📋 Key Information Summary
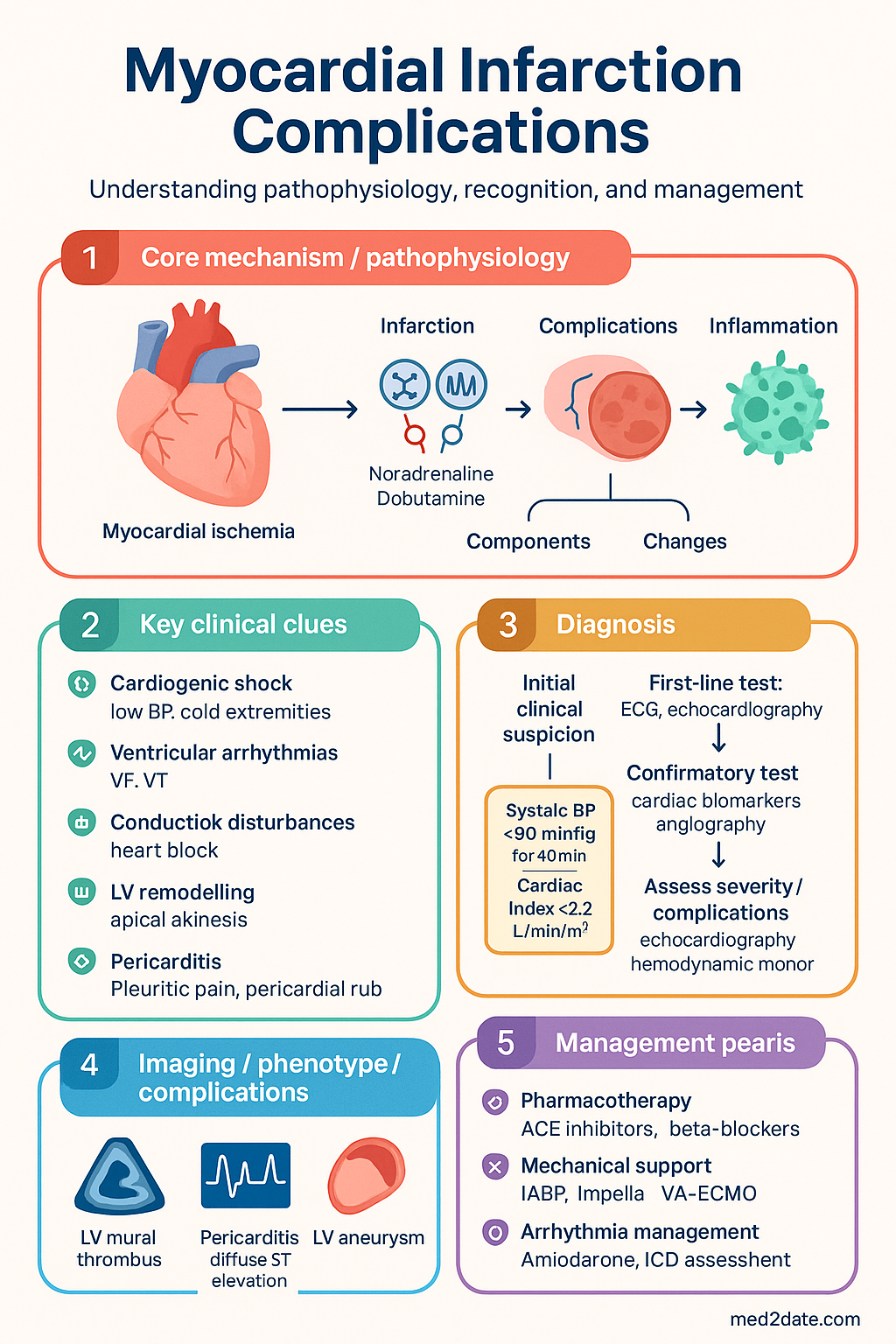
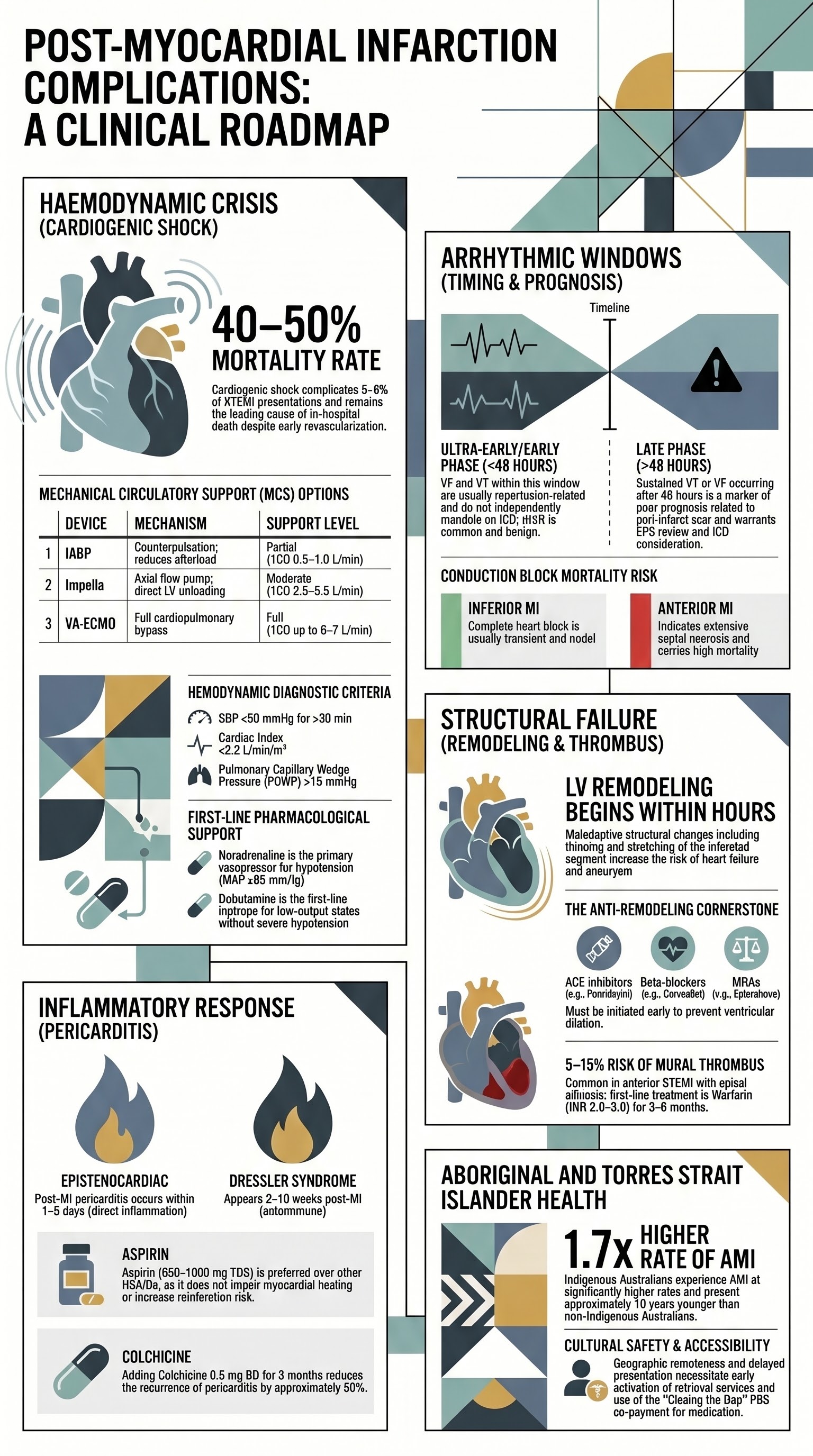
- Cardiogenic shock complicates 5–8% of STEMI presentations and carries mortality of 40–50% even with early revascularisation; haemodynamic criteria include systolic BP <90 mmHg for >30 min, cardiac index <2.2 L/min/m², and PCWP >18 mmHg.
