📋 Key Information Summary
- Myocarditis is inflammation of the myocardium diagnosed by clinical presentation, cardiac MRI (Lake Louise 2018 criteria), and endomyocardial biopsy (gold standard); incidence in Australia is estimated at 4–14 per 100,000 persons annually, though the true burden is likely higher due to subclinical cases.
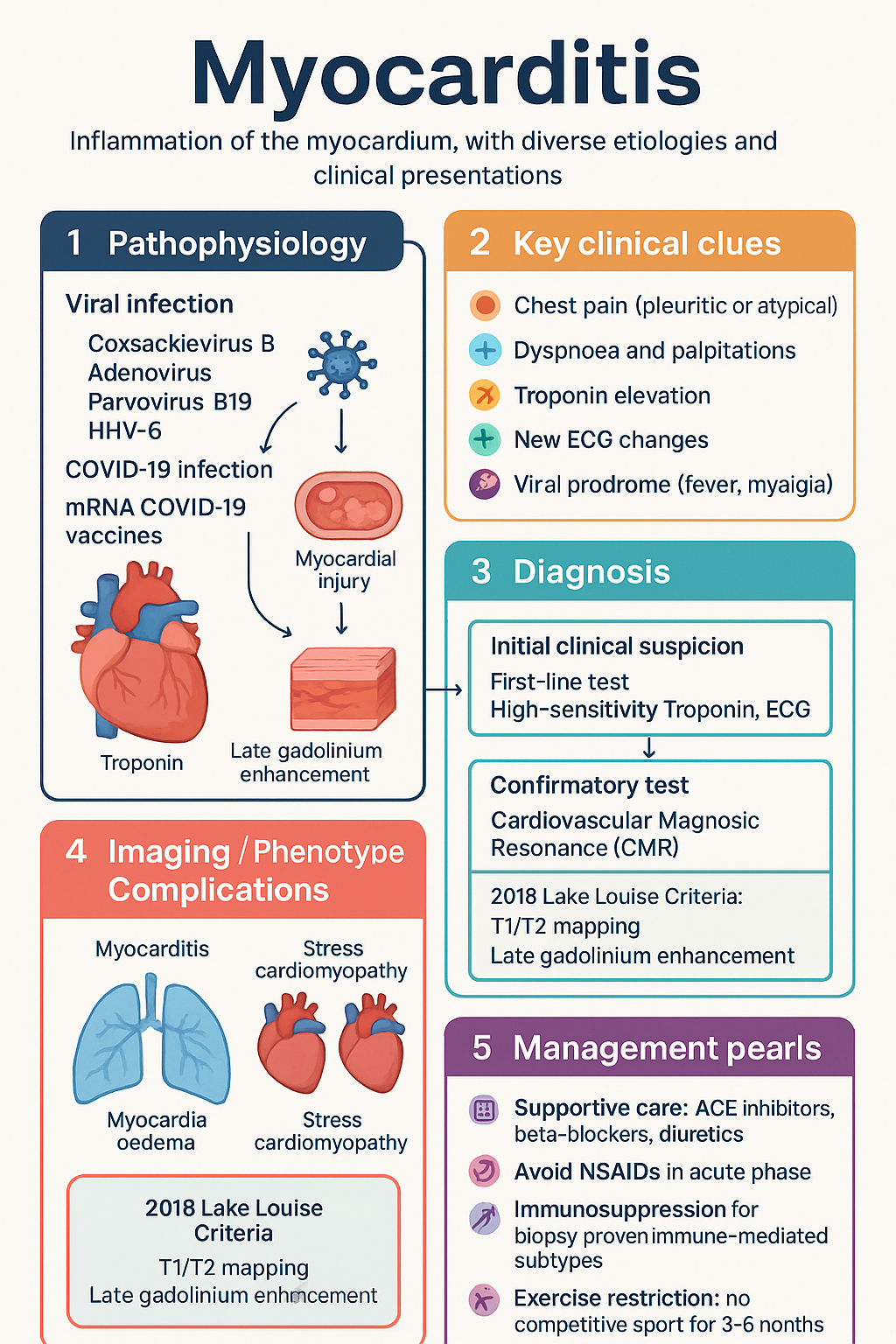
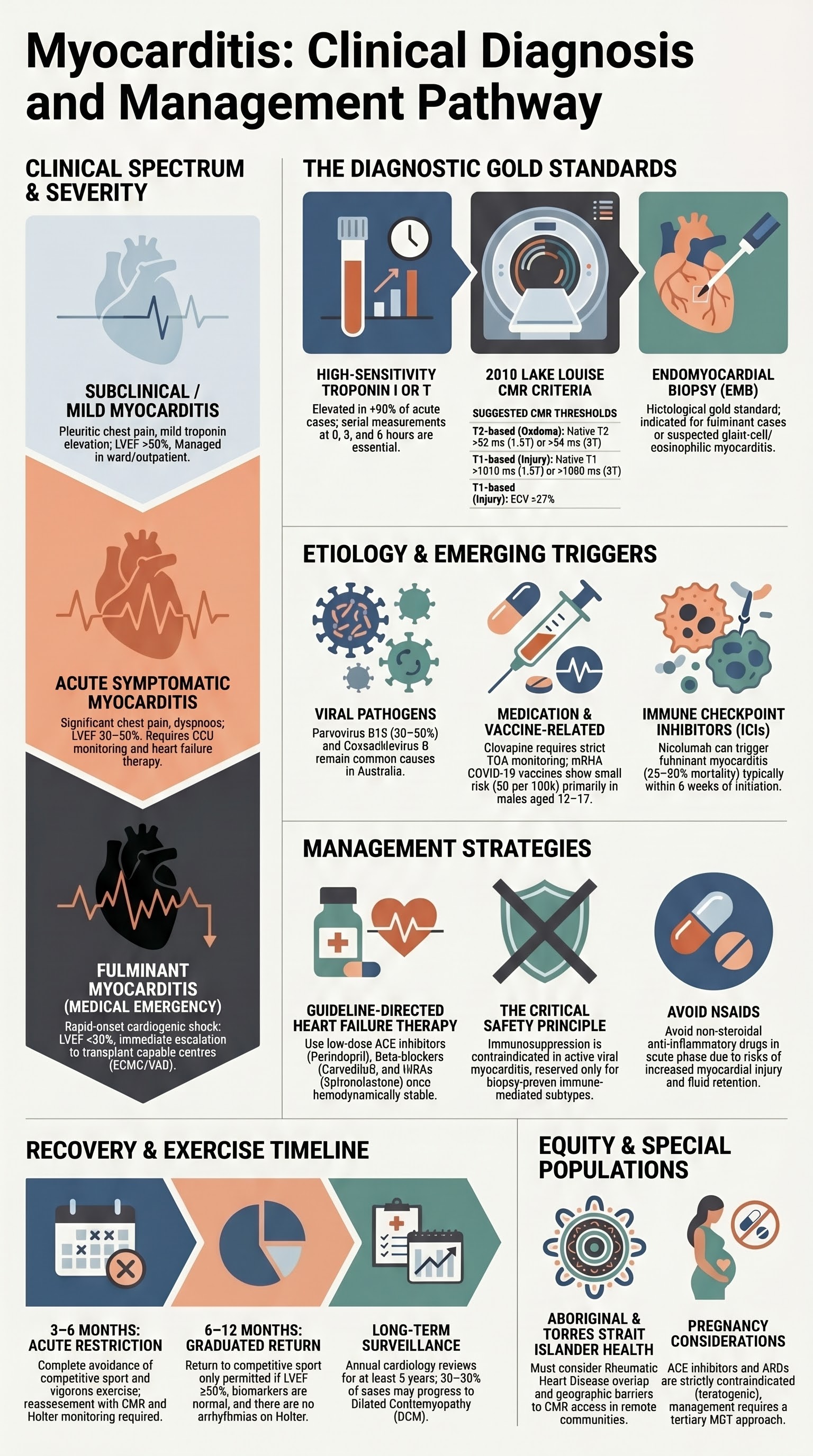
- Presentations range from subclinical chest pain to fulminant cardiogenic shock requiring mechanical circulatory support (MCS); any patient presenting with troponin elevation, new ECG changes, and cardiac symptoms without ischaemic cause should be evaluated for myocarditis.
