📋 Key Information Summary
- Acute Coronary Syndromes (ACS) encompass a spectrum from unstable angina (UA) to NSTEMI and STEMI, all requiring urgent evaluation and management.
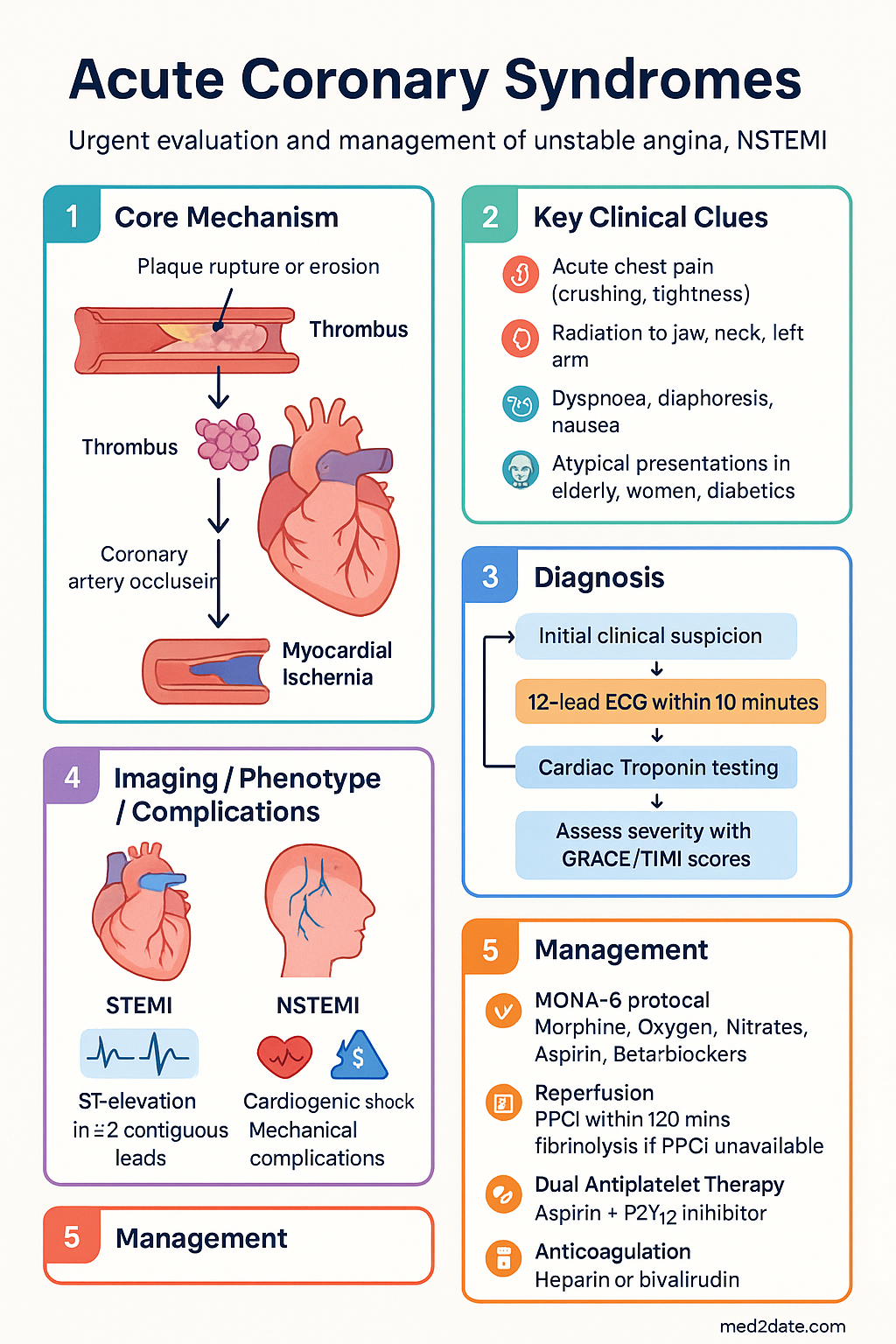
- Immediate management begins with the MONA-B protocol: Morphine (if required), Oxygen (only if SpO2 < 94%), Nitrates, Aspirin (300 mg stat), and Beta-blockers (if appropriate).