- Noradrenaline is the first-line vasopressor in cardiogenic shock (SOAP II trial); dobutamine is the first-line inotrope for low-output states without severe hypotension.
- Mechanical circulatory support (MCS) — IABP is available in most Australian tertiary centres; Impella and VA-ECMO require specialist/cardiothoracic referral and are available at selected quaternary centres only.
- Ventricular fibrillation (VF) and sustained ventricular tachycardia (VT) in the first 48 hours post-MI are early arrhythmias (reperfusion-related) and do not independently mandate ICD; VT/VF beyond 48 hours warrants electrophysiology review and consideration of ICD.
- Complete heart block complicating inferior MI is usually transient (AV node level) and may require temporary pacing; anterior MI with new bundle branch block or complete block (His-Purkinje level) carries high mortality and often requires permanent pacing.
- LV remodelling begins within hours of large transmural infarction; ACE inhibitors (ramipril, perindopril), beta-blockers (carvedilol, bisoprolol), and mineralocorticoid receptor antagonists (eplerenone) are the cornerstone pharmacotherapy to prevent adverse remodelling.
- LV mural thrombus occurs in 5–15% of anterior STEMI with apical akinesis/dyskinesis; anticoagulation with warfarin (INR 2.0–3.0) for 3–6 months is first-line; DOACs are emerging but not yet standard of care for LV thrombus.
- Post-MI pericarditis (epistenocardiac pericarditis) occurs within 1–5 days and is treated with aspirin 650–1000 mg TDS; colchicine 0.5 mg BD is recommended as adjunctive therapy.
- Dressler syndrome (autoimmune pericarditis) occurs 2–10 weeks post-MI and is differentiated from recurrent ischaemia by pleuritic pain, pericardial rub, ST elevation (diffuse, concave-up), and elevated inflammatory markers.
- NSAIDs and corticosteroids should be avoided in post-MI pericarditis where possible due to risk of impaired myocardial healing and increased reinfarction risk; aspirin at high dose is preferred.
- Aboriginal and Torres Strait Islander Australians experience AMI at 1.7× the rate of non-Indigenous Australians and present later, with higher rates of cardiogenic shock and mechanical complications — culturally safe care pathways are essential.
- Transfer criteria — cardiogenic shock, refractory arrhythmias, need for MCS, and mechanical complications (VSD, papillary muscle rupture) require emergent transfer to a PCI-capable or cardiothoracic centre.
Introduction & Australian Epidemiology
Myocardial infarction (MI) remains a leading cause of morbidity and mortality in Australia. Despite significant advances in early reperfusion therapy — primary percutaneous coronary intervention (PCI) and fibrinolysis — complications of MI continue to impose a substantial clinical burden. Understanding the pathophysiology, early recognition, and evidence-based management of these complications is essential for optimising patient outcomes in Australian emergency departments, coronary care units, and cardiology wards.
In Australia, approximately 57,000 acute coronary syndrome (ACS) hospitalisations occur annually (AIHW 2023). ST-elevation myocardial infarction (STEMI) accounts for roughly 30% of ACS presentations. Complications of MI can be broadly categorised as:
- Haemodynamic — cardiogenic shock, mechanical complications (ventricular septal defect, free wall rupture, papillary muscle rupture)
- Arrhythmic — ventricular arrhythmias, conduction disturbances, atrial fibrillation
- Structural — LV remodelling, aneurysm formation, mural thrombus
- Inflammatory — pericarditis, Dressler syndrome
The in-hospital mortality for STEMI in Australia is approximately 5–7% with contemporary management (ACSQA data). However, cardiogenic shock carries mortality rates of 40–50%, and mechanical complications such as ventricular septal defect or free wall rupture remain lethal without emergent surgical intervention.
