📋 Key Information Summary
- Rheumatic heart disease (RHD) remains the most common cause of mitral stenosis (MS) worldwide and disproportionately affects Aboriginal and Torres Strait Islander Australians, particularly in remote Northern Territory and Far North Queensland communities.
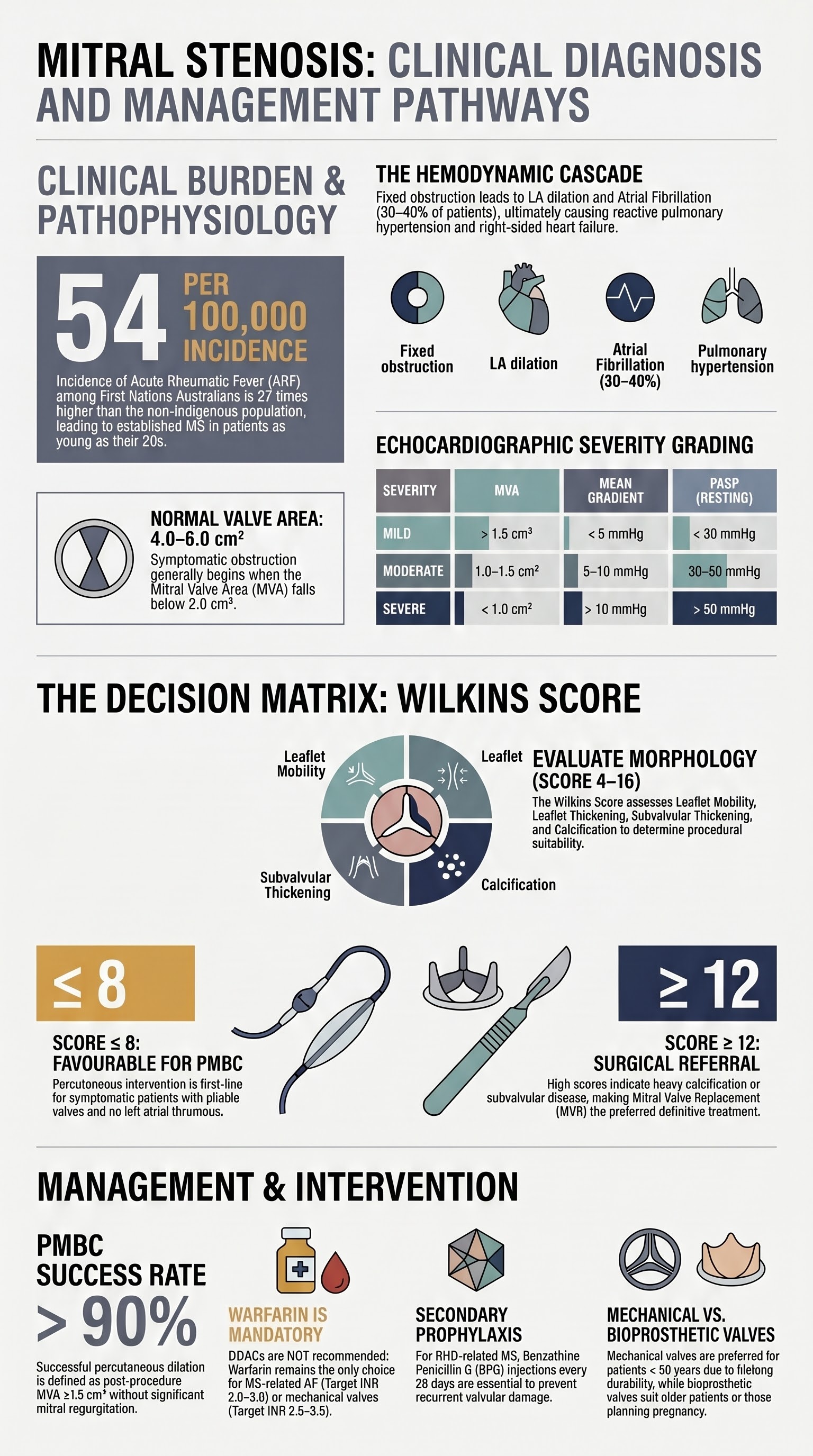
- Normal mitral valve area (MVA) is 4.0–6.0 cm²; mild MS is MVA >1.5 cm², moderate MS 1.0–1.5 cm², and severe MS <1.0 cm² (or <1.5 cm² with symptoms).