- Viral aetiologies (Coxsackievirus B, adenovirus, parvovirus B19, HHV-6) remain the leading cause; COVID-19 infection and, rarely, mRNA COVID-19 vaccines (particularly in adolescent and young adult males) have emerged as important triggers since 2020.
- Cardiovascular magnetic resonance (CMR) is the cornerstone non-invasive diagnostic tool, applying the updated 2018 Lake Louise Criteria (T1/T2 mapping, late gadolinium enhancement, and oedema ratio).
- Endomyocardial biopsy (EMB) is indicated for fulminant presentations, suspected giant-cell or eosinophilic myocarditis, or when diagnosis remains uncertain after CMR — referral to a specialist centre with EMB capability is essential.
- Management is predominantly supportive: ACE inhibitors (perindopril, ramipril), beta-blockers (carvedilol, metoprolol), and diuretics for heart failure; avoid NSAIDs in the acute phase.
- Immunosuppression (corticosteroids, azathioprine, ciclosporin) is indicated only for biopsy-proven immune-mediated subtypes (giant-cell, eosinophilic, cardiac sarcoidosis) and should NOT be used empirically for viral myocarditis.
- Fulminant myocarditis with refractory cardiogenic shock requires urgent escalation: intra-aortic balloon pump (IABP), extracorporeal membrane oxygenation (ECMO), or ventricular assist devices (VAD) — early retrieval to a transplant-capable centre (e.g., Alfred Hospital Melbourne, St Vincent's Sydney, Prince Charles Brisbane).
- Exercise restriction: no competitive sport for a minimum of 3–6 months; return to activity only after normalisation of LV function, biomarkers, and absence of arrhythmias on ambulatory monitoring, guided by 2020 ESC sports cardiology criteria.
- Long-term follow-up is essential: repeat CMR at 6 and 12 months, echocardiography every 3–6 months during recovery, Holter monitoring for arrhythmia surveillance, and screening for progression to dilated cardiomyopathy.
- Aboriginal and Torres Strait Islander peoples have higher rates of rheumatic heart disease and may present with overlapping inflammatory myocarditis; culturally safe care, geographic access to specialist services, and early retrieval from remote communities are critical equity considerations.
- Pregnant women with acute myocarditis should be managed in a tertiary centre with obstetric and cardiac ICU capability; early multidisciplinary team (MDT) involvement is essential for delivery planning if haemodynamic deterioration occurs.
Introduction & Australian Epidemiology
Myocarditis is defined as inflammation of the myocardium, most commonly triggered by infectious agents, immune-mediated processes, or cardiotoxic substances. The disease spectrum extends from subclinical, self-limiting inflammation to fulminant cardiogenic shock and sudden cardiac death. Histologically, myocarditis is characterised by inflammatory cell infiltrate with or without associated myocyte necrosis, as established by the Dallas criteria and refined by subsequent immunohistochemical and molecular classification systems.
In Australia, myocarditis accounts for an estimated 4–14 cases per 100,000 persons per year, though autopsy and CMR studies suggest the true incidence may be considerably higher. Myocarditis is responsible for approximately 5–12% of sudden cardiac death in young adults and up to 9% of unexplained dilated cardiomyopathy presentations nationally. The Cardiac Society of Australia and New Zealand (CSANZ) recognises myocarditis as a significant and under-recognised cause of cardiac morbidity, particularly in younger populations.
Since the onset of the COVID-19 pandemic, Australian data from the National Centre for Immunisation Research and Surveillance (NCIRS) have documented increased myocarditis incidence associated with both SARS-CoV-2 infection and, at lower rates, mRNA COVID-19 vaccination (particularly BNT162b2 [Comirnaty®] in males aged 12–30 years). The Australian Therapeutic Goods Administration (TGA) continues to monitor these events through active surveillance.
The median age at presentation is 30–40 years, with a male-to-female ratio of approximately 1.5–2:1. Males are disproportionately affected in both viral and immune-mediated forms. In paediatric populations, myocarditis presents at a median age of 5–7 years, with viral aetiology predominating.