Cardiogenic Shock
Definition & Haemodynamic Criteria
Cardiogenic shock is defined as a state of critical end-organ hypoperfusion resulting from severe impairment of cardiac pump function. It is the leading cause of in-hospital death following acute MI.
| Parameter | Diagnostic Criterion |
|---|---|
| Systolic BP | <90 mmHg for >30 min, or vasopressors required to maintain ≥90 mmHg |
| Cardiac index (CI) | <2.2 L/min/m² |
| Pulmonary capillary wedge pressure (PCWP) | >18 mmHg |
| End-organ signs | Altered mental status, cold clammy extremities, urine output <30 mL/hr, lactate >2 mmol/L |
| Echocardiographic EF | Typically <30% (not mandatory for diagnosis) |
Vasopressor & Inotrope Selection
Pharmacological haemodynamic support should be initiated early while arranging revascularisation. The choice of vasoactive agent depends on blood pressure, cardiac output, and systemic vascular resistance.
Mechanical Circulatory Support (MCS)
When pharmacological therapy is insufficient, mechanical circulatory support should be considered. Availability of specific devices varies across Australian centres, and early consultation with a cardiothoracic/heart failure centre is essential.
| Device | Mechanism | Support Level | Availability in Australia |
|---|---|---|---|
| IABP (Intra-Aortic Balloon Pump) | Counterpulsation — augments diastolic coronary perfusion, reduces afterload | Partial (↑CO 0.5–1.0 L/min) | Most tertiary cardiac centres (Royal Melbourne, RPAH, Alfred, Prince Charles, Flinders, Fiona Stanley) |
| Impella (CP/5.5) | Percutaneous axial flow pump across aortic valve; provides direct LV unloading | Moderate (↑CO 2.5–5.5 L/min depending on model) | Limited — selected quaternary centres; increasing availability |
| VA-ECMO (Veno-Arterial Extracorporeal Membrane Oxygenation) | Complete cardiopulmonary bypass; provides full circulatory and respiratory support | Full (↑CO up to 6–7 L/min) | ECMO retrieval services (e.g., Alfred ECMO, Royal Prince Alfred, Prince Charles, St Vincent's Melbourne); retrieval from regional centres via dedicated teams |
| LVAD (Left Ventricular Assist Device) | Surgically implanted chronic mechanical support | Full (bridge to transplant/recovery) | Heart transplant centres only (St Vincent's Sydney, Alfred Melbourne, Prince Charles Brisbane) |
Emergency Revascularisation
Early revascularisation remains the most important intervention in cardiogenic shock complicating MI. The SHOCK trial demonstrated a significant 6-month mortality benefit with early PCI or CABG compared to initial medical stabilisation (50.3% vs 63.1%). In Australia, this mandates emergent transfer to a PCI-capable facility if the presenting hospital does not have catheterisation laboratory access.
Arrhythmic Complications
Classification by Timing
Arrhythmias are the most common complication of acute MI and a leading cause of early mortality. They are classified by timing relative to the infarct event, which has important prognostic and therapeutic implications.
| Timing | Window | Common Arrhythmias | Mechanism | Prognostic Implication |
|---|---|---|---|---|
| Ultra-early | <2 hours | VF, VT, sinus bradycardia (inferior MI) | Acute ischaemia, vagal activation, reperfusion injury | High in-hospital mortality; does NOT independently mandate ICD if reversible |
| Early | 2–48 hours | VT, VF, AF, accelerated idioventricular rhythm (AIVR) | Reperfusion arrhythmias, electrolyte shifts, catecholamine surge | AIVR is benign (reperfusion marker); VF/VT in this window generally do not mandate ICD |
| Late (>48 hrs) | >48 hours to discharge | Sustained VT, VF, complete heart block | Peri-infarct scar, re-entrant circuits, progressive conduction system fibrosis | Poor prognosis marker; warrants EPS and ICD consideration per ESC/AHA guidelines |
Ventricular Arrhythmias Post-MI
Ventricular Fibrillation (VF) & Pulseless VT
Management follows standard ALS protocols (Australian Resuscitation Council Guideline 11.2). Early defibrillation is the definitive treatment.