- Mean transmitral gradient ≥5 mmHg at normal heart rate defines haemodynamically significant stenosis; pulmonary artery systolic pressure (PASP) ≥50 mmHg at rest indicates severe disease.
- Atrial fibrillation (AF) develops in 30–40% of patients with significant MS and is a major driver of thromboembolism — rate control and anticoagulation are essential.
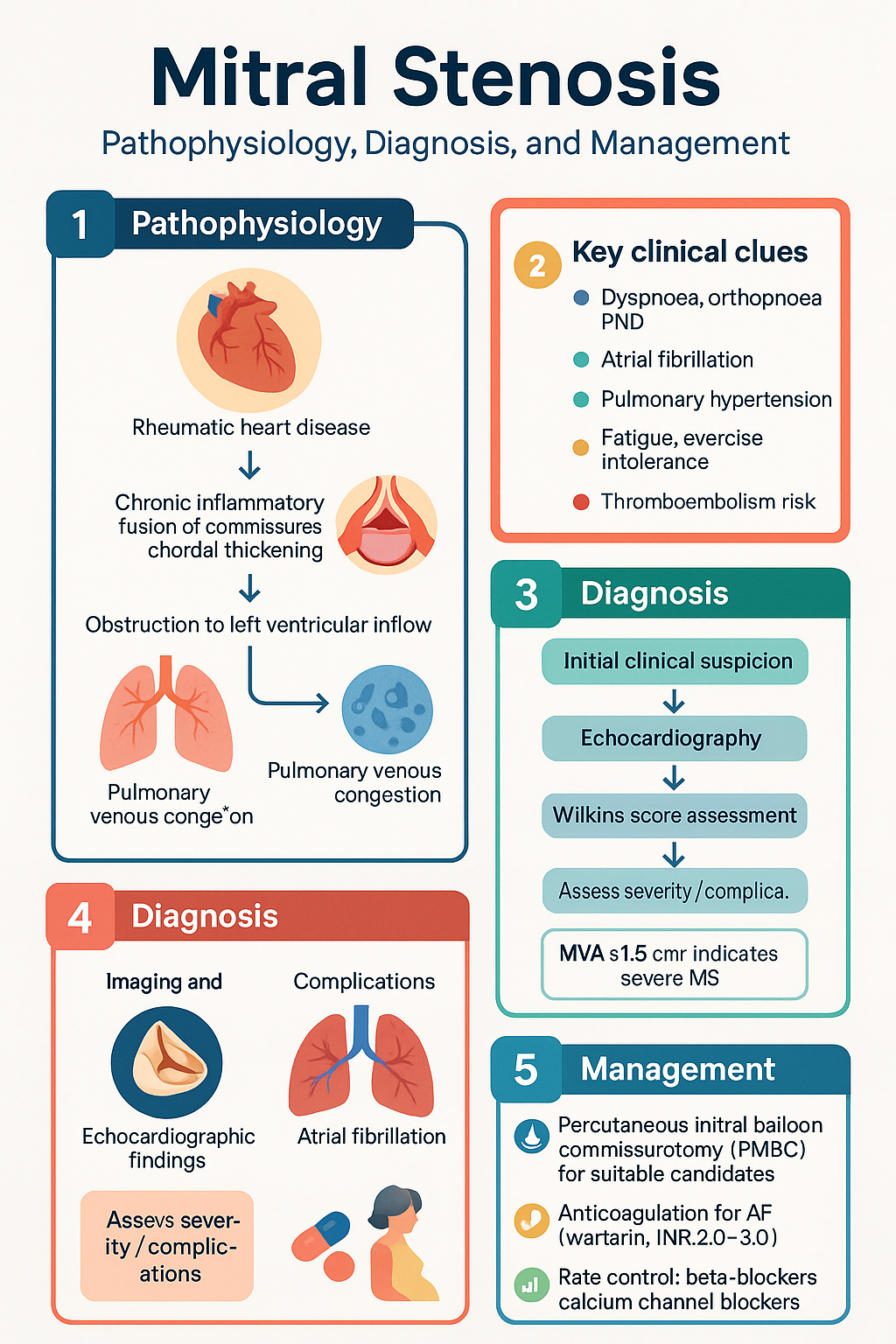
- Percutaneous mitral balloon commissurotomy (PMBC) is first-line intervention for symptomatic patients with favourable valve morphology (Wilkins score ≤8).
