📋 Key Information Summary
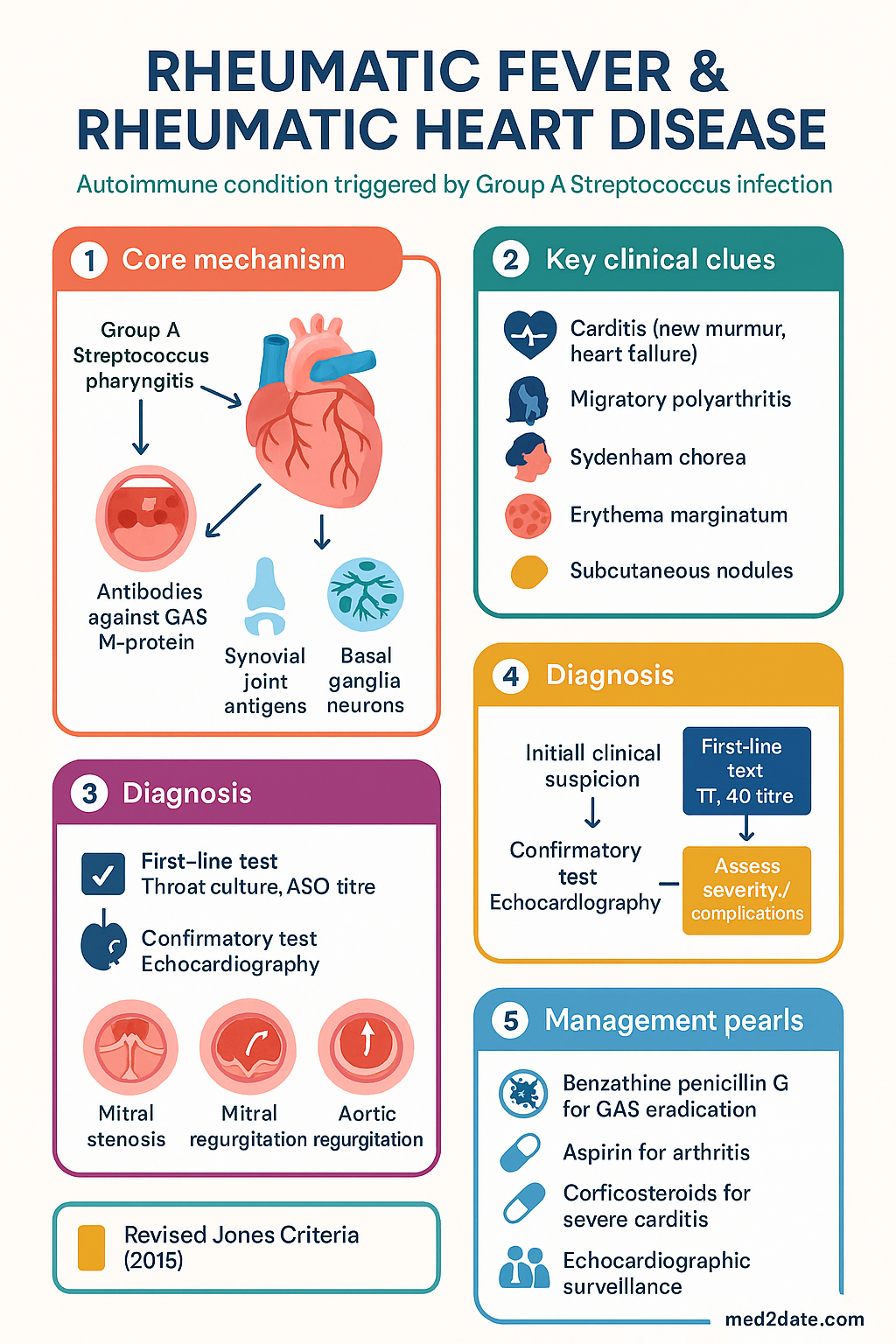
- Acute rheumatic fever (ARF) is an autoimmune inflammatory condition triggered by Group A Streptococcus (GAS) pharyngitis, primarily affecting children aged 5–14 years.
- Recurrent episodes of ARF cause cumulative cardiac valve damage, leading to rheumatic heart disease (RHD) — a chronic and often disabling condition.