Clinical Presentation & Diagnosis
Myocarditis presents across a broad clinical spectrum. Accurate diagnosis requires integration of clinical features, biomarkers, ECG, echocardiography, and increasingly cardiovascular magnetic resonance (CMR). The diagnostic approach varies depending on whether the presentation is acute, chronic, or fulminant.
Clinical Spectrum: Acute, Chronic, and Fulminant Myocarditis
Diagnostic Approach
The initial evaluation of suspected myocarditis should include a systematic assessment combining clinical history, laboratory investigations, electrocardiography, and imaging. No single test is pathognomonic; diagnosis relies on the convergence of multiple findings.
Essential Investigations
2018 Lake Louise CMR Diagnostic Criteria
The updated Lake Louise Criteria require at least ONE T2-based criterion AND at least ONE T1-based criterion (or one from each category) for a CMR-based diagnosis of myocarditis. Native T1 mapping, T2 mapping, and extracellular volume fraction (ECV) significantly improve sensitivity compared to the original 2009 criteria.
| Criterion Category | Parameter | Technique | Suggested Threshold |
|---|---|---|---|
| T2-based (Oedema) | Regional or global myocardial oedema | T2-weighted STIR / T2 mapping | T2 ratio >1.9 (STIR); Native T2 >52 ms (1.5T) or >54 ms (3T) |
| Elevated T2 signal | T2 mapping | ≥2 SD above normal mean | |
| T1-based (Injury/Fibrosis) | Regional or global myocardial injury | Native T1 mapping | Native T1 >1010 ms (1.5T) or >1080 ms (3T); ≥2 SD above normal mean |
| Elevated extracellular volume | ECV quantification | ECV >27% | |
| Late gadolinium enhancement (LGE) | Post-gadolinium IR-GRE | Non-ischaemic pattern (epicardial/mid-wall, non-coronary territory) |
CMR diagnosis is positive when: ≥1 T2-based criterion AND ≥1 T1-based criterion are met. A CMR study is considered negative for acute myocarditis if neither T2 oedema nor T1-based criteria are present.
Indications for Endomyocardial Biopsy
EMB is recommended by CSANZ, AHA, and ESC in the following circumstances:
- Fulminant heart failure with haemodynamic instability (suspected giant-cell or eosinophilic myocarditis where specific therapy would change management)
- Heart failure with progressive LV dysfunction refractory to standard therapy for ≥2 weeks
- Suspected cardiac sarcoidosis or eosinophilic myocarditis where CMR is non-diagnostic
- New-onset heart failure of <2 weeks' duration with LV dilation and new ventricular arrhythmias or high-degree AV block
- Heart failure associated with cutaneous drug rash, peripheral eosinophilia, or suspected immune checkpoint inhibitor toxicity
Differential Diagnosis
The following conditions should be systematically excluded before confirming a diagnosis of myocarditis:
- Acute coronary syndrome (ACS): Coronary angiography should be performed if clinical features suggest ischaemic aetiology, particularly in patients >40 years or with cardiovascular risk factors.
- Acute pericarditis: Distinguished by predominant pleuritic chest pain, pericardial rub, diffuse ST elevation with PR depression, and normal troponin/pericardial effusion without ventricular dysfunction.
- Stress cardiomyopathy (Takotsubo): Apical ballooning pattern on echocardiography/CMR, often triggered by emotional or physical stress, typically reversible within weeks.
- Pulmonary embolism: Acute right heart strain, D-dimer elevation, CT pulmonary angiogram diagnostic.
- Acute decompensated cardiomyopathy: Pre-existing dilated cardiomyopathy with new decompensation — CMR features of chronicity (fibrosis pattern) aid differentiation.
Etiology
Myocarditis aetiology is diverse and often multifactorial. Identifying the underlying cause is essential because treatment strategies differ significantly between viral, immune-mediated, and drug-induced forms. In approximately 30–50% of cases, a specific aetiology cannot be identified despite comprehensive evaluation.