- PMBC success is defined as post-procedure MVA ≥1.5 cm² without more than mild mitral regurgitation (MR); procedural success exceeds 90% in experienced Australian centres.
- Mitral valve replacement (MVR) is indicated when PMBC is unsuitable (Wilkins score ≥9, significant MR, left atrial thrombus) or when concomitant surgical pathology exists.
- Mechanical prostheses are preferred in patients <60 years who can maintain lifelong anticoagulation; bioprosthetic valves suit older patients or those with contraindications to warfarin.
- Diuretics (frusemide, spironolactone) provide symptomatic relief in congestive symptoms; beta-blockers or non-dihydropyridine calcium channel blockers are first-line for rate control in AF with MS.
- Women with moderate-to-severe MS require preconception counselling; pregnancy significantly increases cardiac output and risk of pulmonary oedema and arrhythmias.
- Anticoagulation with warfarin (INR 2.0–3.0 for AF; 2.5–3.5 for mechanical valves) is mandatory; DOACs are not recommended for MS-related AF.
- All patients with RHD-related MS must be enrolled in an RHD control programme per jurisdictional guidelines (e.g., NT Rheumatic Heart Disease Control Programme).
Introduction & Australian Epidemiology
Mitral stenosis (MS) is a narrowing of the mitral valve orifice that obstructs left ventricular inflow during diastole, resulting in elevated left atrial pressure, pulmonary venous congestion, and ultimately right heart failure. Although rheumatic heart disease (RHD) has become rare in high-income nations due to improvements in living conditions and access to antibiotics, it persists as a significant burden in low- and middle-income countries and among disadvantaged populations in Australia.
In Australia, the burden of RHD — and consequently MS — is overwhelmingly concentrated among Aboriginal and Torres Strait Islander peoples. The Australian Institute of Health and Welfare (AIHW) reports that the incidence of acute rheumatic fever (ARF) among First Nations Australians is approximately 54 per 100,000, compared with <2 per 100,000 in the non-Indigenous population. The Northern Territory records the highest notification rates globally, with children aged 5–14 years most affected. Recurrent ARF accelerates valvular damage, and many patients present with established RHD including MS in their 20s–40s — a stark contrast to the degenerative and congenital aetiologies seen in non-Indigenous populations.
Congenital mitral stenosis is rare and typically presents in infancy or early childhood, often as part of a complex including parachute mitral valve, Shone syndrome, or other left-sided obstructive lesions. Prosthetic valve stenosis — either due to pannus ingrowth, thrombus formation, or calcification of bioprosthetic leaflets — constitutes an increasingly recognised cause in an ageing population with prior valve surgery.
Etiology & Pathophysiology
Causes of Mitral Stenosis
| Aetiology | Mechanism | Australian Context |
|---|---|---|
| Rheumatic heart disease (>90% globally) | Chronic inflammatory fusion of commissures, chordal thickening and shortening, leaflet calcification | Leading cause in First Nations Australians; peak onset 20–40 years; often diagnosed late |
| Congenital MS | Parachute mitral valve, double-orifice valve, supravalvular ring, hypoplastic annulus | Rare; presents in infancy; often associated with Shone complex |
| Prosthetic valve stenosis | Thrombus, pannus, calcification (bioprosthetic), tissue ingrowth | Increasing prevalence with ageing surgical population |
| Severe annular calcification | Mitral annular calcification (MAC) encroaching on leaflets | Elderly patients, those with CKD, and metabolic bone disease |
| Infiltrative / mass lesions | Left atrial myxoma, Libman-Sacks vegetations (SLE), carcinoid | Rare; requires high index of suspicion |
Rheumatic Heart Disease — Pathophysiology of MS
Acute rheumatic fever (ARF) results from an aberrant immune response to Group A Streptococcus (GAS) pharyngitis. Molecular mimicry between GAS M-protein epitopes and cardiac tissue antigens triggers T-cell mediated inflammation of valvular endothelium (verrucae), leading to Aschoff bodies and chronic scarring. Repeated episodes of ARF produce progressive commissural fusion, chordal shortening and fusion, and leaflet fibrosis and calcification — the hallmarks of chronic RHD with MS.
