📋 Key Information Summary
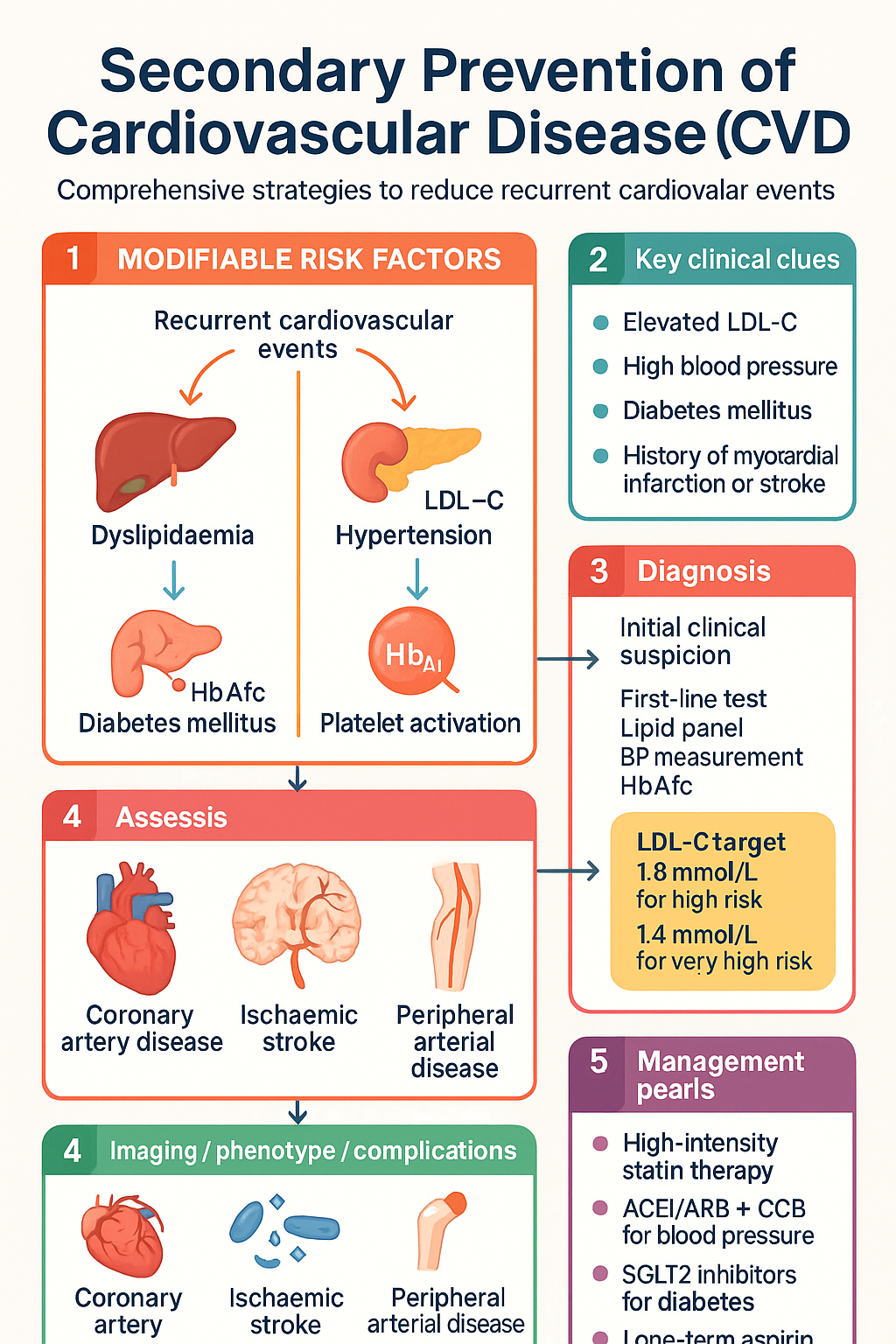
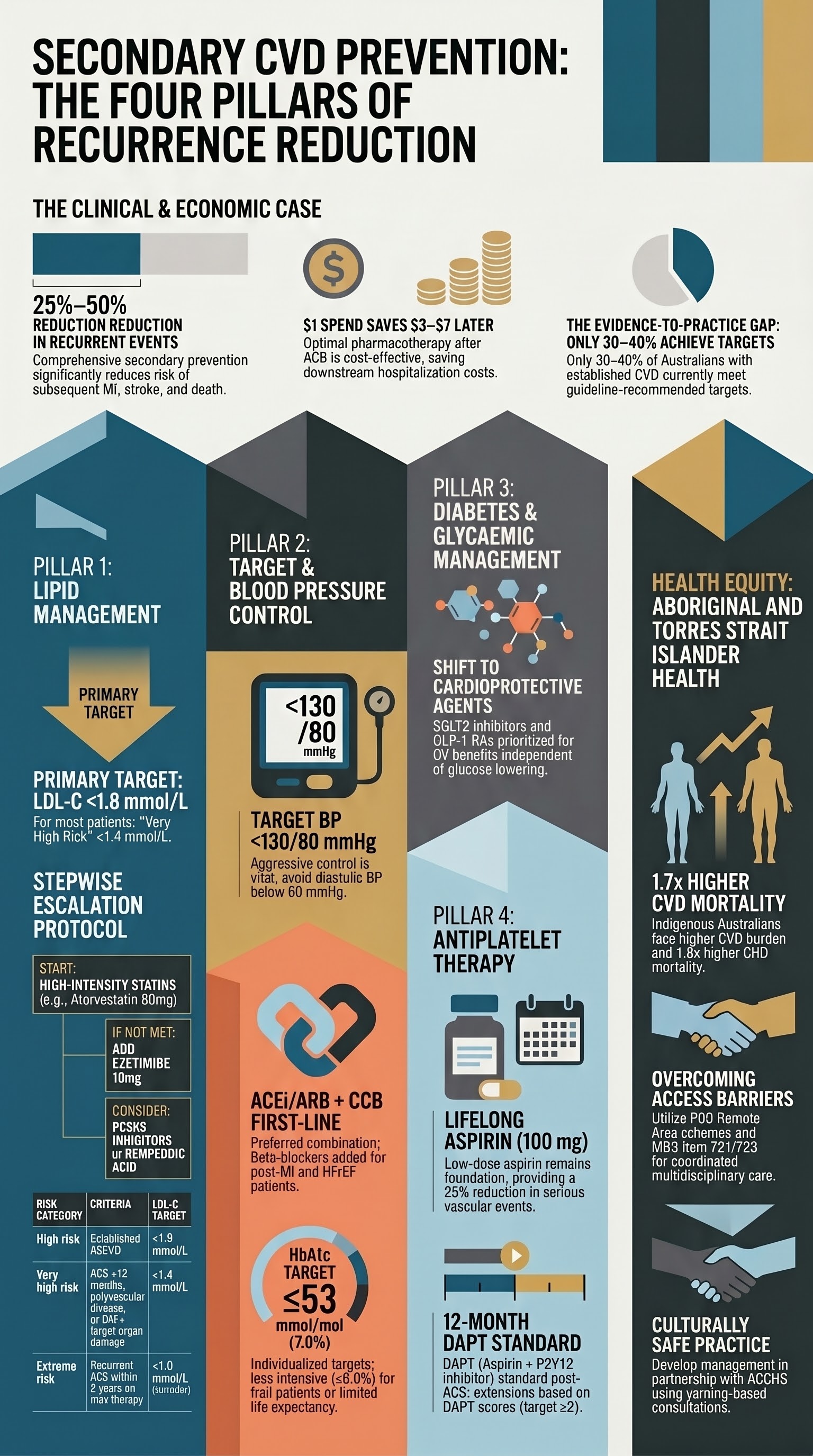
- Secondary CVD prevention reduces recurrent events by 25–50% through integrated lipid, blood pressure, glycaemic, and antiplatelet management.
- LDL-C target <1.8 mmol/L for most patients with established ASCVD; consider <1.4 mmol/L for very high-risk patients (ACS ≤12 months, polyvascular disease, or DM with target organ damage).
- High-intensity statin therapy (atorvastatin 80 mg or rosuvastatin 40 mg) is first-line; add ezetimibe if LDL-C target not achieved after 6–8 weeks.
- PCSK9 inhibitors (evolocumab, alirocumab) are indicated when maximally tolerated statin + ezetimibe fails to reach target — available on PBS Authority Required.