- Immediate: Defibrillation (biphasic 150–200 J, then escalating). Commence CPR if not immediately successful.
- Adrenaline 1 mg IV every 3–5 minutes during cardiac arrest (ALS protocol).
- Amiodarone 300 mg IV bolus for refractory VF/pulseless VT, followed by 150 mg IV if recurrent.
- Correct reversible causes: Hypokalaemia (target K⁺ >4.0 mmol/L), hypomagnesaemia (MgSO₄ 2 g IV), acidosis, hypoxia.
Sustained Monomorphic VT (Haemodynamically Stable)
ICD Indications Post-MI
Implantable cardioverter-defibrillator (ICD) placement for primary prevention should not be considered during the acute admission. Assessment occurs at 6–12 weeks post-MI once optimal medical therapy is established and LV function is reassessed.
- Primary prevention: LVEF ≤35% at ≥6–12 weeks post-MI despite optimal medical therapy (ACEi/ARB + beta-blocker + MRA) — refer for ICD assessment (ESC Class I, NHFA/CSANZ consensus).
- Secondary prevention: Survived cardiac arrest not due to reversible cause, sustained VT not within 48 hours of MI — ICD indicated.
- EPS-guided: If LVEF 36–40% with NYHA II–III and additional risk factors (non-sustained VT, positive EPS) — consider ICD.
Conduction Disturbances & Temporary Pacing
| Conduction Disturbance | MI Location | Level of Block | Prognosis | Pacing Indication |
|---|---|---|---|---|
| 1st-degree AV block | Any | AV node | Benign (monitor) | None unless symptomatic |
| 2nd-degree Type I (Wenckebach) | Inferior | AV node | Usually transient, benign | If HR <50 with symptoms (transcutaneous pacing standby) |
| 2nd-degree Type II (Mobitz II) | Anterior | His-Purkinje | May progress to complete block; ominous | Temporary transvenous pacing — prophylactic |
| Complete heart block (CHB) | Inferior | AV node | Usually transient (1–2 weeks), narrow QRS escape | If HR <40, haemodynamic compromise, or ventricular escape >3 sec pause — temporary pacing |
| Complete heart block (CHB) | Anterior | His-Purkinje | High mortality (extensive septal necrosis); wide QRS escape | Immediate temporary transvenous pacing; likely permanent pacemaker required |
| New bundle branch block (RBBB ± LAFB/LPFB) | Anterior | His-Purkinje | High risk of progression to CHB; marker of large infarct | Prophylactic temporary pacing if alternating bundle branch block or associated with CHB |
Temporary Pacing — Technical Considerations
- Transcutaneous pacing (Zoll/defibrillator pads): Immediate, non-invasive; suitable for bridge to transvenous pacing or as sole therapy in transient bradycardia. Sedation/analgesia required (fentanyl 25–50 mcg IV + midazolam 1–2 mg IV).
- Transvenous pacing (right internal jugular or left subclavian approach): Inserted under fluoroscopy or echocardiographic guidance in catheterisation laboratory or ICU. Required for prolonged (>5–7 days) AV block, His-Purkinje block, or haemodynamically unstable bradycardia unresponsive to transcutaneous pacing.
- Permanent pacemaker: Considered if AV block persists >14 days post-inferior MI, or if His-Purkinje block persists beyond the acute phase.
Post-MI Ventricular Dysfunction
Left Ventricular Remodelling
LV remodelling is the structural and functional adaptation of the left ventricle following myocardial infarction. It begins within hours of the ischaemic event and may continue for months to years. Remodelling is initially adaptive (maintaining stroke volume) but becomes maladaptive, leading to progressive ventricular dilation, sphericity, and ultimately heart failure.