The normal mitral valve orifice measures 4.0–6.0 cm². Symptomatic obstruction generally occurs when MVA falls below 2.0 cm². The pathophysiological cascade includes:
- Fixed obstruction to LV inflow → elevated left atrial (LA) pressure to maintain cardiac output
- LA pressure elevation → LA dilation → atrial fibrillation (AF develops in 30–40%)
- Passive pulmonary venous congestion → dyspnoea, orthopnoea, PND
- Reactive pulmonary arterial vasoconstriction → pulmonary arterial hypertension (PAH)
- Right ventricular pressure overload → RV dilatation → tricuspid regurgitation → right heart failure
- Low cardiac output → fatigue, exercise intolerance, and eventual systemic hypoperfusion
Haemodynamic Consequences
The transmitral pressure gradient is determined by the Gorlin hydraulic equation and depends on both valve area and transvalvular flow. Tachycardia shortens diastolic filling time, disproportionately raising LA pressure in MS. This explains why:
- Exercise, pregnancy, fever, and AF with rapid ventricular response precipitate acute pulmonary oedema in MS patients
- Heart rate control is a critical therapeutic target
- MS is a preload-dependent lesion — excessive diuresis or vasodilation can cause haemodynamic collapse
Severity Grading
Echocardiography is the primary diagnostic and monitoring tool for MS. Severity is classified by valve area, transmitral gradient, and pulmonary artery pressures. The Wilkins score (also known as the echo score) is used to assess suitability for percutaneous mitral balloon commissurotomy (PMBC).
Echocardiographic Severity Classification
Wilkins Echocardiographic Score (for PMBC Suitability)
The Wilkins score evaluates four parameters on transthoracic echocardiography, each scored 1–4. A total score ≤8 predicts favourable PMBC outcomes; a score ≥9 suggests poor commissurotomy results and favours surgical intervention.
| Parameter | Score 1 | Score 2 | Score 3 | Score 4 |
|---|---|---|---|---|
| Leaflet mobility | Normal mobility; only leaflet tips restricted | Mid and base leaflets have reduced mobility | Diastolic forward movement of base and mid portions | No forward movement of any leaflet segment |
| Leaflet thickening | Normal thickness (4–5 mm) | Mid-leaflet thickening; edges 5–8 mm | Thickening extends through entire leaflet (5–8 mm) | Marked thickening of all tissue (>8–10 mm) |
| Subvalvular thickening | Minimal chordal thickening | Thickening of chordae in proximal third | Thickening extends to distal third of chordae | Extensive thickening and shortening of all chordae to papillary muscles |
| Calcification | Single area of bright echo | Scattered bright echoes at leaflet margins | Bright echoes extending to mid-leaflet | Extensive echoes through most of leaflet tissue |
Additional Echocardiographic Assessments
- Planimetry of MVA — Direct measurement at the tips of the mitral leaflets in parasternal short-axis view; most accurate echo method (±0.2 cm²)
- Pressure half-time (PHT) — PHT (ms) ÷ 220 = MVA estimate; less reliable in patients with significant aortic regurgitation, reduced LV compliance, or post-PMBC
- Continuity equation MVA — Useful when PHT is unreliable
- 3D echo planimetry — Increasingly available; provides en-face view for precise MVA measurement
- TOE — Mandatory before PMBC to exclude LA/LAA thrombus and assess commissural calcification
- Exercise stress echocardiography — Identifies exercise-induced elevation in mean gradient (≥15 mmHg) and PASP (≥60 mmHg); useful for patients with discrepancy between symptoms and resting haemodynamics
Percutaneous Mitral Balloon Commissurotomy (PMBC)
Percutaneous mitral balloon commissurotomy (PMBC), also known as percutaneous mitral valvuloplasty, is the preferred intervention for symptomatic moderate-to-severe MS with favourable valve morphology. It is performed via transseptal puncture under fluoroscopic and echocardiographic guidance, typically using the Inoue balloon technique.
