraganglia). They are rare (0.1–0.6% of hypertensives) but carry high morbidity if undiagnosed.
Screening: Plasma-free metanephrines (preferred) or 24-hour urine for catecholamines, metanephrines, and vanillylmandelic acid (VMA). Plasma metanephrines have a sensitivity >96% for exclusion.
Treatment: Pre-operative alpha-blockade (phenoxybenzamine 10 mg BD, titrate to 20–40 mg BD, or doxazosin) for 10–14 days before surgery, followed by beta-blockade ONLY AFTER adequate alpha-blockade. IV saline repletion is essential. Laparoscopic adrenalectomy is the definitive treatment. Metyrosine (catecholamine synthesis inhibitor) may be used for pre-operative preparation in severe cases.
Obstructive Sleep Apnoea (OSA)
OSA is present in 30–50% of patients with resistant hypertension and is an independent risk factor for hypertension, atrial fibrillation, and cardiovascular events. Screening should be performed in all patients with resistant hypertension, obesity (BMI ≥30 kg/m²), or excessive daytime somnolence.
Diagnosis: Overnight polysomnography (PSG) or home sleep apnoea testing (HSAT). Apnoea-hypopnoea index (AHI) ≥5/hour with symptoms confirms diagnosis; AHI ≥30/hour is severe OSA.
Treatment: Continuous positive airway pressure (CPAP) reduces BP by 2–3 mmHg in OSA patients with resistant hypertension. Weight loss, positional therapy, and alcohol avoidance are adjunctive. Mandibular advancement devices may be considered for mild–moderate OSA.
Other Secondary Causes
| Cause | Key Features | Screening Test | Treatment |
|---|---|---|---|
| Cushing's syndrome | Central obesity, striae, proximal myopathy, moon facies, buffalo hump | 24-hr urinary cortisol, overnight dexamethasone suppression test, late-night salivary cortisol | Transsphenoidal surgery (pituitary); adrenalectomy; adrenal steroidogenesis inhibitors (ketoconazole, metyrapone) |
| Coarctation of the aorta | Upper limb hypertension, radio-femoral delay, rib notching on CXR, systolic murmur | Echocardiography, CT or MR angiography | Surgical repair or endovascular stenting; hypertension may persist post-repair |
| Thyroid disease | Hyperthyroidism: systolic HTN, tachycardia, weight loss; Hypothyroidism: diastolic HTN, bradycardia, weight gain | TSH, free T4, free T3 | Treat underlying thyroid disorder |
| Acromegaly | Coarsened features, enlarged hands/feet, headache, visual field defects | IGF-1, oral glucose tolerance test with GH suppression | Transsphenoidal surgery; somatostatin analogues (octreotide, lanreotide) |
Special Populations
Pregnancy
Chronic hypertension: Pre-existing HTN or new diagnosis before 20 weeks' gestation. Target BP: 110–135/80–85 mmHg (SOMANZ guidelines).
Gestational HTN: New hypertension (≥140/90) after 20 weeks without proteinuria. May progress to preeclampsia.
Preeclampsia: HTN + proteinuria (ACR ≥30 mg/mmol) or other end-organ dysfunction after 20 weeks. Requires delivery as definitive treatment; magnesium sulphate for seizure prophylaxis if severe.
• Methyldopa 250 mg PO BD-TDS, titrate to max 2 g/day — PBS General Benefit; most extensive safety data
• Labetalol 100 mg PO BD-TDS, titrate to max 800 mg/day — PBS Authority Required for pregnancy; β1/α-blocker
• Nifedipine MR 20 mg PO BD, titrate to max 90 mg/day — PBS General Benefit; avoid sublingual (acute hypotension)
Paediatrics
Definition: BP ≥95th percentile for age, sex, and height on ≥3 occasions. Pre-hypertension: ≥90th to <95th percentile.
Common causes in children <12 years: Renal disease (70–80%), coarctation of the aorta, endocrine disorders. In adolescents, essential (primary) hypertension predominates.
Measurement: Use auscultatory method with appropriate cuff; oscillometric devices acceptable for screening but elevated readings should be confirmed by auscultation.
Treatment: Lifestyle modification first. If pharmacotherapy required: ACEi (enalapril 0.08 mg/kg/day, max 0.6 mg/kg/day), ARB (losartan 0.7 mg/kg/day), CCB (amlodipine 0.06 mg/kg/day), or thiazide (chlorthalidone). Refer to paediatric nephrologist.
Elderly (≥65 Years)
Target: <130/80 mmHg if fit and robust; 130–149/80 if frail or ≥80 years; individualise in those with limited life expectancy or significant frailty.
Orthostatic hypotension: Measure standing BP at every visit. If systolic drop ≥20 mmHg or diastolic drop ≥10 mmHg on standing, reassess medication regimen.
Preferred agents: Low-dose ACEi/ARB, low-dose CCB (amlodipine 2.5–5 mg), low-dose indapamide (1.5 mg SR). Avoid high-dose thiazides (hyponatraemia risk), high-dose alpha-blockers (postural hypotension), and centrally-acting agents (clonidine — risk of rebound hypertension, sedation).
Renal monitoring: Check eGFR and K⁺ within 2 weeks of starting ACEi/ARB/diuretic and after dose changes. More frequent monitoring if eGFR <60 mL/min/1.73 m².
Falls risk: Aggressive BP lowering increases fall risk. The SPRINT MIND sub-study showed cognitive benefit with intensive treatment, but frailty assessment (Clinical Frailty Scale) should guide target selection.