Viral Causes
Viral infection remains the most common identifiable cause of myocarditis in Australia. The pathogenesis involves direct viral cytopathic effects during the acute phase (days to weeks) followed by an immune-mediated inflammatory response (weeks to months). Molecular diagnosis via EMB tissue PCR has improved viral identification.
| Virus | Prevalence in Viral Myocarditis | Key Clinical Features | Australian Relevance |
|---|---|---|---|
| Parvovirus B19 | Most common (30–50% of viral cases by PCR) | Endothelial tropism; may cause microvascular dysfunction; often detected in EMB but causality debated | Endemic; common childhood infection |
| Coxsackievirus B (Enterovirus) | 15–25% | Classic viral myocarditis; direct myocyte lysis; linked to dilated cardiomyopathy progression | Summer/autumn seasonality; paediatric predominance |
| Human Herpesvirus 6 (HHV-6) | 10–20% | Latent reactivation; often co-detected with Parvovirus B19; significance debated | Common latent infection; reactivation in immunocompromised |
| Adenovirus | 5–10% | Paediatric predominance; often with concurrent respiratory illness | Common cause of paediatric viral myocarditis |
| SARS-CoV-2 | Emerging (see below) | Direct myocardial invasion via ACE2 receptors; cytokine-mediated injury; up to 20–30% of hospitalised COVID-19 patients show myocardial injury biomarkers | Significant pandemic burden; ongoing surveillance |
| Influenza A/B | 5–10% | Seasonal; may present with concurrent pneumonia and myocarditis | Annual influenza season (April–October); vaccination recommended |
| CMV, EBV, HIV | Individual: 2–5% each | Consider in immunocompromised patients; HIV-related cardiomyopathy has improved with ART | HIV: higher prevalence in priority populations |
Immune-Mediated Myocarditis
Immune-mediated myocarditis involves aberrant immune activation against cardiac tissue without active viral replication. These subtypes often require targeted immunosuppression and carry distinct prognoses. Diagnosis typically requires EMB with immunohistochemistry.
| Subtype | Histopathology | Clinical Features | Prognosis / Key Points |
|---|---|---|---|
| Giant-Cell Myocarditis (GCM) | Multinucleated giant cells + eosinophils + myocardial necrosis | Fulminant presentation in 75%; rapidly progressive HF, ventricular arrhythmias, high-degree AV block; often affects young–middle-aged adults | Poor prognosis without treatment (median transplant-free survival ~5.5 months); aggressive immunosuppression + early transplant listing essential |
| Eosinophilic Myocarditis | Eosinophilic infiltrate + myocyte necrosis; degranulation pattern | Associated with hypereosinophilic syndrome, drug reactions (antibiotics, anticonvulsants), parasitic infections, eosinophilic granulomatosis with polyangiitis (EGPA) | Treat underlying cause; corticosteroids first-line; mepolizumab for EGPA-related cases |
| Cardiac Sarcoidosis | Non-caseating granulomas with lymphocytic infiltrate | Conduction abnormalities, ventricular arrhythmias, HF; may present with syncope; 5–10% of systemic sarcoidosis patients have cardiac involvement | CMR (LGE in basal inferolateral wall) + PET (FDG uptake) for diagnosis; corticosteroids + steroid-sparing agents |
| Autoimmune Myocarditis | Lymphocytic infiltrate; no viral genome on PCR | Associated with SLE, rheumatoid arthritis, systemic sclerosis, inflammatory bowel disease; cardiac involvement may be the presenting feature | Treat underlying autoimmune disease; corticosteroids + disease-modifying agents |
Drug-Induced Myocarditis
Drug-induced myocarditis is an increasingly recognised entity. The most important categories in Australian clinical practice include:
- Immune checkpoint inhibitors (ICIs): Nivolumab, pembrolizumab, ipilimumab — ICI-related myocarditis occurs in 0.3–1.5% of treated patients, with mortality rates of 25–50%. Onset typically within 6 weeks of commencing therapy. Presentation is often fulminant with concurrent myositis and myasthenia gravis overlap. Key emerging cause
- Antimicrobials: Clofazimine, penicillins, cephalosporins, sulfonamides (eosinophilic pattern), dapsone.
- Antipsychotics: Clozapine (1–2% risk; requires baseline and serial troponin monitoring per TGA guidance), chlorpromazine.