Indications for PMBC
Patient Selection — Key Criteria
| Favourable for PMBC | Unfavourable for PMBC |
|---|---|
| Wilkins score ≤8 | Wilkins score ≥12 (or ≥9 with heavy calcification) |
| No more than mild MR | Moderate or severe MR |
| No LA/LAA thrombus | LA/LAA thrombus despite anticoagulation |
| Predominant commissural fusion | Predominant subvalvular disease with immobile leaflets |
| Younger patients with pliable valves | Severe calcification of both commissures |
| No concomitant surgical indication | Concomitant aortic valve or coronary disease requiring surgery |
Procedural Outcomes and Success Rates
PMBC achieves successful valve dilation (MVA ≥1.5 cm² without significant MR) in >90% of patients with favourable valve morphology. Immediate haemodynamic benefits include:
- Increase in MVA by 50–100% (typically from 1.0 cm² to 1.8–2.2 cm²)
- Reduction in mean transmitral gradient by 50%
- Reduction in LA and pulmonary artery pressures
- Symptomatic improvement in >85% of patients at 1 year
- Event-free survival (freedom from death, repeat intervention, or NYHA III–IV) of approximately 80–90% at 7 years
Complications of PMBC
| Complication | Incidence | Management |
|---|---|---|
| Severe MR (≥3+) | 2–5% | May require emergency MVR; risk reduced by stepwise balloon sizing |
| Cardiac tamponade | 0.5–1% | Pericardiocentesis; surgical repair if unresponsive |
| Systemic embolisation (stroke) | 0.5–2% | Pre-procedural TOE essential; intra-procedural heparinisation |
| Residual ASD | 20–40% (small, haemodynamically insignificant) | Most close spontaneously; large shunts (Qp:Qs >1.5) may need device closure |
| Arrhythmias | 5–10% | Transient AF common; ventricular arrhythmias rare |
| In-hospital mortality | <1% | Procedure-related mortality very low in experienced centres |
Surgical Intervention
Indications for Mitral Valve Replacement (MVR)
Surgical mitral valve replacement (or rarely, open mitral commissurotomy) is indicated when percutaneous intervention is unsuitable or has failed. Open surgical commissurotomy retains a role in selected patients where PMBC is unavailable or when concomitant surgery is required.
Open Mitral Commissurotomy vs Mitral Valve Replacement
| Factor | Open Commissurotomy | Mitral Valve Replacement |
|---|---|---|
| Ideal candidate | Young patients with predominantly commissural fusion; pliable subvalvular apparatus | Severely distorted valve; heavy calcification; subvalvular fibrosis; failed PMBC |
| Advantage | Preserves native valve; avoids prosthetic complications; no anticoagulation required | Definitive treatment; durable; effective for complex anatomy |
| Disadvantage | Higher restenosis rate (10–20% at 10 years); limited by valve morphology | Requires anticoagulation (mechanical) or limited durability (bioprosthetic); prosthetic complications |
| Operative mortality | 1–2% | 2–5% (higher with redo surgery, LV dysfunction, or emergency) |
Mechanical vs Bioprosthetic Valve Selection
Valve choice requires shared decision-making involving the patient, cardiac surgeon, and cardiologist. Key considerations include age, bleeding risk, reproductive plans, compliance with anticoagulation monitoring, and patient preference.
Transcatheter Mitral Valve Replacement (TMVR)
TMVR (e.g., Tendyne™, Intrepid™) is an emerging option primarily studied in patients with failed surgical bioprosthetic valves (valve-in-valve) or severe mitral annular calcification (valve-in-MAC). It is not yet standard therapy for native valve MS and remains largely confined to clinical trials and compassionate-use cases at select Australian centres. Multidisciplinary heart team evaluation is essential.
Medical Management
Medical therapy for MS is palliative — it controls symptoms and prevents complications but does not reverse valve obstruction. Intervention (PMBC or surgery) is the only definitive treatment for significant MS. Medical management is appropriate for asymptomatic mild MS, patients awaiting intervention, and those who are not candidates for any procedural approach.