Chronic Kidney Disease
Target: <130/80 mmHg for all CKD stages (KDIGO 2021). ACEi or ARB is mandatory if ACR ≥30 mg/mmol (albuminuric CKD).
ACEi/ARB in CKD: May cause initial rise in creatinine of up to 30% — this is expected and does not warrant cessation. Cease only if creatinine rises >30% or K⁺ >6.0 mmol/L. Recheck at 1–2 weeks after initiation or dose increase.
Diuretic choice: eGFR ≥30: indapamide or thiazide diuretic. eGFR <30: loop diuretic (frusemide 20–80 mg PO OD-BD, or bumetanide) — thiazides lose efficacy in advanced CKD.
Dialysis patients: ACEi/ARBs may be continued; avoid in patients with recurrent intradialytic hypotension. Volume management (dry weight assessment) is the cornerstone of BP control.
Hepatic Impairment
Preferred agents: Amlodipine (start 2.5 mg OD in Child-Pugh B/C), ACEi (caution with encephalopathy risk), beta-blockers (propranolol for portal hypertension prophylaxis if indicated).
Avoid: Diuretics at high doses (precipitate hepatic encephalopathy via hypokalaemia and alkalosis); spironolactone may be used at low dose (12.5–25 mg OD) for ascites but monitor K⁺ closely.
Metabolism considerations: Many antihypertensives undergo hepatic metabolism. Start low, go slow. Prefer renally cleared agents in combined hepatic-renal impairment.
Immunocompromised / Transplant
Kidney transplant: Hypertension is near-universal post-transplant. Target <130/80 mmHg. Dihydropyridine CCBs (amlodipine) are first-line; ACEi/ARBs may be used but monitor for hyperkalaemia and reduced GFR. Avoid non-DHP CCBs (diltiazem, verapamil) — potent CYP3A4 inhibitors that raise tacrolimus/ciclosporin levels.
Drug interactions: Calcineurin inhibitors (tacrolimus, ciclosporin) cause vasoconstriction and sodium retention, contributing to post-transplant HTN. Dose-adjust antihypertensives when interacting with immunosuppressants.
HIV on antiretrovirals: CCBs may interact with protease inhibitors (CYP3A4); beta-blockers with NNRTIs. Seek specialist pharmacology advice.
Aboriginal and Torres Strait Islander peoples experience a disproportionately high burden of hypertension and its complications. AIHW data show that Indigenous Australians have 1.3–1.6 times the prevalence of hypertension compared with non-Indigenous Australians, with earlier onset, worse control, and significantly higher rates of cardiovascular disease, stroke, heart failure, and end-stage kidney disease.
📚 References
- 1. National Heart Foundation of Australia; Cardiac Society of Australia and New Zealand. Position statement on the management of raised blood pressure in Australia. National Heart Foundation of Australia; 2016.
- 2. SPRINT Research Group, Wright JT Jr, Williamson JD, et al. A randomized trial of intensive versus standard blood-pressure control. N Engl J Med. 2015;373(22):2103–2116.
- 3. Whelton PK, Carey RM, Aronow WS, et al. 2017 ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ASH/ASPC/NMA/PCNA Guideline for the Prevention, Detection, Evaluation, and Management of High Blood Pressure in Adults. J Am Coll Cardiol. 2018;71(19):e127–e248.
- 4. KDIGO 2021 Clinical Practice Guideline for the Management of Blood Pressure in Chronic Kidney Disease. Kidney Int. 2021;99(3S):S1–S87.
- 5. Williams B, MacDonald TM, Morant SV, et al. Spironolactone versus placebo, bisoprolol, and doxazosin to determine the optimal treatment for drug-resistant hypertension (PATHWAY-2): a randomised, double-blind, crossover trial. Lancet. 2015;386(10008):2059–2068.
- 6. Beckett NS, Peters R, Fletcher AE, et al. Treatment of hypertension in patients 80 years of age or older. N Engl J Med. 2008;358(18):1887–1898. [HYVET trial]
- 7. ASTRAL Investigators, Wheatley K, Ives N, et al. Revascularization versus medical therapy for renal-artery stenosis. N Engl J Med. 2009;361(20):1953–1962.
- 8. Cooper WO, Hernandez-Diaz S, Arbogast PG, et al. Major congenital malformations after first-trimester exposure to ACE inhibitors. N Engl J Med. 2006;354(23):2443–2451.
- 9. Somerfield J, Beber S, Sheikh M, et al. Aboriginal and Torres Strait Islander cardiovascular health: a consensus statement. Heart Lung Circ. 2020;29(1):14–22.
- 10. Australian Institute of Health and Welfare (AIHW). Cardiovascular disease in Aboriginal and Torres Strait Islander people. AIHW; 2023.
- 11. The Australian Diabetes Society. Position statement: Blood pressure management in adults with diabetes. ADS; 2022.
- 12. Society of Obstetric Medicine of Australia and New Zealand (SOMANZ). Guideline for the management of hypertensive disorders of pregnancy. SOMANZ; 2014 (updated 2020).
- 13. National Vascular Disease Prevention Alliance. Absolute Cardiovascular Disease Risk Assessment — Quick Reference Guide for Health Professionals. NVDPA; 2012 (updated 2023).
- 14. Egan BM, Zhao Y, Axon RN. US trends in prevalence, awareness, treatment, and control of hypertension, 1988–2008. JAMA. 2010;303(20):2043–2050.
- 15. Funder JW, Carey RM, Mantero F, et al. The management of primary aldosteronism: case detection, diagnosis, and treatment: an Endocrine Society clinical practice guideline. J Clin Endocrinol Metab. 2016;101(5):1889–1916.