- Recreational substances: Methamphetamine (increasingly prevalent in Australia), cocaine, synthetic cannabinoids.
- Other: Interferon-alpha, lithium (rare), TNF-alpha inhibitors (paradoxical).
COVID-19 and Vaccine-Related Myocarditis
Since 2020, SARS-CoV-2 infection and mRNA COVID-19 vaccination have emerged as important considerations in the differential diagnosis of myocarditis.
- Mechanism: direct viral invasion via myocardial ACE2 receptors, cytokine storm, microvascular thrombosis, and autoimmune cross-reactivity
- Incidence: myocardial injury (troponin elevation) in 20–30% of hospitalised COVID-19 patients; clinical myocarditis diagnosed in approximately 2–5%
- Higher risk in older patients, those with pre-existing CVD, and severe COVID-19 pneumonia
- CMR studies in post-COVID patients (including athletes) demonstrate myocardial oedema/fibrosis in 30–60% even after mild infection
- Predominantly affects males aged 12–30 years; highest risk after dose 2 of BNT162b2 (Comirnaty®) or mRNA-1273 (Spikevax®)
- Onset typically 1–7 days post-vaccination (median 2–3 days)
- Australian TGA data: ~30 cases per 100,000 doses in males 12–17 years; ~15 per 100,000 in males 18–29 years
- Typically mild (LVEF >50% in >90%) with excellent prognosis; resolution of symptoms in 1–7 days; recovery of LV function in >95% at 3–6 months
- ACIP/ATAGI recommendation: benefit–risk favours vaccination; consider extended dosing interval (8 weeks) for those at higher risk of myocarditis
Management Strategies
Management of myocarditis depends on the clinical severity, aetiology (viral vs immune-mediated), and haemodynamic status. The majority of patients with acute lymphocytic myocarditis are managed supportively, while specific subtypes (giant-cell, eosinophilic, sarcoidosis) require targeted immunosuppression or immunomodulation.
Supportive Care (First-Line for All Patients)
Pharmacotherapy — Heart Failure Management
Immunosuppression — Indications and Regimens
| Myocarditis Subtype | First-Line Immunosuppression | Second-Line / Steroid-Sparing | Duration |
|---|---|---|---|
| Giant-Cell Myocarditis | Methylprednisolone 1 g IV daily × 3 days → Prednisolone 1 mg/kg/day PO (max 60 mg) taper over 6 months | Ciclosporin 3–5 mg/kg/day (trough 150–300 ng/mL) OR azathioprine 2 mg/kg/day + anti-thymocyte globulin (ATG) for refractory cases | Lifelong immunosuppression required; early transplant evaluation |
| Eosinophilic Myocarditis | Methylprednisolone 500–1000 mg IV daily × 3 days → Prednisolone 1 mg/kg/day taper over 2–3 months | Mepolizumab 300 mg SC every 4 weeks (for EGPA); azathioprine; ciclosporin | 6–12 months minimum; lifelong if underlying eosinophilic disorder |
| Cardiac Sarcoidosis | Prednisolone 0.5–1 mg/kg/day (max 40 mg) for 4–8 weeks, then taper to 5–10 mg/day over 6–12 months | Methotrexate 10–20 mg/week, azathioprine 2 mg/kg/day, mycophenolate 1–1.5 g BD; consider infliximab for refractory disease | Minimum 12–24 months; often lifelong steroid-sparing therapy |
| ICI-Related Myocarditis | Stop ICI immediately; Methylprednisolone 1–2 g IV daily × 3–5 days → Prednisolone 1–2 mg/kg/day taper over 4–6 weeks | Abatacept (for fulminant cases), mycophenolate, infliximab, anti-thymocyte globulin | Corticosteroids for minimum 4–6 weeks; may require longer taper |
Immunomodulation — Adjunctive Therapies
Mechanical Circulatory Support (MCS)
Fulminant myocarditis with refractory cardiogenic shock may require mechanical circulatory support as a bridge to recovery or to transplantation. Early recognition and transfer to a transplant-capable centre are critical. Australian ECMO-capable centres include The Alfred (Melbourne), Royal Prince Alfred (Sydney), St Vincent's (Sydney), Prince Charles Hospital (Brisbane), Fiona Stanley Hospital (Perth), and Royal Adelaide Hospital.
