📋 Key Information Summary
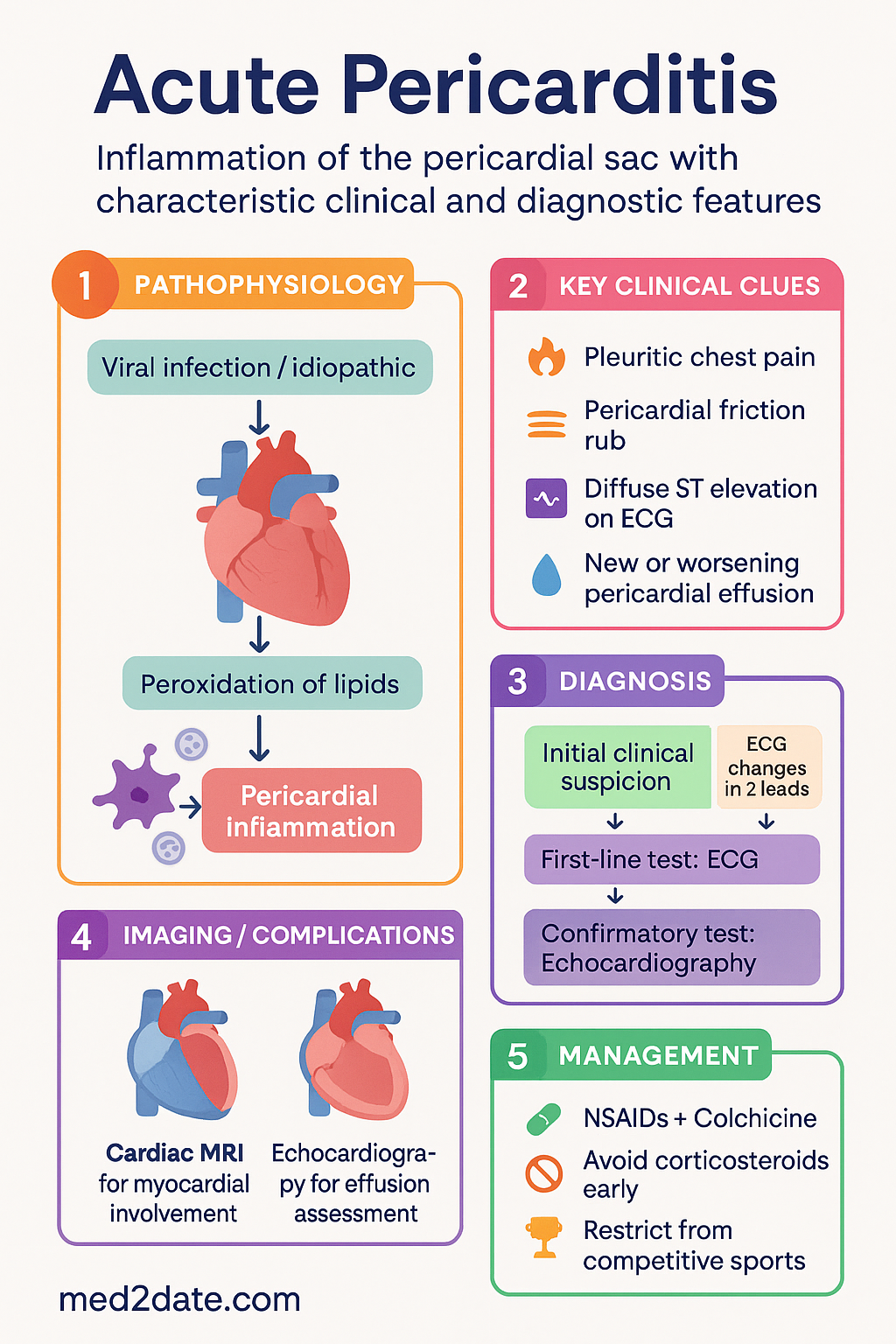
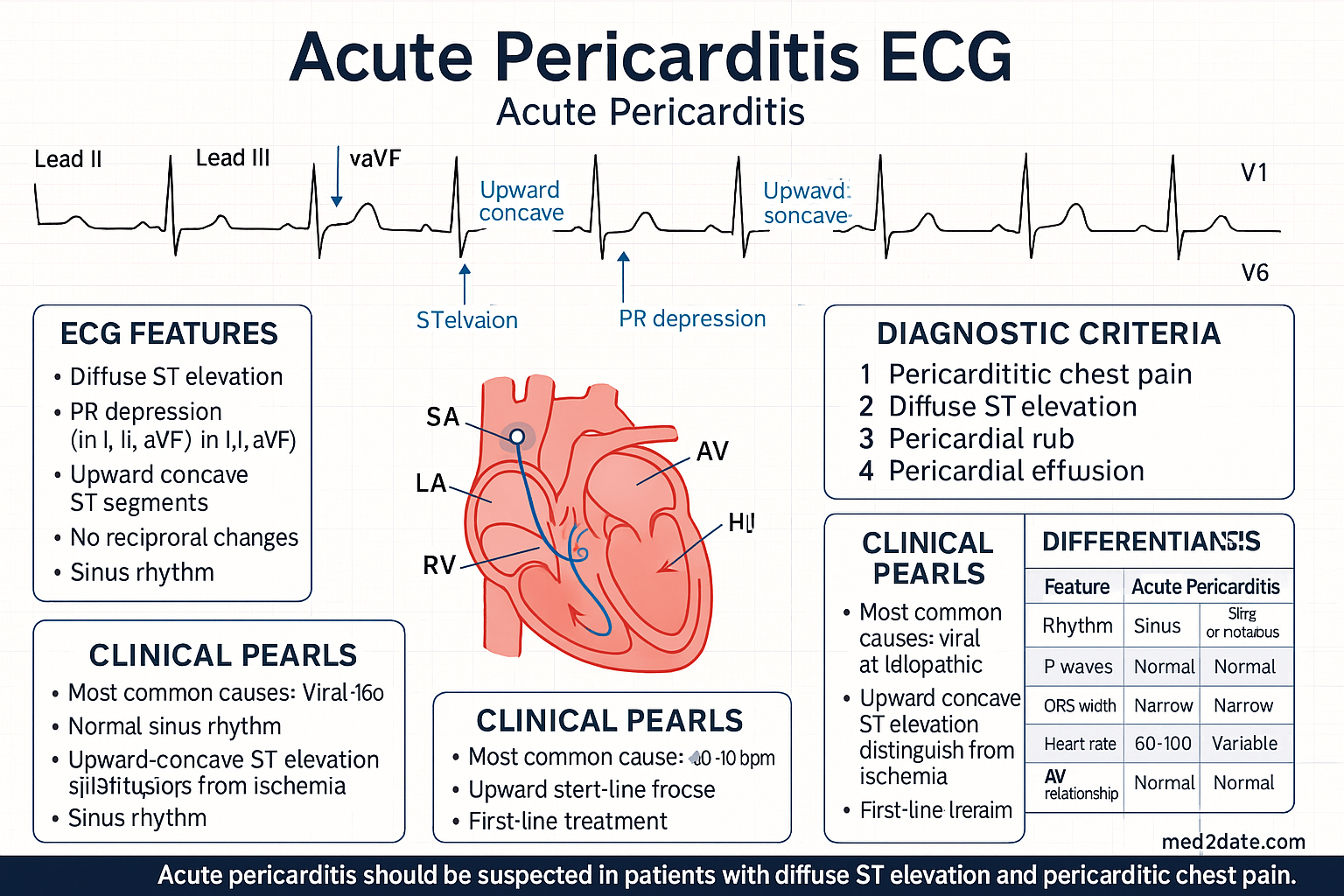
- Acute pericarditis is the most common pericardial disease, presenting with pleuritic chest pain that improves on leaning forward, a pericardial friction rub, diffuse ST elevation with PR depression on ECG, and new or worsening pericardial effusion.
- Most cases (80–90%) in Australia are idiopathic or presumed viral; always consider TB in immunocompromised and ATSI populations, and uraemic pericarditis in advanced CKD.