- Bempedoic acid (Nexletol®) is a non-statin option for statin-intolerant patients; PBS-listed with Authority Required status.
- Target BP <130/80 mmHg for secondary CVD prevention; ACEi/ARB + CCB is preferred first-line combination.
- ACE inhibitors (or ARBs) are strongly recommended post-MI, in HFrEF, and in diabetic patients; add beta-blockers for post-MI and HFrEF.
- HbA1c target ≤53 mmol/mol (7.0%) in most CVD patients with T2DM; individualise for frailty and hypoglycaemia risk.
- SGLT2 inhibitors (empagliflozin, dapagliflozin) reduce cardiovascular death and HF hospitalisation — recommended regardless of glycaemic status in patients with established CVD or HF.
- GLP-1 receptor agonists (semaglutide, liraglutide) reduce MACE in T2DM with ASCVD; preferred second-line after metformin in this population.
- Long-term aspirin 100 mg daily remains standard for secondary prevention; extended DAPT (aspirin + ticagrelor or clopidogrel) is guided by ischaemic vs bleeding risk balance.
- Aboriginal and Torres Strait Islander Australians have 1.7× the cardiovascular mortality rate of non-Indigenous Australians; culturally safe follow-up and medication access are essential.
Introduction & Australian Epidemiology
Cardiovascular disease (CVD) remains the leading cause of death in Australia, responsible for approximately 42,900 deaths in 2022 and accounting for 25% of all deaths nationally. Patients who survive an acute cardiovascular event — myocardial infarction (MI), ischaemic stroke, or peripheral arterial disease (PAD) — face a substantially elevated risk of recurrent events. Evidence consistently demonstrates that comprehensive secondary prevention reduces recurrent cardiovascular events by 25–50% and all-cause mortality by 20–30%.
Secondary prevention of CVD encompasses a multifactorial approach targeting modifiable risk factors: dyslipidaemia, hypertension, diabetes mellitus, platelet activation, smoking, physical inactivity, and obesity. The Australian Institute of Health and Welfare (AIHW) reports that only 30–40% of Australians with established CVD achieve guideline-recommended targets for lipid control, blood pressure, and glycaemic management, highlighting a significant evidence-to-practice gap.
This guideline addresses the four pillars of pharmacological secondary prevention: lipid management, blood pressure control, diabetes management, and antiplatelet therapy, with specific reference to Australian PBS availability, MBS item numbers, and national cardiovascular guidelines.
Lipid Management
LDL-C Targets in Secondary Prevention
Elevated low-density lipoprotein cholesterol (LDL-C) is the primary lipid target in secondary CVD prevention. The relationship between LDL-C and recurrent cardiovascular events is log-linear, with no lower threshold identified below which benefit ceases. Current Australian and international guidelines recommend stratified LDL-C goals based on residual cardiovascular risk.
| Risk Category | Criteria | LDL-C Target |
|---|---|---|
| High risk | Established ASCVD (prior MI, ischaemic stroke, PAD, revascularisation) | <1.8 mmol/L |
| Very high risk | ACS ≤12 months, polyvascular disease, DM + target organ damage, FH + ASCVD, recurrent events despite optimal therapy | <1.4 mmol/L |
| Extreme risk | Recurrent ACS within 2 years on maximally tolerated statin + ezetimibe, or ACS with multi-vessel disease + DM | <1.0 mmol/L (consider) |
Statin Intensity Selection
High-intensity statin therapy is the cornerstone of lipid management in secondary prevention. In Australia, the two principal high-intensity statins are atorvastatin 80 mg and rosuvastatin 40 mg. Where these doses are not tolerated (myalgia, elevated transaminases), moderate-intensity statin therapy combined with ezetimibe is preferred over low-intensity monotherapy.
Ezetimibe
Ezetimibe reduces LDL-C by inhibiting intestinal cholesterol absorption via NPC1L1 blockade. It provides an additional 15–25% LDL-C reduction when added to statin therapy and is recommended as the first add-on agent when statin monotherapy fails to achieve target. The IMPROVE-IT trial demonstrated a modest but significant reduction in cardiovascular events when ezetimibe was added to simvastatin in post-ACS patients.