Rate Control in Atrial Fibrillation
AF occurs in 30–40% of MS patients and is poorly tolerated due to loss of atrial kick (which contributes 20–30% of LV filling in MS) and the tendency for rapid ventricular response to exacerbate pulmonary congestion. Heart rate control is a fundamental therapeutic goal.
Diuretics for Congestive Symptoms
Diuretics provide symptomatic relief in patients with elevated pulmonary venous pressures. Caution is required — excessive diuresis reduces preload, which can critically lower cardiac output in this preload-dependent lesion.
Anticoagulation
Anticoagulation is a cornerstone of management in MS, particularly in the presence of AF, prior thromboembolism, or an enlarged left atrium (>55 mm).
Rhythm Control Considerations
In selected patients with symptomatic AF despite adequate rate control, rhythm control may be considered after successful PMBC or valve replacement that has reduced LA pressure. Amiodarone is the preferred antiarrhythmic for maintaining sinus rhythm in structural heart disease.
Secondary Prophylaxis for RHD
All patients with rheumatic heart disease — including those with established MS — must receive secondary prophylaxis to prevent recurrent ARF and progressive valvular damage.
Endocarditis Prophylaxis
Current Australian (Therapeutic Guidelines) and international (AHA/ESC) guidelines do not recommend routine antibiotic prophylaxis for infective endocarditis in patients with native valve MS. Prophylaxis may be considered for patients with prosthetic valves or prior endocarditis undergoing high-risk dental procedures. Patients with RHD-related MS should be counselled about good dental hygiene and regular dental reviews.
Special Populations
Pregnancy
Haemodynamic impact: Pregnancy increases cardiac output by 30–50% and heart rate by 10–20 bpm. The fixed obstruction of MS makes patients extremely vulnerable to pulmonary oedema, particularly during the second trimester and peripartum period.
Preconception counselling: Women with moderate-to-severe MS should be counselled before conception. PMBC should be considered prior to pregnancy if valve morphology is favourable.
Anticoagulation: Warfarin is teratogenic (nasal hypoplasia, stippled epiphyses — warfarin embryopathy) especially in weeks 6–12. Options:
- Warfarin throughout pregnancy (INR 2.5–3.5) for mechanical valve patients — highest maternal safety but foetal risk
- LMWH (enoxaparin 1 mg/kg SC BD, dose-adjusted to anti-Xa 0.8–1.2 U/mL) in first trimester, then switch to warfarin
- UFH IV for peripartum period (stop 4–6 hrs before delivery)
Rate control: Beta-blockers (metoprolol, atenolol) are preferred. Avoid atenolol in first trimester if possible (foetal growth restriction concern). Digoxin is safe.
Diuretics: Use lowest effective dose; avoid volume depletion. Frusemide is Category C.
Delivery: Vaginal delivery preferred with short second stage (instrumental delivery). Epidural analgesia recommended (reduces pain-related tachycardia). Haemodynamic monitoring in labour.
PMBC in pregnancy: Can be performed in the second trimester in experienced centres with foetal shielding and minimal fluoroscopy if medical therapy fails.
Risk classification (modified WHO): Mild MS — WHO II (low risk); moderate MS — WHO III (high risk); severe MS — WHO IV (very high risk — pregnancy contraindicated).
Paediatrics
Congenital MS: Presents in infancy with failure to thrive, tachypnoea, recurrent chest infections, and pulmonary oedema. Often associated with other left-sided obstructive lesions (Shone complex).
RHD in children: In Australian First Nations communities, ARF may occur as young as 5 years. Severe MS may develop by adolescence if secondary prophylaxis is inadequate.
Management: PMBC can be performed in children with acquired RHD-related MS and favourable morphology. Surgical commissurotomy or MVR may be required for congenital MS. Bioprosthetic valves are preferred in growing children (avoid mechanical if possible) though durability is limited.
Dosing: BPG 600,000 units IM every 28 days for children <30 kg; 1.2 million units for ≥30 kg. Warfarin dosing requires careful titration with frequent INR monitoring; consider the Australasian Kardiology consortium guidelines.
Key concern: Children in remote communities face significant barriers to regular BPG injections and cardiology follow-up. Rheumatic heart disease registers and recall systems are critical.