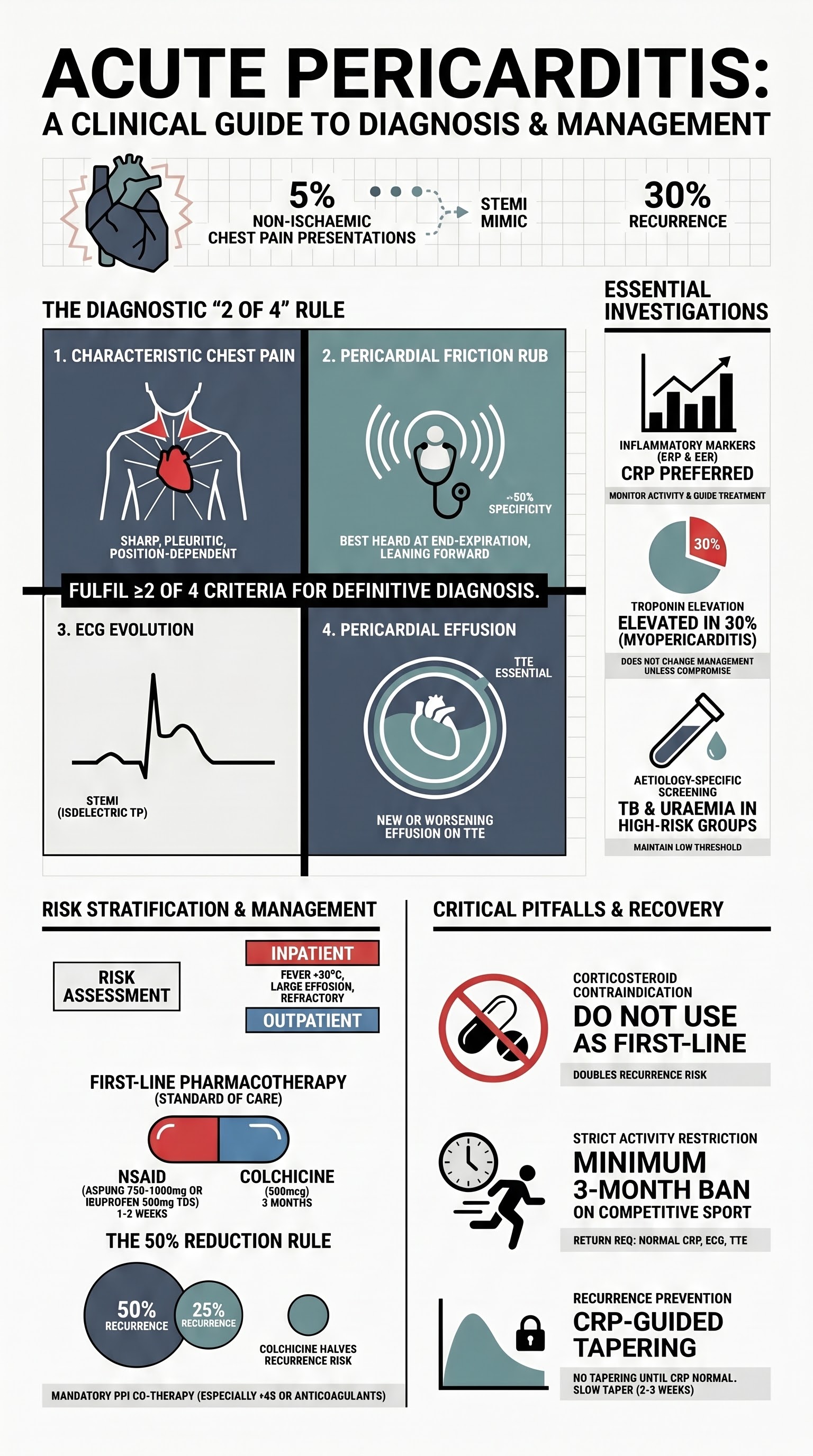
- The diagnosis is clinical — fulfil ≥2 of 4 criteria: characteristic chest pain, pericardial friction rub, ECG changes, or new/worsening pericardial effusion on echocardiography.