Pathophysiology
- Infarct expansion: Thinning and stretching of the infarcted myocardial segment (first 72 hours); greatest risk with large transmural anterior MI.
- Compensatory hypertrophy: Non-infarcted segments undergo eccentric hypertrophy to maintain cardiac output.
- Ventricular dilation: Progressive increase in end-diastolic and end-systolic volumes; spherical geometry increases wall stress (Laplace law).
- Neurohormonal activation: RAAS activation, sympathetic nervous system upregulation, and inflammatory cytokines drive ongoing remodelling and fibrosis.
Pharmacological Prevention of Remodelling
LV Aneurysm Formation
A true LV aneurysm is a localised area of thinned, scarred myocardium that bulges during systole and diastole. It typically develops 4–8 weeks post-large transmural anterior MI.
- Incidence: 5–10% of anterior STEMI in the primary PCI era (lower than historical rates of 10–35%).
- Diagnosis: Echocardiography (parasternal and apical views); cardiac MRI with late gadolinium enhancement is gold standard for characterising scar and aneurysm extent.
- ECG findings: Persistent ST elevation in anterior leads beyond 2 weeks post-MI (differentiate from acute ischaemia).
- Complications: Heart failure, ventricular arrhythmias (re-entrant circuits within scar), mural thrombus, systemic thromboembolism.
- Management: Pharmacological (ACEi, beta-blockers, diuretics); surgical ventricular restoration (Dor procedure) for refractory heart failure or recurrent VT; ICD for VT not amenable to ablation.
LV Mural Thrombus
Left ventricular mural thrombus is a common complication of anterior STEMI, particularly when there is apical akinesis or dyskinesis. The incidence has decreased with contemporary anticoagulation and early reperfusion but remains clinically important.
| Feature | Detail |
|---|---|
| Incidence | 5–15% of anterior STEMI (higher with large infarcts, apical akinesis/dyskinesis) |
| Diagnostic modality | Transthoracic echo (sensitivity 60%); contrast echo or cardiac MRI (sensitivity >90%) if suboptimal acoustic windows |
| Thromboembolic risk | Up to 10% risk of stroke/peripheral embolisation if untreated |
| First-line anticoagulation | Warfarin (INR 2.0–3.0) for 3–6 months; repeat echo at 3 months to assess thrombus resolution |
| DOACs | Emerging evidence (WATCHMAN-like data, case series); not yet standard of care for LV thrombus in Australian guidelines; may be considered if warfarin contraindicated (Haematology/EP consult) |
| Triple therapy | If concurrent PCI with stent: aspirin + clopidogrel + warfarin (shortest duration possible, typically 1–3 months), then dual therapy (clopidogrel + warfarin) for remainder, then warfarin alone. Bleeding risk is high — PPI co-prescribe. |
Newer Therapies for LV Dysfunction — SGLT2 Inhibitors
SGLT2 inhibitors (dapagliflozin, empagliflozin) are now established in HFrEF management and are increasingly used in the post-MI setting where LV dysfunction develops.