| MCS Modality | Indication | Key Features | Australian Availability |
|---|---|---|---|
| IABP (Intra-Aortic Balloon Pump) | Cardiogenic shock with adequate but depressed LV function | Provides counterpulsation; improves coronary perfusion; limited in severe biventricular failure; reduces afterload | Widely available at tertiary centres |
| VA-ECMO (Veno-arterial ECMO) | Refractory cardiogenic shock; biventricular failure; cardiac arrest | Full circulatory and respiratory support; femoral or central cannulation; complications include limb ischaemia, bleeding, thromboembolism | Major cardiac transplant centres; retrieval services via state ambulance ECMO programs |
| Impella® / pVAD | Isolated LV failure; bridge to decision | Percutaneous axial flow pump; provides up to 5.5 L/min LV unloading; limited availability in Australia | Select centres only |
| Ventricular Assist Device (VAD) | Prolonged cardiogenic shock; bridge to transplant | Durable LVAD or BiVAD; requires sternotomy; complications include device thrombosis, stroke, infection, bleeding | Cardiac transplant centres (Alfred, St Vincent's, Prince Charles) |
Long-term Follow-up
Myocarditis requires structured long-term follow-up to detect incomplete recovery, progression to dilated cardiomyopathy, arrhythmic complications, and relapse. The duration and intensity of surveillance depend on the initial severity, aetiology, and LV function trajectory.
Recovery Monitoring Timeline
Exercise Restriction
Exercise restriction is a critical component of myocarditis management. Myocardial inflammation renders the myocardium electrically unstable and susceptible to catecholamine-mediated arrhythmias. The 2020 ESC Guidelines on Sports Cardiology and Exercise in Patients with Cardiovascular Disease provide the framework for return-to-activity decisions.
- Acute phase (first 3–6 months): Complete avoidance of all competitive sport and moderate-to-vigorous recreational exercise. Light daily activities (walking) are permissible once haemodynamically stable.
- 3–6 months: Re-assessment with CMR, echocardiography, Holter, and biomarkers. If LVEF has normalised, no arrhythmias, no LGE, and biomarkers are normal, graduated return to recreational exercise may begin under cardiologist guidance.
- Return to competitive sport: Requires normalisation of ALL parameters: LVEF ≥55%, no residual oedema on CMR, no significant LGE, no ventricular arrhythmias on 24–48 hour Holter, normal BNP, and satisfactory CPET. This typically occurs at 6–12 months in recovered patients.
- Persistent LV dysfunction: No competitive sport indefinitely; recreational exercise per heart failure guidelines (moderate-intensity aerobic, avoid isometric heavy lifting).
Arrhythmia Surveillance
Ventricular arrhythmias are a significant cause of morbidity and mortality in myocarditis survivors. Arrhythmia surveillance is essential throughout the recovery period and beyond.
- 24–48 hour Holter monitoring: At 3, 6, and 12 months post-diagnosis; annually thereafter for 5 years if LGE is present on CMR.
- Implantable loop recorder (ILR): Consider for patients with recurrent unexplained syncope, non-sustained VT on Holter, or suspected arrhythmia with negative standard monitoring.
- Electrophysiology study (EPS): May be considered for risk stratification in patients with LGE on CMR and non-sustained VT; positive programmed ventricular stimulation predicts future sustained arrhythmic events.
- ICD implantation: Indicated for survivors of cardiac arrest, sustained VT despite medical therapy, or LVEF ≤35% persisting beyond 3–6 months (per AHA/ACC/HRS 2017 guidelines). Primary prevention ICD in patients with LVEF 30–35% and LGE on CMR remains an individualised decision.
Chronic Sequelae
Myocarditis may lead to several long-term complications that require ongoing surveillance:
- Dilated cardiomyopathy (DCM): 20–30% of biopsy-proven myocarditis progresses to DCM over 5–10 years; ongoing guideline-directed heart failure therapy is essential; genetic testing should be considered as 30–50% of DCM has a genetic basis.