- CRP and ESR are essential for confirming inflammation and guiding treatment duration; troponin elevation (myopericarditis) occurs in up to 30% of cases and does not change management in the absence of haemodynamic compromise.
- First-line therapy is aspirin (750–1000 mg PO TDS for 1–2 weeks) or ibuprofen (600 mg PO TDS for 1–2 weeks) PLUS colchicine (500 mcg PO BD for 3 months) — this combination reduces recurrence by approximately 50%.
- Colchicine must be dosed by weight (500 mcg OD if <70 kg) and requires renal dose adjustment; avoid in severe hepatic impairment and pregnancy.
- Corticosteroids are NOT first-line and should be reserved for refractory cases, specific autoimmune aetiologies, or contraindications to NSAIDs; early corticosteroid use increases recurrence risk.
- Cardiac MRI (CMR) with late gadolinium enhancement is recommended when the diagnosis is uncertain, to assess for myocardial involvement, or to guide safe return to activity.
- Recurrent pericarditis occurs in approximately 30% of cases; risk factors include early corticosteroid use, inadequate initial colchicine, and elevated CRP at presentation.
- For refractory recurrent pericarditis, anti-IL-1 agents (anakinra, rilonacept) are effective second-line therapies; intrapericardial corticosteroids and pericardiectomy are reserved for the most resistant cases.
- Patients should be restricted from competitive sport for at least 3 months; return requires normalisation of CRP, no effusion, and normal ECG and CMR findings.
- Uraemic pericarditis requires intensification of dialysis (ideally daily), not anti-inflammatory therapy as first-line; TB pericarditis mandates standard anti-TB therapy with consideration of corticosteroids.
- Aboriginal and Torres Strait Islander Australians have higher rates of TB and rheumatic heart disease, requiring a lower threshold for screening in suspected pericarditis of uncertain aetiology.
Introduction & Australian Epidemiology
Acute pericarditis is inflammation of the pericardial sac, the fibrous double-layered membrane enclosing the heart. It is the most common disease of the pericardium and accounts for approximately 5% of emergency department presentations with non-ischaemic chest pain in Australia. The condition is typically self-limiting but carries risks of recurrence, cardiac tamponade, and constrictive pericarditis if inadequately treated.
In Australia, the annual incidence of acute pericarditis is estimated at 27.7 per 100,000 population, with a peak incidence in males aged 20–50 years. Viral aetiologies predominate, particularly in temperate zones where coxsackievirus B and echovirus circulate seasonally. The post-cardiac injury syndrome (Dressler syndrome) following myocardial infarction or cardiac surgery accounts for a smaller but clinically significant proportion of cases.
Importantly, Australia's burden of rheumatic heart disease and tuberculosis among Aboriginal and Torres Strait Islander communities means that pericardial disease of these aetiologies must be actively considered in relevant populations. TB pericarditis remains a significant differential in immunocompromised patients, including those with HIV, and in migrants from high-prevalence regions.
Clinical Presentation
Chest Pain Characteristics
The hallmark of acute pericarditis is sharp, pleuritic chest pain that is typically retrosternal or left-sided. The pain classically:
- Radiates to the trapezius ridge (pathognomonic) or left shoulder
- Improves when the patient sits up and leans forward
- Worsens with inspiration, coughing, and supine positioning
- May be accompanied by dyspnoea, particularly when a moderate-to-large effusion is present
- Differentiated from ischaemic pain by its pleuritic nature, positional relief, and absence of exertional trigger
ECG Changes
The ECG evolves through four stages in classic pericarditis:
| Stage | Timing | ECG Features |
|---|---|---|
| Stage 1 | Days 1–2 | Diffuse concave ST elevation (except aVR and V1); PR depression (most specific finding); no reciprocal ST depression (except aVR and V1) |
| Stage 2 | Days 2–3 | Normalisation of ST segments; T wave flattening |
| Stage 3 | Weeks | Diffuse T wave inversions |
| Stage 4 | Weeks to months | Normalisation of ECG |
Pericardial Friction Rub
A pericardial friction rub is the most specific physical finding (specificity ~90%) but sensitivity is only about 35–60%. It is best heard with the diaphragm of the stethoscope with the patient sitting upright and leaning forward, at end-expiration. The rub may be transient, so serial examinations may be required. A three-component rub (atrial systole, ventricular systole, rapid ventricular filling) is classic but a two-component or even monophonic rub may be heard.