PCSK9 Inhibitors
Proprotein convertase subtilisin/kexin type 9 (PCSK9) inhibitors are monoclonal antibodies that significantly reduce LDL-C by 50–70% when added to maximally tolerated statin ± ezetimibe. The FOURIER trial (evolocumab) and ODYSSEY OUTCOMES trial (alirocumab) demonstrated significant reductions in MACE in patients with established ASCVD. In Australia, PBS access requires Authority Approval and is restricted to patients with ASCVD who have not achieved target LDL-C despite maximally tolerated statin + ezetimibe.
Bempedoic Acid
Bempedoic acid (Nexletol®) is an ATP citrate lyase inhibitor that reduces LDL-C by 15–25% and is approved for use as monotherapy or add-on therapy. It is activated in the liver (not muscle), which accounts for its lower myalgia risk compared with statins. The CLEAR Outcomes trial demonstrated a 13% relative reduction in MACE in statin-intolerant patients. It is available in Australia as a combination with ezetimibe (Nexlizet®).
Lipid-Lowering Stepwise Approach
Blood Pressure Control
Blood Pressure Targets in CAD
Hypertension is the most prevalent modifiable risk factor for recurrent cardiovascular events. In patients with established coronary artery disease (CAD), ischaemic stroke, or PAD, the target blood pressure is <130/80 mmHg, consistent with the 2023 ESH guidelines, AHA/ACC guidance, and the Australian Clinical Practice Guidelines for the Management of Hypertension. A systolic target of 120–129 mmHg may be beneficial in high-risk patients if tolerated, supported by the SPRINT trial and subsequent meta-analyses.
Antihypertensive Selection in Secondary Prevention
The choice of antihypertensive agent in secondary CVD prevention is guided by comorbidities and evidence from landmark trials. ACE inhibitors (or ARBs if intolerant) are the preferred first-line agents given their mortality benefit post-MI and in heart failure with reduced ejection fraction (HFrEF). Beta-blockers have a strong evidence base post-MI and in HFrEF, while calcium channel blockers and thiazide-like diuretics are effective add-on agents.
| Drug Class | Preferred Agent | Indication in CVD | Key Considerations |
|---|---|---|---|
| ACE inhibitor | Ramipril, perindopril, enalapril | Post-MI, HFrEF, DM, CKD | Monitor K⁺ and eGFR at 1–2 weeks; contraindicated in bilateral RAS, pregnancy |
| ARB | Candesartan, valsartan, telmisartan | ACEi intolerance (cough), HFrEF, post-MI | Same monitoring as ACEi; do NOT combine with ACEi |
| Beta-blocker | Metoprolol succinate, bisoprolol, carvedilol | Post-MI (12+ months), HFrEF, rate control | Prefer evidence-based agents for HFrEF (bisoprolol, carvedilol, metoprolol succinate) |
| Calcium channel blocker | Amlodipine, lercanidipine | Add-on therapy, angina, elderly | Avoid verapamil/diltiazem in HFrEF; amlodipine safe in HFrEF |
| Thiazide-like diuretic | Indapamide, chlorthalidone | Resistant hypertension, volume overload | Monitor electrolytes (Na⁺, K⁺, uric acid); prefer indapamide in elderly |
| Mineralocorticoid receptor antagonist | Spironolactone, eplerenone | HFrEF, resistant hypertension, post-MI with LVSD | Monitor K⁺ closely; avoid if eGFR <30; gynaecomastia risk with spironolactone |
Combination Therapy Strategies
Most patients with established CVD will require ≥2 antihypertensive agents to achieve target BP. Australian guidelines recommend the following combination approaches:
- First-line combination: ACEi (or ARB) + dihydropyridine CCB (e.g., perindopril + amlodipine) — preferred in most patients with CAD
- Second-line combination: ACEi/ARB + CCB + thiazide-like diuretic — for resistant hypertension
- Third-line / resistant HT: Add spironolactone 25 mg (PATHWAY-2 trial demonstrated superiority over doxazosin and bisoprolol in resistant hypertension)
- Single-pill combinations (SPCs): Improve adherence by 20–30%. Available Australian SPCs include perindopril/amlodipine, perindopril/indapamide, irbesartan/amlodipine, and candesartan/amlodipine — all PBS-listed
- Post-MI: ACEi + beta-blocker is the foundational combination; add CCB or diuretic if BP remains above target
Diabetes Management in CVD
HbA1c Targets in Cardiovascular Disease
Diabetes mellitus confers a 2–4-fold increased risk of cardiovascular events and is present in 25–35% of patients hospitalised with acute coronary syndromes in Australia. Glycaemic management in secondary CVD prevention focuses not only on HbA1c reduction but increasingly on cardiovascular risk reduction through agent-specific effects.