- Restrictive cardiomyopathy: Rare; more common in eosinophilic myocarditis (Löffler endocarditis) and cardiac amyloidosis (important differential).
- Recurrent myocarditis: Relapse rate approximately 10–15% for lymphocytic myocarditis; higher for giant-cell myocarditis (>50% without maintenance immunosuppression).
- Chronic pericarditis: Perimyocarditis may evolve into chronic relapsing pericarditis; colchicine prophylaxis may be beneficial.
- Stroke and thromboembolism: In patients with severe LV dysfunction (LVEF <30%) or atrial fibrillation; anticoagulation considerations per current guidelines.
- Psychological impact: Anxiety, depression, and reduced quality of life are common after myocarditis; screening with PHQ-9 and GAD-7 is recommended; referral to cardiac rehabilitation programs improves outcomes.
Special Populations
📚 References
- 1. Caforio ALP, Pankuweit S, Arbustini E, et al. Current state of knowledge on aetiology, diagnosis, management, and therapy of myocarditis: a position statement of the European Society of Cardiology Working Group on Myocardial and Pericardial Diseases. Eur Heart J. 2013;34(33):2636-2648.
- 2. Ferreira VM, Schulz-Menger J, Holmvang G, et al. Cardiovascular magnetic resonance in nonischemic myocardial inflammation: expert recommendations. J Am Coll Cardiol. 2018;72(24):3158-3176. (2018 Lake Louise Criteria)
- 3. Ammirati E, Frigerio M, Adler ED, et al. Management of acute myocarditis and chronic inflammatory cardiomyopathy: an expert consensus document. Circ Heart Fail. 2020;13(11):e007405.
- 4. Pellicia A, Sharma S, Gati S, et al. 2020 ESC Guidelines on sports cardiology and exercise in patients with cardiovascular disease. Eur Heart J. 2021;42(1):17-96.
- 5. Oster ME, Shay DK, Su JR, et al. Myocarditis cases reported after mRNA-based COVID-19 vaccination in the US from December 2020 to August 2021. JAMA. 2022;327(4):331-340.
- 6. Bozkurt B, Kamat I, Hotez PJ. Myocarditis with COVID-19 mRNA vaccines. Circulation. 2021;144(6):471-484.
- 7. Al-Khatib SM, Stevenson WG, Ackerman MJ, et al. 2017 AHA/ACC/HRS guideline for management of patients with ventricular arrhythmias and the prevention of sudden cardiac death. Circulation. 2018;138(13):e272-e391.
- 8. Maisch B, Pankuweit S. Standard and aetiology-directed treatment of inflammatory cardiomyopathies — ESC Working Group position statement. Eur Heart J. 2023;44(35):3360-3374.
- 9. Grün S, Schumm J, Greulich S, et al. Long-term follow-up of biopsy-proven viral myocarditis: predictors of mortality and incomplete recovery. J Am Coll Cardiol. 2012;59(18):1604-1615.
- 10. Heymans S, Eriksson U, Lehtonen J, Cooper LT. The quest for new approaches in myocarditis and inflammatory cardiomyopathy. J Am Coll Cardiol. 2016;68(21):2348-2364.
- 11. Cardiac Society of Australia and New Zealand (CSANZ). Position statement on the investigation and management of myocarditis. Heart Lung Circ. 2021;30(7):963-973.
- 12. Australian Institute of Health and Welfare (AIHW). Aboriginal and Torres Strait Islander Health Performance Framework 2023 Summary Report. Canberra: AIHW; 2023.
- 13. Sagar S, Liu PP, Cooper LT. Myocarditis. Lancet. 2012;379(9817):738-747.
- 14. National Centre for Immunisation Research and Surveillance (NCIRS). COVID-19 vaccine safety reports: Myocarditis and pericarditis following COVID-19 vaccination. Sydney: NCIRS; 2023.
- 15. Bonaca MP, Olenchock BA, Salem JE, et al. Myocarditis in the setting of cancer therapeutics: proposed case definitions for emerging clinical syndromes in cardio-oncology. Circulation. 2019;140(2):80-91. (ICI-related myocarditis)