- Diagnosis is clinical, based on the revised Jones Criteria (2015): two major manifestations OR one major + two minor, plus evidence of preceding GAS infection.
- Major Jones manifestations: carditis (including valvulitis), polyarthritis, Sydenham chorea, erythema marginatum, subcutaneous nodules.
- Minor Jones manifestations: fever, elevated acute-phase reactants (ESR/CRP), prolonged PR interval on ECG, arthralgia (only if arthritis is not a major manifestation).
- Evidence of preceding GAS infection: positive throat culture, elevated/strengthening ASO titre or anti-DNase B, or positive rapid antigen detection test.
- Acute treatment: benzathine penicillin G 1.2 MU IM (single dose) to eradicate GAS, plus anti-inflammatory therapy (aspirin for arthritis, corticosteroids for severe carditis).
- Secondary prophylaxis: benzathine penicillin G 1.2 MU IM every 21 days (every 14 days in high-risk patients) — duration depends on age and presence of RHD.
- RHD management requires multidisciplinary care, echocardiographic surveillance, anticoagulation for atrial fibrillation or prosthetic valves, and timely surgical valve repair or replacement.
- Aboriginal and Torres Strait Islander peoples bear the greatest burden of ARF and RHD in Australia, with incidence rates among the highest globally — RHDAustralia clinical guidelines (2020) are the standard of care.
- The Australian RHD Register and Control Programme support notification, recall, and secondary prophylaxis adherence in endemic regions (NT, QLD, WA).
- Penicillin allergy: use azithromycin 500 mg PO day 1 then 250 mg daily for 4 days (secondary prophylaxis: erythromycin 250 mg BD or azithromycin if tolerated).
- ARF is a notifiable disease in the NT, QLD, SA, and WA.
Introduction & Australian Epidemiology
Acute rheumatic fever (ARF) is a systemic autoimmune condition triggered by pharyngeal infection with Group A Streptococcus (GAS; Streptococcus pyogenes). An abnormal immune response leads to inflammation of the heart, joints, brain, and skin. Recurrent episodes cause cumulative valvular damage, culminating in rheumatic heart disease (RHD) — a chronic, progressive condition responsible for significant morbidity and premature mortality.
In Australia, ARF and RHD are diseases of inequity. The burden falls overwhelmingly on Aboriginal and Torres Strait Islander peoples, particularly children and young adults living in remote and very remote communities across the Northern Territory, Queensland, and Western Australia. Incidence rates of ARF among Indigenous Australians in high-risk areas can exceed 150–200 per 100,000 children aged 5–14 years, comparable to the highest rates globally. In contrast, ARF in non-Indigenous Australians in metropolitan areas is exceedingly rare, though clusters of ARF have been reported in non-Indigenous children in New Zealand and parts of the United States.
ARF is a notifiable disease in the Northern Territory, Queensland, South Australia, and Western Australia. National notification data consistently show that over 95% of ARF cases occur in Aboriginal and Torres Strait Islander peoples. The National Aboriginal Community Controlled Health Organisation (NACCHO) and RHDAustralia coordinate registries, clinical guidelines, and control programmes across endemic jurisdictions.
The revised Australian guidelines for the management of ARF and RHD were published by RHDAustralia (formerly the RHD Control Programme) in 2020, aligned with the New Zealand guidelines and the 2015 AHA revised Jones Criteria. These guidelines form the basis of this article's recommendations.
Pathophysiology & Group A Streptococcus
Molecular Mimicry
The pathogenesis of ARF is based on molecular mimicry between GAS antigens and host tissues. Antibodies produced against GAS M-protein and hyaluronate capsule cross-react with:
- Cardiac myosin and valve glycoproteins — leading to valvulitis and carditis.
- Synovial joint antigens — causing migratory polyarthritis.
- Basal ganglia neurones — producing Sydenham chorea.
- Dermal collagen — associated with subcutaneous nodules.
Susceptible Host
Not all individuals who contract GAS pharyngitis develop ARF. Host susceptibility is influenced by:
- Genetic factors — certain HLA class II alleles (DR7, DR5, DQ2) confer increased risk.