Pericarditis & Dressler Syndrome
Classification
Pericardial inflammation following MI is classified into two distinct entities based on timing and pathophysiology:
| Feature | Post-MI (Epistenocardiac) Pericarditis | Dressler Syndrome |
|---|---|---|
| Timing | 1–5 days post-MI | 2–10 weeks post-MI (weeks to months) |
| Mechanism | Direct inflammation of pericardium adjacent to infarcted myocardium | Autoimmune (anti-myocardial antibodies); systemic inflammatory response |
| Incidence | 10–20% (decreased with early reperfusion) | 1–5% (rare in the primary PCI era) |
| Pericardial rub | Present in ~30–85% | Common |
| Effusion risk | Small–moderate effusion common; tamponade rare | Moderate–large effusion; tamponade possible |
Diagnostic Criteria
Diagnosis of post-MI pericarditis requires at least 2 of the following 4 criteria:
- Pleuritic chest pain — sharp, positional (worse supine, better leaning forward), distinct from ischaemic pain
- Pericardial friction rub — high-pitched, scratchy, best heard at left sternal border with diaphragm during end-expiration
- ECG changes — diffuse concave-upward ST elevation (not in a single coronary territory), PR depression (most specific in lead II), or new/worsening pericardial effusion on echo
- Inflammatory markers — elevated CRP and/or ESR; WBC may be elevated
| Feature | Post-MI Pericarditis | Recurrent Ischaemia / Reinfarction |
|---|---|---|
| Pain character | Sharp, pleuritic, positional | Crushing, pressure, retrosternal |
| ECG | Diffuse concave ST elevation, PR depression | Territorial ST elevation/depression, reciprocal changes |
| Troponin | Mildly elevated (from index MI or myopericarditis) — no re-elevation pattern | Rise and fall pattern consistent with acute MI |
| CRP | Elevated | Usually normal early |
| Friction rub | Present | Absent |
| Echo | Pericardial effusion; preserved regional wall motion | New or worsening wall motion abnormality |
Treatment Protocols
First-Line Therapy
Medications to AVOID
- NSAIDs (ibuprofen, naproxen, indomethacin) — impair myocardial scar formation, increase risk of myocardial rupture in the early post-MI period, and may increase reinfarction risk (with the exception of aspirin at anti-inflammatory doses).
- Corticosteroids (prednisolone, dexamethasone) — impair myocardial healing, increase risk of ventricular wall thinning and aneurysm formation; should only be used as last resort for refractory pericarditis not responsive to aspirin + colchicine.
- Anticoagulants in the setting of pericarditis — increased risk of haemopericardium and tamponade. If anticoagulation is required (e.g., LV thrombus, AF), use with caution and monitor closely for pericardial effusion development.
Second-Line / Refractory Therapy
- Ibuprofen 600 mg TDS + colchicine 0.5 mg BD — reserved for patients without LV dysfunction and not at risk of myocardial rupture (generally >4 weeks post-MI).
- IL-1 receptor antagonist (anakinra) — for recurrent, corticosteroid-dependent pericarditis; requires specialist (cardiology/rheumatology) initiation; not PBS-listed for this indication.
- Pericardiocentesis — for large effusion with haemodynamic compromise (tamponade) or diagnostic uncertainty (rule out purulent pericarditis).
Cardiac Rehabilitation Considerations
Exercise should be restricted during the acute phase of post-MI pericarditis. Patients may participate in Phase II cardiac rehabilitation once symptoms have resolved, inflammatory markers have normalised, and there is no significant pericardial effusion on repeat echocardiography. Typically this means a delay of 2–4 weeks from symptom resolution.
Special Populations
Pregnancy
Paediatrics
Elderly (≥75 years)
Renal Impairment
Hepatic Impairment
Immunocompromised
Aboriginal and Torres Strait Islander Health
Aboriginal and Torres Strait Islander Australians experience acute myocardial infarction at approximately 1.7 times the rate of non-Indigenous Australians (AIHW 2023). The burden is disproportionately high in remote and very remote communities, where access to PCI-capable centres, mechanical circulatory support, and cardiothoracic surgery is limited. The median age of first AMI in Indigenous Australians is approximately 10 years younger than in non-Indigenous Australians, and in-hospital mortality is significantly higher.
📚 References
- 1. Amsterdam EA, Wenger NK, Brindis RG, et al. 2014 AHA/ACC guideline for the management of patients with non-ST-elevation acute coronary syndromes. J Am Coll Cardiol. 2014;64(24):e139–e228.
- 2. Ibanez B, James S, Agewall S, et al. 2017 ESC guidelines for the management of acute myocardial infarction in patients presenting with ST-segment elevation. Eur Heart J. 2018;39(2):119–177.