Elderly
Aetiology: In non-Indigenous elderly Australians, MS is more likely due to severe mitral annular calcification (MAC) than RHD. Prosthetic valve degeneration is increasingly common.
Comorbidities: AF, CKD, coronary artery disease, and frailty complicate management. Bleeding risk is higher on anticoagulation — use HAS-BLED score to assess.
Rate control: Beta-blockers preferred but monitor for bradycardia, falls, and fatigue. Diltiazem/verapamil are alternatives if beta-blockers not tolerated.
Intervention: PMBC may still be feasible if valve morphology is favourable. For those with significant comorbidities, surgical risk assessment using EuroSCORE II or STS score is essential. Bioprosthetic valve preferred if MVR required (avoids lifelong warfarin; limited life expectancy makes valve durability less critical).
Warfarin management: More frequent INR monitoring recommended; aim lower end of target range if bleeding risk elevated.
Renal Impairment
Diuretics: Frusemide dose requirements increase with declining eGFR (up to 250 mg IV in severe CKD). Monitor electrolytes closely — loop diuretics cause hypokalaemia, thiazides potentiate this.
Warfarin: No dose adjustment required; however INR variability increases in CKD. Calciphylaxis risk with warfarin in dialysis patients — consider alternatives where possible.
Digoxin: Significant renal adjustment required; reduce dose by 50% if eGFR 10–30; 62.5 mcg daily or alternate days if eGFR <10. Monitor serum levels (target 0.5–0.9 ng/mL).
MAC-related MS: Severe calcification is more common in CKD and dialysis patients, making PMBC technically challenging.
Specialist input: Nephrology co-management recommended for patients on dialysis or with eGFR <30 mL/min.
Hepatic Impairment
Warfarin sensitivity: Liver disease reduces synthesis of clotting factors, increasing INR sensitivity. Start at lower doses (1–2 mg daily) and titrate cautiously. Monitor LFTs.
Spironolactone: Useful in patients with concurrent hepatic congestion or ascites; however, hyperkalaemia risk increases. Avoid if eGFR <30 or K⁺ >5.0.
Amiodarone: Hepatotoxic — contraindicated in severe liver disease. Monitor LFTs at baseline, 6 months, then annually.
Key consideration: Congestive hepatopathy from right heart failure may elevate INR independently of warfarin effect. Interpret INR cautiously.
Immunocompromised
Infective endocarditis risk: Immunosuppressed patients (transplant recipients, HIV, chemotherapy) with MS are at higher risk of endocarditis if bacteraemia occurs. Maintain vigilant dental hygiene and promptly treat infections.
RHD overlap: Immunosuppressed patients with RHD should continue BPG secondary prophylaxis — immunosuppression does not affect GAS recurrence risk but may mask ARF presentations.
Amiodarone: Pulmonary toxicity (pneumonitis) is more difficult to distinguish from opportunistic infections in immunocompromised patients. Use lowest effective dose and monitor with serial chest imaging.
Prosthetic valve infection: If MVR has been performed, prosthetic valve endocarditis carries high mortality; early infectious diseases consultation is essential.
Aboriginal and Torres Strait Islander Health Considerations
Mitral stenosis in Aboriginal and Torres Strait Islander Australians is overwhelmingly a consequence of rheumatic heart disease (RHD), a disease of poverty, overcrowding, and inequitable access to healthcare. RHD-related MS presents at a younger age, progresses more rapidly, and carries significantly worse outcomes in First Nations Australians compared with the non-Indigenous population. Addressing MS in this context requires a holistic, culturally safe approach that extends beyond the valve lesion to encompass social determinants of health, secondary prophylaxis adherence, and community engagement.