The recommended HbA1c target for most patients with T2DM and established CVD is ≤53 mmol/mol (≤7.0%). This target should be individualised: less intensive targets (≤64 mmol/mol / ≤8.0%) may be appropriate for patients with limited life expectancy, significant comorbidities, recurrent severe hypoglycaemia, or advanced frailty.
SGLT2 Inhibitors — Cardiovascular Benefits
Sodium-glucose co-transporter 2 (SGLT2) inhibitors have transformed cardiovascular management in diabetes. The EMPA-REG OUTCOME, CANVAS, DECLARE-TIMI 58, and CREDENCE trials collectively demonstrated reductions in major adverse cardiovascular events (MACE), cardiovascular death, and heart failure hospitalisation. These benefits extend to patients without diabetes, as shown in DAPA-HF and EMPEROR-Reduced.
GLP-1 Receptor Agonists — Cardiovascular Outcomes
GLP-1 receptor agonists (GLP-1 RAs) have demonstrated significant reductions in MACE in patients with T2DM and established ASCVD. The LEADER trial (liraglutide) showed a 13% reduction in 3-point MACE and 22% reduction in cardiovascular death. The SUSTAIN-6 and PIONEER-6 trials established semaglutide's cardiovascular safety profile, while the SELECT trial demonstrated MACE reduction in overweight/obese patients without diabetes.
Antiplatelet Therapy
Long-Term Aspirin Therapy
Low-dose aspirin (75–100 mg daily) remains the foundation of long-term antiplatelet therapy in secondary CVD prevention. Aspirin irreversibly acetylates cyclooxygenase-1 (COX-1), inhibiting thromboxane A₂ production and platelet aggregation. Evidence from the Antithrombotic Trialists' (ATT) Collaboration meta-analysis confirms a 25% proportional reduction in serious vascular events with aspirin in secondary prevention, with benefits clearly outweighing the modest increase in major bleeding risk.
Extended Dual Antiplatelet Therapy (DAPT)
Standard DAPT following ACS consists of aspirin + a P2Y12 inhibitor (clopidogrel or ticagrelor) for 12 months. The decision to extend DAPT beyond 12 months requires careful assessment of ischaemic versus bleeding risk.
Bleeding vs Ischaemic Risk Assessment
The decision to intensify or de-escalate antiplatelet therapy requires integrated assessment using validated risk scores:
- DAPT Score: Integrates age, DM, MI at presentation, prior PCI/MI, stent diameter, smoking, CHF/LVEF <30%, paclitaxel stent, vein graft PCI. Score ≥2 favours extended DAPT.
- GRACE Score: Predicts 6-month mortality post-ACS (age, HR, SBP, creatinine, cardiac arrest, ST deviation, biomarkers, Killip class).
- Thrombolysis in Myocardial Infarction (TIMI) Risk Score: For unstable angina/NSTEMI.
- HAS-BLED: Hypertension, abnormal renal/liver function, stroke, bleeding history, labile INR, elderly (>65), drugs/alcohol. Score ≥3 = high bleeding risk.
- PRECISE-DAPT: Age, haemoglobin, WBC, creatinine clearance, prior bleeding. Score ≥25 suggests high bleeding risk and favours shorter DAPT.
- ARC-HBR: Academic Research Consortium criteria for high bleeding risk (anatomical and clinical criteria).
Antiplatelet Therapy Post-Stroke
For secondary prevention following ischaemic stroke or TIA, dual antiplatelet therapy (aspirin + clopidogrel) for 21 days followed by clopidogrel monotherapy is supported by the CHANCE and POINT trials. For long-term secondary prevention, clopidogrel 75 mg monotherapy is preferred over aspirin based on the CAPRIE trial showing superior efficacy of clopidogrel in patients with recent ischaemic events.
Investigations & Monitoring
Baseline and Ongoing Investigations
Special Populations
Pregnancy
- Statins — Contraindicated in pregnancy (Category X in Australian categorisation). Discontinue at least 1 month before planned conception or immediately upon confirmed pregnancy.