- For STEMI, the cornerstone of treatment is timely reperfusion: Primary Percutaneous Coronary Intervention (PPCI) within 120 minutes of first medical contact is preferred; fibrinolysis within 30 minutes if PPCI is not available.
- NSTEMI/UA requires rapid risk stratification using validated scores (GRACE or TIMI) to guide the decision for an early invasive (angiography) versus conservative strategy.
- Dual Antiplatelet Therapy (DAPT) with aspirin and a P2Y12 inhibitor is fundamental for all ACS types; choice and duration depend on bleeding risk (PRECISE-DAPT score) and ischemic risk.
- Anticoagulation with heparin (UFH or enoxaparin) or bivalirudin is required in the acute phase, with choice influenced by renal function and planned reperfusion strategy.
- Mechanical complications (VSD, free wall rupture, papillary muscle rupture) are rare but life-threatening emergencies requiring immediate surgical consultation.
- Cardiogenic shock complicating ACS necessitates urgent revascularization, haemodynamic support (e.g., vasopressors, inotropes, mechanical circulatory support), and intensive care management.
- Comprehensive post-ACS care includes cardiac rehabilitation, lifelong secondary prevention (statins, ACEi/ARB, beta-blockers), and addressing lifestyle risk factors (smoking cessation, diet, exercise).
- Aboriginal and Torres Strait Islander peoples experience higher rates of ACS, delayed presentations, and poorer outcomes, requiring culturally safe, coordinated care.
Introduction & Australian Epidemiology
Acute Coronary Syndromes (ACS) represent a continuum of ischaemic heart disease ranging from unstable angina (UA) to non-ST elevation myocardial infarction (NSTEMI) and ST-elevation myocardial infarction (STEMI). They are a leading cause of morbidity and mortality in Australia. In 2022, ischaemic heart disease remained the leading cause of death, accounting for approximately 10% of all deaths.
Australia has established world-leading systems of care for ACS, particularly for STEMI, with coordinated networks for primary percutaneous coronary intervention (PPCI). Despite this, significant disparities exist. Aboriginal and Torres Strait Islander peoples experience an age-standardised rate of acute myocardial infarction approximately twice that of non-Indigenous Australians, with higher rates of comorbidities and barriers to accessing timely care.