Additional Clinical Features
- Low-grade fever (<38°C) is common; high fever (>39°C) should raise suspicion for purulent or tuberculous pericarditis
- Tachycardia may be present as a pain response or compensatory in the setting of significant effusion
- Pulsus paradoxus >10 mmHg suggests haemodynamically significant pericardial effusion or tamponade
- Beck's triad (hypotension, muffled heart sounds, jugular venous distension) indicates cardiac tamponade — a medical emergency
Aetiology
The majority of acute pericarditis cases in Australia are idiopathic (presumed viral). A systematic evaluation is warranted when clinical features suggest a specific underlying cause.
| Category | Aetiology | Key Distinguishing Features |
|---|---|---|
| Idiopathic / Viral | Coxsackievirus B, echovirus, adenovirus, CMV, EBV, parvovirus B19, SARS-CoV-2 | 80–90% of cases; often preceded by URTI; usually self-limiting; diagnosis of exclusion |
| Post-cardiac injury | Post-MI (Dressler syndrome), post-cardiac surgery, post-catheter ablation, post-trauma | Occurs days to weeks after injury; autoimmune mechanism; positive anti-heart antibodies |
| Autoimmune / Inflammatory | SLE, rheumatoid arthritis, systemic sclerosis, sarcoidosis, vasculitis, familial Mediterranean fever | Recurrent episodes; elevated ANA/RF; may be first presentation of underlying connective tissue disease |
| Uraemic | End-stage kidney disease (eGFR <15), dialysis-dependent CKD | Fibrinous pericarditis; responds to intensification of dialysis; WBC within pericardial fluid elevated |
| Malignant | Lung cancer, breast cancer, lymphoma, melanoma, mesothelioma | Large haemorrhagic effusion; cytology positive; progressive; consider in patients with known malignancy and new effusion |
| Tuberculous | Mycobacterium tuberculosis | Insidious onset; high ADA in fluid; predominantly lymphocytic; high prevalence in ATSI communities and immunocompromised patients |
| Purulent / Bacterial | Staphylococcus aureus, Streptococcus pneumoniae, Gram-negatives | High fever, toxic appearance; requires urgent pericardiocentesis and IV antibiotics; mortality up to 40% if untreated |
| Drug-related | Immune checkpoint inhibitors (pembrolizumab, nivolumab), hydralazine, isoniazid, methyldopa, phenytoin | Temporal association with drug initiation; checkpoint inhibitor pericarditis has a high recurrence rate |
| Post-irradiation | Prior mediastinal radiotherapy (lymphoma, breast cancer) | May present years after treatment; risk of constrictive pericarditis |
| Traumatic | Blunt or penetrating chest trauma | Pericardial tear may occur; may present acutely or with delayed post-traumatic syndrome |
Aetiology-Specific Testing Strategy
Targeted investigations should be performed based on clinical suspicion:
- Autoimmune screen: ANA, anti-dsDNA, complement (C3/C4), RF, anti-CCP — when recurrent pericarditis or features of connective tissue disease
- TB testing: Interferon-gamma release assay (QuantiFERON-TB Gold), pericardial fluid ADA, fluid AFB stain and culture, PCR for M. tuberculosis — ATSI patients, immunocompromised, migrants from endemic regions
- Uraemic assessment: eGFR, urea, creatinine, phosphate — if eGFR <30 mL/min/1.73 m²
- Malignancy workup: CT chest/abdomen/pelvis, pericardial fluid cytology, tumour markers — when large or recurrent effusion or risk factors present
- Drug history: Review for immune checkpoint inhibitors, hydralazine, isoniazid
Diagnostic Workup
Clinical Diagnostic Criteria
Acute pericarditis is diagnosed when at least 2 of 4 criteria are met:
- Characteristic chest pain (sharp, pleuritic, improved by sitting forward)
- Pericardial friction rub
- ECG changes (new widespread ST elevation or PR depression)
- New or worsening pericardial effusion on imaging
Supportive findings include elevated inflammatory markers (CRP, ESR), elevated troponin (suggesting myopericarditis), and fever.