- 3. Hochman JS, Sleeper LA, Webb JG, et al. Early revascularization and long-term survival in cardiogenic shock complicating acute myocardial infarction. JAMA. 2006;295(21):2511–2515.
- 4. Thiele H, Zeymer U, Neumann FJ, et al. Intraaortic balloon support for myocardial infarction with cardiogenic shock. N Engl J Med. 2012;367(14):1287–1296.
- 5. De Backer D, Biston P, Devriendt J, et al. Comparison of dopamine and norepinephrine in the treatment of shock. N Engl J Med. 2010;362(9):779–789.
- 6. Pfeffer MA, Braunwald E, Moyé LA, et al. Effect of captopril on mortality and morbidity in patients with left ventricular dysfunction after myocardial infarction: results of the Survival and Ventricular Enlargement trial. N Engl J Med. 1992;327(10):669–677.
- 7. Pitt B, Remme W, Zannad F, et al. Eplerenone, a selective aldosterone blocker, in patients with left ventricular dysfunction after myocardial infarction. N Engl J Med. 2003;348(14):1309–1321.
- 8. Dargie HJ. Effect of carvedilol on outcome after myocardial infarction in patients with left-ventricular dysfunction: the CAPRICORN randomised trial. Lancet. 2001;357(9266):1385–1390.
- 9. Imazio M, Bobbio M, Cecchi E, et al. Colchicine in addition to conventional therapy for acute pericarditis: results of the COlchicine for acute PEricarditis (COPE) trial. Circulation. 2005;112(13):2012–2016.
- 10. Imazio M, Brucato A, Cemin R, et al. A randomized trial of colchicine for acute pericarditis. N Engl J Med. 2013;369(16):1522–1528.
- 11. McCarthy JJ, Boehmer JP, Hruban RH, et al. Long-term outcome of fulminant myocarditis as compared with acute (nonfulminant) myocarditis. N Engl J Med. 2000;342(10):690–695.
- 12. Australian Institute of Health and Welfare. Acute coronary syndrome (ACS) data snapshots. AIHW: Canberra; 2023.
- 13. Chew DP, Briffa TG, Alhammad NJ, et al. Acute coronary syndrome care across Australia and New Zealand: the SNAPSHOT ACS study. Med J Aust. 2015;202(4):185–189.
- 14. National Heart Foundation of Australia and Cardiac Society of Australia and New Zealand. Australian clinical guidelines for the management of acute coronary syndromes 2023. Heart Lung Circ. 2023;32(8):919–967.
- 15. McMurray JJ, Packer M, Desai AS, et al. Angiotensin–neprilysin inhibition versus enalapril in heart failure. N Engl J Med. 2014;371(11):993–1004.
- 16. McMurray JJV, Solomon SD, Inzucchi SE, et al. Dapagliflozin in patients with heart failure and reduced ejection fraction. N Engl J Med. 2019;381(21):1995–2008.
- 17. Spencer FA, Meyer TE, Gore JM, Goldberg RJ. Heterogeneity in the management and outcomes of patients with acute myocardial infarction complicated by heart failure: the National Registry of Myocardial Infarction. Circulation. 2002;105(22):2605–2610.
- 18. Respiratory and Critical Care Medicine (ANZICS) ECMO Registry Steering Committee. ANZICS ECMO Registry Annual Report. Melbourne: ANZICS; 2023.
- 19. Al-Khatib SM, Stevenson WG, Ackerman MJ, et al. 2017 AHA/ACC/HRS guideline for management of patients with ventricular arrhythmias and the prevention of sudden cardiac death. J Am Coll Cardiol. 2018;72(14):e91–e220.
- 20. Australian Institute of Health and Welfare. The health and welfare of Australia's Aboriginal and Torres Strait Islander peoples 2023. AIHW: Canberra; 2023.