Clinical Presentation & Diagnostic Criteria
ACS typically presents with acute chest pain, discomfort, or pressure, often described as crushing, tightness, or heaviness. Pain may radiate to the jaw, neck, left arm, or epigastrium. Associated symptoms include dyspnoea, diaphoresis, nausea, and lightheadedness. Atypical presentations (e.g., isolated dyspnoea, fatigue) are more common in the elderly, women, and patients with diabetes.
Diagnostic Workup
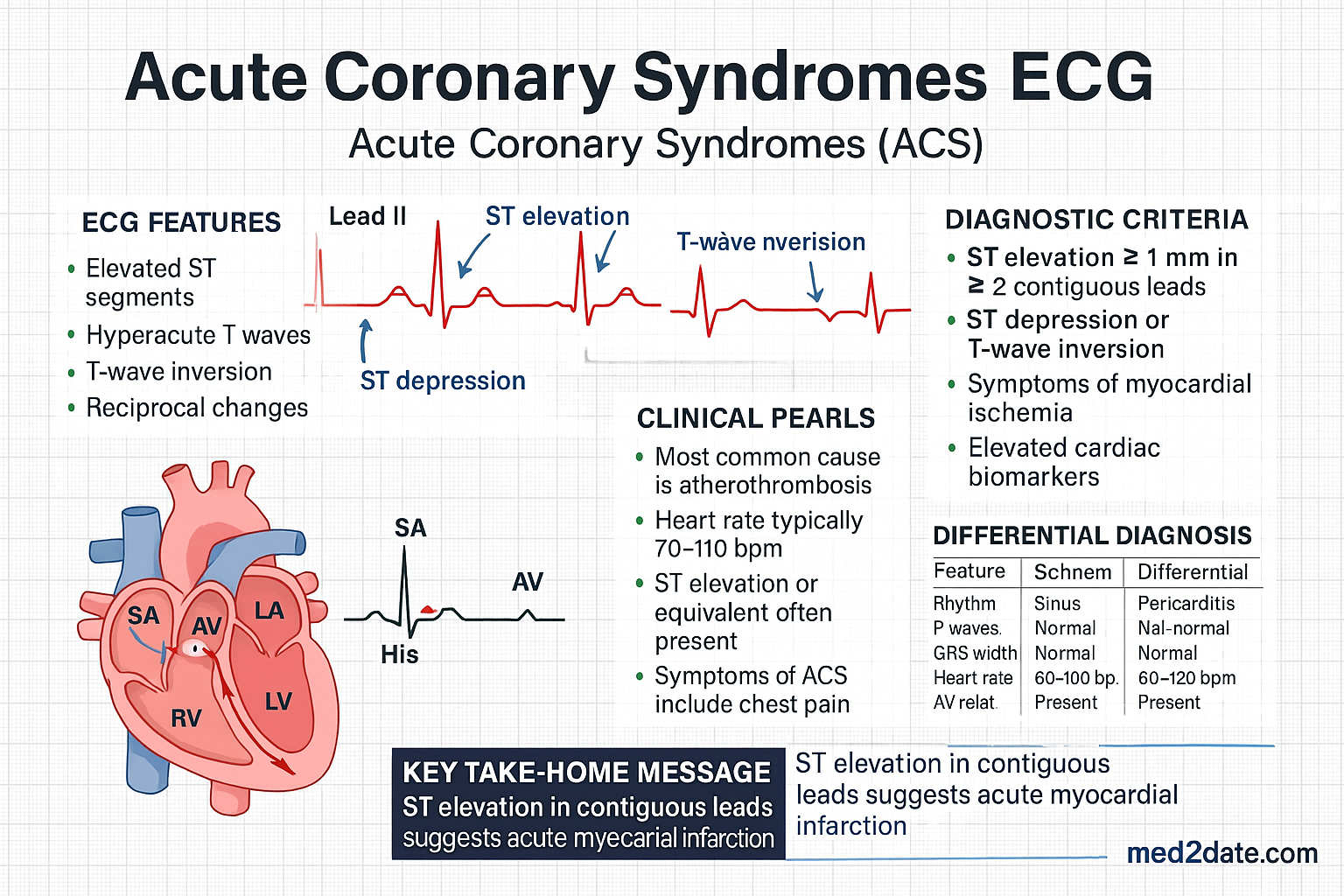
- 12-lead ECG: Must be performed within 10 minutes of arrival. ST-elevation in ≥2 contiguous leads indicates STEMI. ST-depression, T-wave inversion, or transient ST-elevation suggest NSTEACS.
- Cardiac Troponin: High-sensitivity troponin (hs-cTn) is the preferred biomarker. A rise and/or fall pattern with at least one value above the 99th percentile upper reference limit confirms myocardial injury. Serial testing at 0 and 1-3 hours is standard.
- Other investigations: Chest X-ray, full blood count, electrolytes, creatinine, coagulation screen, and lipids.
STEMI Management
Initial Assessment & Time-Critical Goals
The goal is to restore coronary blood flow as quickly as possible. Time is myocardium.
Reperfusion Strategies
Complications of STEMI
Early recognition of complications is vital. These include arrhythmias (VT/VF, heart block), acute heart failure, cardiogenic shock, mechanical complications (see below), and pericarditis.
NSTEMI/Unstable Angina
Risk Stratification
Use validated scores to guide the timing of invasive management.
Initial Anti-Ischaemic Therapy
- Nitrates: Sublingual GTN 0.4 mg every 5 minutes for up to 3 doses. IV GTN infusion if ongoing pain.
- Beta-blockers: e.g., Metoprolol 25-50 mg PO BD-TDS. Avoid in acute heart failure or cardiogenic shock.
- Morphine: 2.5-5 mg IV for pain not relieved by nitrates. Use with caution (hypotension risk).
Antiplatelet & Anticoagulation Therapy
Dual Antiplatelet Therapy (DAPT)
Aspirin 300 mg stat (enteric-coated if tolerated) followed by 100 mg daily indefinitely. A P2Y12 inhibitor is added.
Anticoagulation
Anticoagulation is continued during the acute phase (usually 48 hours or until PCI).