Investigations
High-Sensitivity Troponin — Prognostic Implications
Elevated troponin defines myopericarditis (pericarditis with myocardial involvement). In the absence of haemodynamic compromise, heart failure, or sustained arrhythmia, isolated troponin elevation does not change management. Patients with myopericarditis should have prolonged activity restriction (at least 6 months) and be followed with repeat CMR before clearance.
Treatment
Risk Stratification — Inpatient vs Outpatient Management
First-Line Pharmacotherapy
The cornerstone of treatment is a combination of an anti-inflammatory agent plus colchicine. Aspirin or ibuprofen is preferred over other NSAIDs due to the best available evidence.
Gastroprotection
All patients receiving high-dose NSAIDs should receive concurrent gastroprotection with a proton pump inhibitor (PPI), e.g., pantoprazole 40 mg PO daily, particularly if aged >65 years, history of peptic ulcer disease, or on concomitant anticoagulation or corticosteroids.
Corticosteroids — When Indicated
Treatment Summary — Quick Reference
Activity Restriction
All patients with acute pericarditis should abstain from competitive and strenuous physical activity. The 2015 European Society of Cardiology guidelines recommend a minimum of 3 months restriction from competitive sport following an acute episode. In myopericarditis, restriction extends to 6 months. Return to competitive activity requires:
- Normalisation of CRP and ESR
- Resolution of pericardial effusion on echocardiography
- Normal 12-lead ECG and Holter monitoring
- CMR demonstrating no residual oedema or LGE (especially in myopericarditis)
- Normal LV systolic function
Recurrent Pericarditis
Definition & Incidence
Recurrent pericarditis is defined as a symptomatic recurrence of pericarditis after a documented first episode with a symptom-free interval of at least 4–6 weeks. It occurs in approximately 30% of patients after an initial episode, with the highest risk in the first 18 months.
Risk Factors for Recurrence
- Inadequate initial treatment (NSAID dose too low, insufficient duration, no colchicine)
- Early use of corticosteroids in the first episode (approximately doubles recurrence risk)
- Incompletely treated or missed underlying aetiology (autoimmune, TB, malignancy)
- Large pericardial effusion at presentation
- Elevated CRP at diagnosis that was not monitored to confirm normalisation
- Younger age and female sex
- Immune checkpoint inhibitor-related pericarditis
Prevention Strategies
- Colchicine 500 mcg BD (or OD if <70 kg) for 3 months at first episode — the single most important intervention to prevent recurrence
- Adequate NSAID dose and duration; do not stop NSAIDs prematurely
- Monitor CRP and do not taper anti-inflammatories until CRP is normal
- Avoid corticosteroids at first episode unless specifically indicated
- If corticosteroids are required, use the lowest effective dose (0.25 mg/kg/day) and taper very slowly guided by CRP
Management of Recurrent Pericarditis — Step-Up Approach
Anti-IL-1 Agents — Detail
Corticosteroid Tapering Protocol (Recurrent Pericarditis)
When corticosteroids are required in recurrent pericarditis, a slow taper is critical to prevent rebound flares:
- Start prednisolone 0.25–0.5 mg/kg/day (max ~25 mg/day)
- Maintain initial dose for 2–4 weeks until CRP normalises
- Reduce by 2.5 mg every 2–4 weeks
- Below 10 mg/day: reduce by 1.25 mg every 2–4 weeks
- If CRP rises during taper: pause taper, increase dose to last effective dose, and consider adding anti-IL-1 agent