- Streptococcal strain — rheumatogenic strains (M-types 1, 3, 5, 6, 14, 18, 19, 24, 27, 29) are associated with pharyngitis and ARF; pyoderma strains (49, 53, 55, 56, 57, 59) are associated with impetigo and, in some populations, post-cutaneous ARF.
- Repeated exposure in crowded living conditions increases risk.
- Age — peak incidence in children 5–14 years; rare before age 3 and after age 40.
The Latent Period
ARF typically manifests 2–4 weeks after GAS pharyngitis. The onset may be insidious. Many patients do not recall a preceding sore throat, especially in populations where subclinical GAS infection is common.
Cardiac Pathology in RHD
Repeated episodes of ARF cause progressive valvular inflammation and scarring. The mitral valve is affected in ~90% of cases, followed by the aortic valve. Pathological features include:
- Acute: fibrinoid necrosis of valve leaflets, Aschoff bodies (granulomas) in myocardium.
- Chronic: commissural fusion, chordal shortening and thickening, calcification — leading to mitral stenosis, regurgitation, or mixed disease.
- Aortic regurgitation occurs in ~30% of RHD cases, often combined with mitral disease.
Clinical Presentation & Jones Criteria (Major & Minor)
The diagnosis of ARF is clinical. The 2015 revised Jones Criteria, endorsed by the American Heart Association (AHA) and adopted by RHDAustralia, require evidence of preceding GAS infection plus:
- Two major manifestations, OR
- One major + two minor manifestations.
Exceptions: Three categories of clinical presentation are considered diagnostic of ARF even without strict adherence to the above combination:
- Sydenham chorea (may be the sole manifestation).
- Insidious-onset carditis (may present as heart failure without other criteria).
- Recurrent ARF — a known history of RHD or prior ARF, with one major or several minor manifestations plus evidence of recent GAS infection.
Major Manifestations
| Manifestation | Features | Frequency |
|---|---|---|
| Carditis (including valvulitis) | New murmur of mitral regurgitis (apical pansystolic) or aortic regurgitation (early diastolic). Pericarditis, cardiomegaly, heart failure. Echocardiographic evidence of subclinical valvulitis is now accepted as a major manifestation. | 50–70% |
| Polyarthritis | Migratory, affecting large joints (knees, ankles, elbows, wrists). Flitting — one joint improves as another becomes involved. Extremely painful and responsive to salicylates. | 60–75% |
| Sydenham chorea | Involuntary, purposeless movements; emotional lability; hypotonia; "milkmaid grip"; "darting tongue". May occur in isolation and late (weeks to months after GAS infection). Also called St Vitus dance. | 10–30% |
| Erythema marginatum | Evanescent, non-pruritic, erythematous rash with serpiginous margins and central clearing. Trunk and proximal limbs. Not scaly. Worsened by warmth. | class="guideline-td">5–10%|
| Subcutaneous nodules | Small (0.5–2 cm), firm, painless, mobile nodules over extensor surfaces of joints (elbows, knees, wrists, occiput, spine). Usually associated with severe carditis. | 2–10% |
Minor Manifestations
| Manifestation | Notes |
|---|---|
| Fever | ≥38°C. Non-specific. Common at presentation. |
| Polyarthralgia | Can only be counted as minor if arthritis is NOT a major manifestation. Otherwise excluded to avoid "double counting." |
| Elevated ESR ≥60 mm/hr or CRP ≥30 mg/L | Acute-phase reactants. ESR may be unreliable if there is concurrent heart failure (hepatic congestion lowers ESR). |
| Prolonged PR interval on ECG | Age-adjusted. First-degree AV block. Does NOT imply progression to complete heart block. |
Evidence of Preceding GAS Infection
At least one of the following must be present (except in Sydenham chorea and insidious-onset carditis):
- Positive throat swab culture for GAS.
- Positive rapid antigen detection test (RADT) for GAS.
- Elevated or rising anti-streptolysin O (ASO) titre.
- Elevated anti-DNase B titre (particularly useful when pharyngeal infection is absent and post-cutaneous GAS is suspected).
- Streptozyme test (where available).