- ACEi/ARBs — Teratogenic (Category D); must be ceased before conception. Switch to methyldopa or labetalol for BP control.
- SGLT2 inhibitors — Contraindicated in pregnancy. Cease before conception.
- GLP-1 RAs — Not recommended in pregnancy; discontinue at least 2 months before planned conception (semaglutide).
- Aspirin — Low-dose (100 mg) is safe in pregnancy for pre-eclampsia prevention; continue for secondary CVD prevention if high risk, after individual risk–benefit assessment.
- Women of reproductive age with established CVD should receive pre-conception counselling and be managed jointly by cardiology and obstetric medicine.
Paediatrics
- Statins — Limited to heterozygous familial hypercholesterolaemia (FH) under specialist supervision from age 10 years. Atorvastatin 10–20 mg or rosuvastatin 5–20 mg.
- Ezetimibe — May be used from age 10 years in FH (specialist indication).
- Aspirin — Low-dose aspirin (2–5 mg/kg/day) in paediatric patients post-Kawasaki disease with coronary artery aneurysms (secondary CVD prevention in children).
- ACEi/ARBs — Use in paediatric hypertension (enalapril, losartan) with weight-based dosing; monitor growth and renal function.
- Secondary CVD prevention in paediatrics is rare and typically relates to Kawasaki disease, congenital heart disease, or FH. Always involve paediatric cardiology.
Elderly (≥75 years)
- Statins — Benefit persists but with reduced relative risk reduction. Intensity may be reduced if frailty, polypharmacy, or myalgia limit high-intensity therapy. Continue if previously tolerated.
- BP targets — Individualise; SBP <130 mmHg may cause orthostatic hypotension and falls. Consider <140/90 mmHg as pragmatic target if frail. SPRINT showed benefit in fit elderly.
- Antiplatelet therapy — Increased bleeding risk (HAS-BLED); GI protection with PPI recommended. Consider risk–benefit of continuing DAPT beyond 12 months.
- SGLT2i / GLP-1 RA — Limited data in very elderly (>80 years); use with caution, especially SGLT2i (volume depletion, falls).
- Regular medication review to reduce polypharmacy-related harm. Falls risk assessment with BP management changes.
Renal Impairment
- Statins — Atorvastatin (no renal dose adjustment) preferred in CKD. Rosuvastatin: start 5 mg, max 10 mg if eGFR <30. Pravastatin: start 10 mg in severe CKD.
- ACEi/ARBs — Essential for cardiorenal protection; monitor K⁺ and creatinine at 1–2 weeks. Accept up to 30% rise in creatinine from baseline. Avoid in bilateral renal artery stenosis.
- SGLT2i — Can be initiated at eGFR ≥20 mL/min for cardiorenal benefits. Glycaemic efficacy reduced below eGFR 45 but organ-protective benefits persist (DAPA-CKD, EMPA-KIDNEY).
- Antiplatelet agents — Increased bleeding risk in advanced CKD; no specific dose adjustments for aspirin, clopidogrel, or ticagrelor.
- Patients on dialysis have been excluded from most CVD prevention trials. Extrapolate with caution and individualise care.
Hepatic Impairment
- Statins — Contraindicated in active liver disease or unexplained persistent transaminase elevation. Use cautiously in Child-Pugh A; avoid in Child-Pugh B–C.
- Ezetimibe — Not recommended in moderate–severe hepatic impairment.
- ACEi/ARBs — Use with caution; no specific dose adjustment but monitor for hepatotoxicity (rare with ACEi).
- GLP-1 RAs — Limited data; caution in severe hepatic impairment.
- Non-alcoholic fatty liver disease (NAFLD) is common in CVD patients; statins are safe and may reduce liver fibrosis progression.
Immunocompromised
- HIV-positive patients — Higher CVD risk; statin–antiretroviral interactions (avoid simvastatin with PIs; pravastatin and atorvastatin preferred). Consult with infectious disease specialist.
- Transplant recipients — Cardiovascular disease is the leading cause of death post-transplant. Statins (pravastatin preferred in renal transplant due to lower interaction with calcineurin inhibitors). Avoid rosuvastatin with cyclosporin.