- Complete taper over 3–6 months minimum; concurrent colchicine mandatory throughout
Special Populations
Pregnancy
Paediatrics
Elderly (>65 years)
Renal Impairment
Hepatic Impairment
Immunocompromised
Aboriginal and Torres Strait Islander Health Considerations
📚 References
- 1. Adler Y, Charron P, Imazio M, et al. 2015 ESC Guidelines for the diagnosis and management of pericardial diseases. Eur Heart J. 2015;36(42):2921–2964. doi:10.1093/eurheartj/ehv318
- 2. Imazio M, Brucato A, Cemin R, et al. A randomized trial of colchicine for acute pericarditis (COPE). N Engl J Med. 2013;369(16):1522–1528. doi:10.1056/NEJMoa1208536
- 3. Imazio M, Brucato A, Cemin R, et al. Colchicine for recurrent pericarditis (CORP): a randomized trial. Ann Intern Med. 2011;155(7):409–414. doi:10.7326/0003-4819-155-7-201110040-00359
- 4. Imazio M, Andreis A, De Ferrari GM, et al. Anakinra for corticosteroid-dependent and colchicine-resistant first episode of recurrent pericarditis (AIRTRIP): a randomised, double-blind, placebo-controlled trial. Lancet. 2016;387(10013):330–331. doi:10.1016/S0140-6736(15)00963-4
- 5. Klein AL, Imazio M, Cremer P, et al. Phase 3 trial of interleukin-1 trap rilonacept in recurrent pericarditis (RHAPSODY). N Engl J Med. 2021;384(1):31–41. doi:10.1056/NEJMoa2027892
- 6. Chiabrando JG, Bonaventura A, Vecchié A, et al. Management of acute and recurrent pericarditis: JACC state-of-the-art review. J Am Coll Cardiol. 2020;75(1):76–92. doi:10.1016/j.jacc.2019.11.021
- 7. Lotrionte M, Biondi-Zoccai G, Imazio M, et al. International collaborative systematic review of controlled clinical trials on pharmacologic treatments for acute pericarditis and its recurrences. Am Heart J. 2010;160(4):662–670. doi:10.1016/j.ahj.2010.06.026
- 8. Australian Institute of Health and Welfare (AIHW). Rheumatic heart disease and acute rheumatic fever in Australia: 2013–2017. Cat. no. CVD 87. Canberra: AIHW; 2019.
- 9. RHDAustralia (ARF/RHD writing group). National guideline for the prevention, diagnosis and management of acute rheumatic fever and rheumatic heart disease. 3rd ed. Darwin: Menzies School of Health Research; 2020.
- 10. Adler Y, Charron P, Imazio M, et al. 2015 ESC Guidelines for the diagnosis and management of pericardial diseases. Eur Heart J. 2015;36(42):2921–2964. [Supplementary: return-to-play recommendations, Section 7.5]
- 11. Basso C, Aguilera B, Banner J, et al. Guidelines for autopsy investigation of sudden cardiac death: 2017 update from the Association for European Cardiovascular Pathology. Virchows Arch. 2017;471(6):691–705. doi:10.1007/s00428-017-2227-z
- 12. World Health Organization (WHO). Global tuberculosis report 2023. Geneva: WHO; 2023.
- 13. Klein AL, Abbara S, Agler DA, et al. American Society of Echocardiography clinical recommendations for multimodality cardiovascular imaging of patients with pericardial disease. J Am Soc Echocardiogr. 2013;26(9):965–1012. doi:10.1016/j.echo.2013.06.023
- 14. Maron BJ, Zipes DP, Kovacs RJ. Eligibility and disqualification recommendations for competitive athletes with cardiovascular abnormalities: preamble, principles, and general considerations. Circulation. 2015;132(22):e256–e261. doi:10.1161/CIR.0000000000000291
- 15. Imazio M, Brucato A, Barbieri A, et al. Good prognosis for pericarditis with and without myocardial involvement: results from a multicenter, prospective cohort study. Circulation. 2013;128(1):42–49. doi:10.1161/CIRCULATIONAHA.113.001531