Investigations
Laboratory Investigations
Cardiac Imaging
Treatment of Acute Rheumatic Fever
Step 1 — Eradicate GAS
All patients with ARF — regardless of throat swab result — should receive antibiotic therapy to eradicate residual GAS from the pharynx.
Step 2 — Anti-inflammatory Therapy
Anti-inflammatory treatment reduces fever, pain, and joint inflammation, but does NOT alter the natural history of carditis.
Step 3 — Management of Heart Failure in Acute Carditis
If heart failure is present:
- Diuretics (frusemide 0.5–1 mg/kg IV/PO) for fluid overload.
- ACE inhibitors (ramipril or enalapril) if MR is significant — use cautiously, titrate slowly.
- Bed rest and fluid restriction.
- Avoid digoxin in acute carditis (higher risk of toxicity due to myocardial inflammation).
- Urgent cardiology referral for inpatient management.
Step 4 — Management of Sydenham Chorea
Sydenham chorea is usually self-limiting (resolving within 6 weeks to 6 months) but may persist. Management includes:
- Reassurance and supportive care. Reduce environmental stimuli.
- If functionally disabling: sodium valproate 15–20 mg/kg/day PO (first-line) or carbamazepine.
- Severe cases: short course of corticosteroids may be considered.
- Psychological support — anxiety and emotional lability are common.
- Initiate secondary prophylaxis regardless of GAS serology (chorea may occur without evidence of preceding infection).
Monitoring During Acute Episode
Secondary Prophylaxis
Secondary prophylaxis with regular benzathine penicillin G (BPG) injections is the cornerstone of preventing recurrent ARF and progressive RHD. Adherence to prophylaxis is the single most important modifiable factor in RHD outcomes.
Benzathine Penicillin G — Secondary Prophylaxis
Penicillin Allergy — Alternative Prophylaxis
Duration of Secondary Prophylaxis
| Clinical Scenario | Recommended Duration |
|---|---|
| ARF without carditis (no valve disease on echo) | Until age 21 years OR 5 years after last episode (whichever is longer) |
| ARF with mild carditis (no residual valve disease at follow-up echo) | Until age 25–30 years OR 10 years after last episode (whichever is longer) |
| ARF with persistent valve disease / established RHD | Lifelong or until specialist review (age ≥35–40, no recurrence ≥10 years, no valve disease on echo) |
| Recurrent ARF episodes | Prolonged / lifelong prophylaxis regardless of valve status |
Rheumatic Heart Disease (RHD) Management
RHD results from cumulative valve damage from one or more episodes of ARF. Management requires lifelong secondary prophylaxis plus medical and surgical management of valve disease.
Severity Classification (Echocardiographic)
Medical Management of RHD
- Heart failure: Diuretics (frusemide, spironolactone), ACE inhibitors (ramipril, perindopril), beta-blockers (carvedilol). Avoid beta-blockers in severe symptomatic MS.
- Atrial fibrillation: Anticoagulation with warfarin (target INR 2.0–3.0). DOACs are generally NOT recommended for RHD-related AF with moderate-to-severe mitral stenosis. Rate control with beta-blockers or diltiazem. Consider rhythm control if symptomatic.
- Anticoagulation for prosthetic valves: Warfarin is mandatory for mechanical prosthetic valves. Target INR varies by valve position and type (aortic: 2.0–3.0; mitral: 2.5–3.5). Low-dose aspirin (75–100 mg) may be added.
- Endocarditis prophylaxis: Prophylactic antibiotics are recommended for dental and high-risk procedures in patients with prosthetic valves or prior endocarditis, according to current Australian guidelines.
Surgical and Interventional Management
Surgical referral should be considered when there is:
- Symptomatic severe valve disease despite optimal medical therapy.
- Asymptomatic severe valve disease with evidence of LV dysfunction, pulmonary hypertension, or progressive chamber dilatation.