- Rheumatic disease on immunosuppression — Increased CVD risk from chronic inflammation. Statins considered safe; colchicine (0.5 mg daily) may provide dual anti-inflammatory and cardiovascular benefit (COLCOT, LoDoCo2).
- Screen for cardiovascular risk factors at baseline and regularly in all immunocompromised populations. Rheumatoid arthritis, SLE, psoriasis, and HIV are independent CVD risk equivalents.
Aboriginal and Torres Strait Islander Health
Aboriginal and Torres Strait Islander Australians experience cardiovascular disease at 1.7 times the rate of non-Indigenous Australians, with coronary heart disease mortality 1.8 times higher. The burden is particularly pronounced in remote and very remote communities, where access to specialist cardiology services, cardiac rehabilitation, and pharmacotherapy is limited. Cardiovascular disease accounts for approximately 25% of the life expectancy gap between Indigenous and non-Indigenous Australians.
Quick Reference — Secondary Prevention Targets
📚 References
- 1. Mach F, Baigent C, Catapano AL, et al. 2019 ESC/EAS Guidelines for the management of dyslipidaemias: lipid modification to reduce cardiovascular risk. Eur Heart J. 2020;41(1):111–188.
- 2. Sabatine MS, Giugliano RP, Keech AC, et al. Evolocumab and clinical outcomes in patients with cardiovascular disease (FOURIER). N Engl J Med. 2017;376(18):1713–1722.
- 3. Schwartz GG, Steg PG, Szarek M, et al. Alirocumab and cardiovascular outcomes after acute coronary syndrome (ODYSSEY OUTCOMES). N Engl J Med. 2018;379(22):2097–2107.
- 4. Cannon CP, Blazing MA, Giugliano RP, et al. Ezetimibe added to statin therapy after acute coronary syndromes (IMPROVE-IT). N Engl J Med. 2015;372(25):2387–2397.
- 5. Nissen SE, Lincoff AM, Brennan D, et al. Bempedoic acid and cardiovascular outcomes in statin-intolerant patients (CLEAR Outcomes). N Engl J Med. 2023;388(15):1353–1364.
- 6. Zinman B, Wanner C, Lachin JM, et al. Empagliflozin, cardiovascular outcomes, and mortality in type 2 diabetes (EMPA-REG OUTCOME). N Engl J Med. 2015;373(22):2117–2128.
- 7. McMurray JJV, Solomon SD, Inzucchi SE, et al. Dapagliflozin in patients with heart failure and reduced ejection fraction (DAPA-HF). N Engl J Med. 2019;381(21):1995–2008.
- 8. Marso SP, Daniels GH, Tanaka K, et al. Liraglutide and cardiovascular outcomes in type 2 diabetes (LEADER). N Engl J Med. 2016;375(4):311–322.
- 9. Marso SP, Bain SC, Consoli A, et al. Semaglutide and cardiovascular outcomes in patients with type 2 diabetes (SUSTAIN-6). N Engl J Med. 2016;375(19):1834–1844.
- 10. Bonaca MP, Bhatt DL, Cohen M, et al. Long-term use of ticagrelor in patients with prior myocardial infarction (PEGASUS-TIMI 54). N Engl J Med. 2015;372(19):1791–1800.
- 11. Wallentin L, Becker RC, Budaj A, et al. Ticagrelor versus clopidogrel in patients with acute coronary syndromes (PLATO). N Engl J Med. 2009;361(11):1045–1057.
- 12. Yusuf S, Zhao F, Mehta SR, et al. Effects of clopidogrel in addition to aspirin in patients with acute coronary syndromes without ST-segment elevation (CURE). N Engl J Med. 2001;345(7):494–502.
- 13. SPRINT Research Group, Wright JT Jr, Williamson JD, et al. A randomized trial of intensive versus standard blood-pressure control (SPRINT). N Engl J Med. 2015;373(22):2103–2116.
- 14. National Heart Foundation of Australia and Cardiac Society of Australia and New Zealand. Reducing risk in heart disease: an expert guide to clinical practice for secondary prevention of coronary heart disease. Med J Aust. 2023;218(Suppl 6):S1–S59.
- 15. Australian Institute of Health and Welfare (AIHW). Cardiovascular disease in Aboriginal and Torres Strait Islander people. AIHW Cat. No. CVD 87. Canberra: AIHW; 2023.