Post-ACS Care & Secondary Prevention
Cardiac Rehabilitation
All patients should be referred to an accredited cardiac rehabilitation programme. This is associated with reduced mortality and improved quality of life.
Long-Term Medications
- High-Intensity Statin: Atorvastatin 80 mg or Rosuvastatin 20-40 mg nightly. Target LDL-C <1.8 mmol/L or ≥50% reduction.
- ACE Inhibitor/ARB: e.g., Ramipril 2.5-10 mg daily, titrated to max tolerated dose. Especially for patients with LVEF ≤40%, hypertension, diabetes, or CKD.
- Beta-Blocker: e.g., Bisoprolol, Carvedilol, Metoprolol succinate. Continue indefinitely, particularly for those with LVEF ≤40% or heart failure.
Lifestyle Modifications
Cessation support (pharmacotherapy and counselling), Mediterranean-style diet, regular aerobic exercise (150 mins/week), weight management, and psychosocial support.
Follow-up Protocols
GP review within 1-2 weeks post-discharge. Cardiology review at 6-12 weeks. Repeat lipid profile and HbA1c at 6-8 weeks. Consider stress testing if symptoms recur.
Mechanical Complications
Cardiogenic Shock Management
The foundation is urgent revascularisation. Haemodynamic support is critical.
- Vasopressors/Inotropes: Noradrenaline (first-line for shock), dobutamine, or milrinone to maintain perfusion.
- Mechanical Circulatory Support (MCS): Intra-aortic balloon pump (IABP), Impella, or VA-ECMO may be considered in refractory shock. Requires discussion with a tertiary centre with MCS capability.
Special Populations
ACS in pregnancy is rare but serious. Diagnosis is challenging (troponin normal in pregnancy).
Management: Requires multidisciplinary team (cardiology, obstetrics, anaesthetics). Aspirin is safe. Avoid statins, ACEi/ARB. PCI with minimal radiation is preferred over fibrinolysis.
ACS in children is usually associated with congenital heart disease, Kawasaki disease, or anomalous coronary arteries.
Management: Adult protocols are generally followed, with weight-based dosing. Consultation with a paediatric cardiologist is essential.
High bleeding and thrombotic risk. Dose-adjust anticoagulants (enoxaparin, eptifibatide). Ticagrelor preferred over clopidogrel. Avoid fondaparinux if CrCl <30.
📚 References
- 1. Chew DP, Scott IA, Cullen L, et al. National Heart Foundation of Australia & Cardiac Society of Australia and New Zealand: Australian Clinical Guidelines for the Management of Acute Coronary Syndromes 2016. Heart, Lung and Circulation. 2016;25(9):895-951.
- 2. Ibanez B, James S, Agewall S, et al. 2017 ESC Guidelines for the management of acute myocardial infarction in patients presenting with ST-segment elevation. European Heart Journal. 2018;39(2):119-177.
- 3. Collet JP, Thiele H, Barbato E, et al. 2020 ESC Guidelines for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation. European Heart Journal. 2021;42(14):1289-1367.
- 4. Australian Institute of Health and Welfare (AIHW). Acute coronary syndrome and coronary heart disease in Australia 2024. Cat. no. CVD 94. Canberra: AIHW; 2024.
- 5. National Health and Medical Research Council (NHMRC). Australian guidelines for the prevention and control of infection in healthcare. Canberra: NHMRC; 2019.
- 6. National Heart Foundation of Australia. Secondary prevention of cardiovascular disease. Quick reference guide. 2020.
- 7. RACGP. Guidelines for preventive activities in general practice (Red Book). 9th edn. East Melbourne: RACGP; 2016.
- 8. O'Gara PT, Kushner FG, Ascheim DD, et al. 2013 ACCF/AHA guideline for the management of ST-elevation myocardial infarction. Journal of the American College of Cardiology. 2013;61(4):e78-e140.
- 9. Amsterdam EA, Wenger NK, Brindis RG, et al. 2014 AHA/ACC guideline for the management of patients with non–ST-elevation acute coronary syndromes. Journal of the American College of Cardiology. 2014;64(24):e139-e228.
- 10. RHDAustralia (RHD Australia), Australian Government Department of Health and Ageing. The Australian guideline for prevention, diagnosis and management of acute rheumatic fever and rheumatic heart disease (3rd edition). 2020.