Epidemiology and Disease Burden
- Aboriginal and Torres Strait Islander Australians experience ARF at rates 20–60 times higher than non-Indigenous Australians
- The highest ARF and RHD notification rates are in the Northern Territory, Far North Queensland, and Western Australia
- RHD is the leading cause of acquired heart disease in First Nations children and young adults
- First Nations Australians with RHD are diagnosed with severe MS approximately 15–20 years younger than non-Indigenous patients with degenerative or calcific MS
- Mortality from RHD in First Nations Australians remains 5–10 times higher than in non-Indigenous Australians
Barriers to Optimal Management
Recommended Actions for Clinicians
- Register all RHD patients on the jurisdictional RHD register (e.g., NT RHDAustralia, QLD RHD register) to enable recall and tracking
- Ensure BPG is administered on time — liaise with community health centres, use recall systems, and explore nurse-led injection programs
- Provide culturally safe care — engage Aboriginal health workers/ practitioners; use interpreter services for patients whose first language is not English; accommodate cultural obligations
- Screen household contacts — siblings and household members of ARF/RHD cases should be offered GAS screening and treatment
- Advocate for upstream interventions — support housing, hygiene, and community infrastructure programs that reduce GAS transmission
- Plan for intervention early — refer for PMBC or surgery before severe PAH and RV failure develop; delays in referral contribute to worse outcomes
- Use telehealth for echocardiographic surveillance and specialist cardiology review to reduce the burden of travel
📚 References
- 1. Vahanian A, Beyersdorf F, Praz F, et al. 2020 ESC/EACTS Guidelines for the management of valvular heart disease. Eur Heart J. 2022;43(7):561–632. doi:10.1093/eurheartj/ehab132
- 2. RHDAustralia (ARF/RHD writing group). The 2020 Australian guideline for prevention, diagnosis and management of acute rheumatic fever and rheumatic heart disease. 3rd ed. Darwin: Menzies School of Health Research; 2020.
- 3. Australian Institute of Health and Welfare (AIHW). Rheumatic heart disease and acute rheumatic fever in Australia: 2017–2018. Cat. no. CVD 86. Canberra: AIHW; 2021.
- 4. Baumgartner H, Hung J, Bermejo J, et al. Recommendations on the echocardiographic assessment of aortic valve stenosis: a focused update from the European Association of Cardiovascular Imaging and the American Society of Echocardiography. J Am Soc Echocardiogr. 2017;30(4):372–392.
- 5. Wilkins GT, Weyman AE, Abascal VM, Block PC, Palacios IF. Percutaneous balloon dilatation of the mitral valve: an analysis of echocardiographic variables related to outcome and the mechanism of dilatation. Br Heart J. 1988;60(4):299–308.
- 6. Palacios IF, Sanchez PL, Harrell LC, Weyman AE, Block PC. Which patients benefit from percutaneous mitral balloon valvuloplasty? Prevalvuloplasty and postvalvuloplasty variables that predict long-term outcome. Circulation. 2002;105(12):1465–1471.
- 7. Nishimura RA, Otto CM, Bonow RO, et al. 2017 AHA/ACC Focused Update of the 2014 AHA/ACC Guideline for the Management of Patients with Valvular Heart Disease. Circulation. 2017;135(25):e1159–e1195.
- 8. Carapetis JR, Steer AC, Mulholland EK, Weber M. The global burden of group A streptococcal diseases. Lancet Infect Dis. 2005;5(11):685–694.
- 9. National Heart Foundation of Australia and Cardiac Society of Australia and New Zealand. Guidelines for the prevention, detection and management of chronic heart failure in Australia. Updated 2024.
- 10. Iung B, Baron G, Butchart EG, et al. A prospective survey of patients with valvular heart disease in Europe: the Euro Heart Survey on Valvular Heart Disease. Eur Heart J. 2003;24(13):1231–1243.
- 11. Reményi B, Wilson N, Steer A, et al. World Heart Federation criteria for echocardiographic diagnosis of rheumatic heart disease — an evidence-based guideline. Nat Rev Cardiol. 2012;9(5):297–309.
- 12. Roberts K, Maguire G, Brown A, et al. Echocardiographic screening for rheumatic heart disease in high and low risk Australian children. Circulation. 2014;129(19):1953–1961.
- 13. Francis J, Bayfield H, Francis J, et al. Gaps in the management of rheumatic heart disease in Aboriginal and Torres Strait Islander peoples. Med J Aust. 2021;214(8):363–369.
- 14. Essop MR, Nkomo VT. Rheumatic and nonrheumatic valvular heart disease: epidemiology, management, and prevention in Africa. Circulation. 2005;112(23):3584–3591.