- Severe mitral stenosis (MVA ≤1.0 cm²) — consider percutaneous balloon mitral valvuloplasty (PBMV) if valve morphology is favourable.
| Intervention | Indication | Considerations |
|---|---|---|
| Mitral valve repair | Preferred for severe MR with suitable anatomy | Avoids lifelong anticoagulation. Better outcomes than replacement. Requires surgical expertise. |
| Mitral valve replacement | When repair is not feasible (heavily calcified, fused leaflets) | Mechanical valve: lifelong warfarin. Bioprosthetic: limited durability in young patients. |
| PBMV (balloon valvuloplasty) | Severe MS (MVA ≤1.5 cm²) with favourable morphology | Avoid if LA thrombus, significant MR, or heavily calcified/subvalvular disease. Available at major cardiac centres. |
| Aortic valve replacement | Severe AR or AS | TAVR is generally not used for rheumatic aortic disease. SAVR remains standard. |
Contraception and Pregnancy Planning
Women of childbearing age with RHD require:
- Contraception counselling — warfarin is teratogenic (first trimester exposure causes warfarin embryopathy).
- Pre-pregnancy planning with cardiology and obstetric teams at a tertiary centre.
- Warfarin should be switched to heparin (LMWH or UFH) before conception or by 6 weeks' gestation.
- Severe RHD may need surgical correction before pregnancy.
Special Populations
Aboriginal and Torres Strait Islander Health Considerations
ARF and RHD are among the starkest markers of health inequity in Australia. Over 95% of new ARF cases occur in Aboriginal and Torres Strait Islander peoples. Rates of RHD are 20–40 times higher than in non-Indigenous Australians. ARF is almost entirely preventable through improved housing, reduced overcrowding, and access to prompt antibiotic treatment for GAS pharyngitis.
The RHDAustralia Australian guideline for prevention, diagnosis and management of acute rheumatic fever and rheumatic heart disease (3rd edition, 2020) is the definitive clinical standard.
Quick Reference — Acute ARF Management
📚 References
- 1. RHDAustralia (ARF/RHD writing group). Australian guideline for prevention, diagnosis and management of acute rheumatic fever and rheumatic heart disease. 3rd edition. Darwin: Menzies School of Health Research; 2020.
- 2. Gewitz MH, Baltimore RS, Tani LY, et al. Revision of the Jones Criteria for the diagnosis of acute rheumatic fever in the era of Doppler echocardiography: a scientific statement from the American Heart Association. Circulation. 2015;131(20):1806–1818.
- 3. Australian Institute of Health and Welfare (AIHW). Rheumatic heart disease in Australia. Cat. no. CVD 87. Canberra: AIHW; 2023.
- 4. Parnaby MG, Carapetis JR. Rheumatic fever in Indigenous Australian children. J Paediatr Child Health. 2010;46(9):527–533.
- 5. Zühlke LJ, Steer AC. Estimates of the global burden of rheumatic heart disease. Glob Heart. 2013;8(3):185–192.
- 6. Karthikeyan G, Connolly SJ, Ntsekhe M, et al. The INVICTUS rheumatic heart disease research programme: rationale, design and baseline characteristics of a randomized trial of rivaroxaban compared with warfarin in patients with rheumatic heart disease and atrial fibrillation. Am Heart J. 2020;227:81–89.
- 7. Engelman D, Kado JH, Remenyi B, et al. Screening for rheumatic heart disease: quality and agreement of focused cardiac ultrasound by briefly trained health workers. BMC Cardiovasc Disord. 2016;16:30.
- 8. Wyber R, Taubert K, Marko S, Carapetis JR. Benzathine penicillin G for the management of RHD: concerns about feasibility and delivery, and opportunities for improvement. Int J Cardiol. 2013;166(2):279–286.
- 9. Francis JR, Gargan C, Remenyi B, et al. High rates of Group A streptococcal pharyngitis and acute rheumatic fever in Aboriginal children in the Northern Territory. Med J Aust. 2023;218(5):229–234.
- 10. National Heart Foundation of Australia and the Cardiac Society of Australia and New Zealand. Guidelines for the prevention, detection, and management of heart failure in Australia. 2018 (updated 2023).
- 11. National Health and Medical Research Council (NHMRC). Staying healthy: preventing infectious diseases in early childhood education and care services. 5th edition. Canberra: NHMRC; 2012.
- 12. Remenyi B, Wilson N, Steer A, et al. World Heart Federation criteria for echocardiographic diagnosis of rheumatic heart disease — an evidence-based guideline. Nat Rev Cardiol. 2012;9(5):297–309.