📋 Key Information Summary
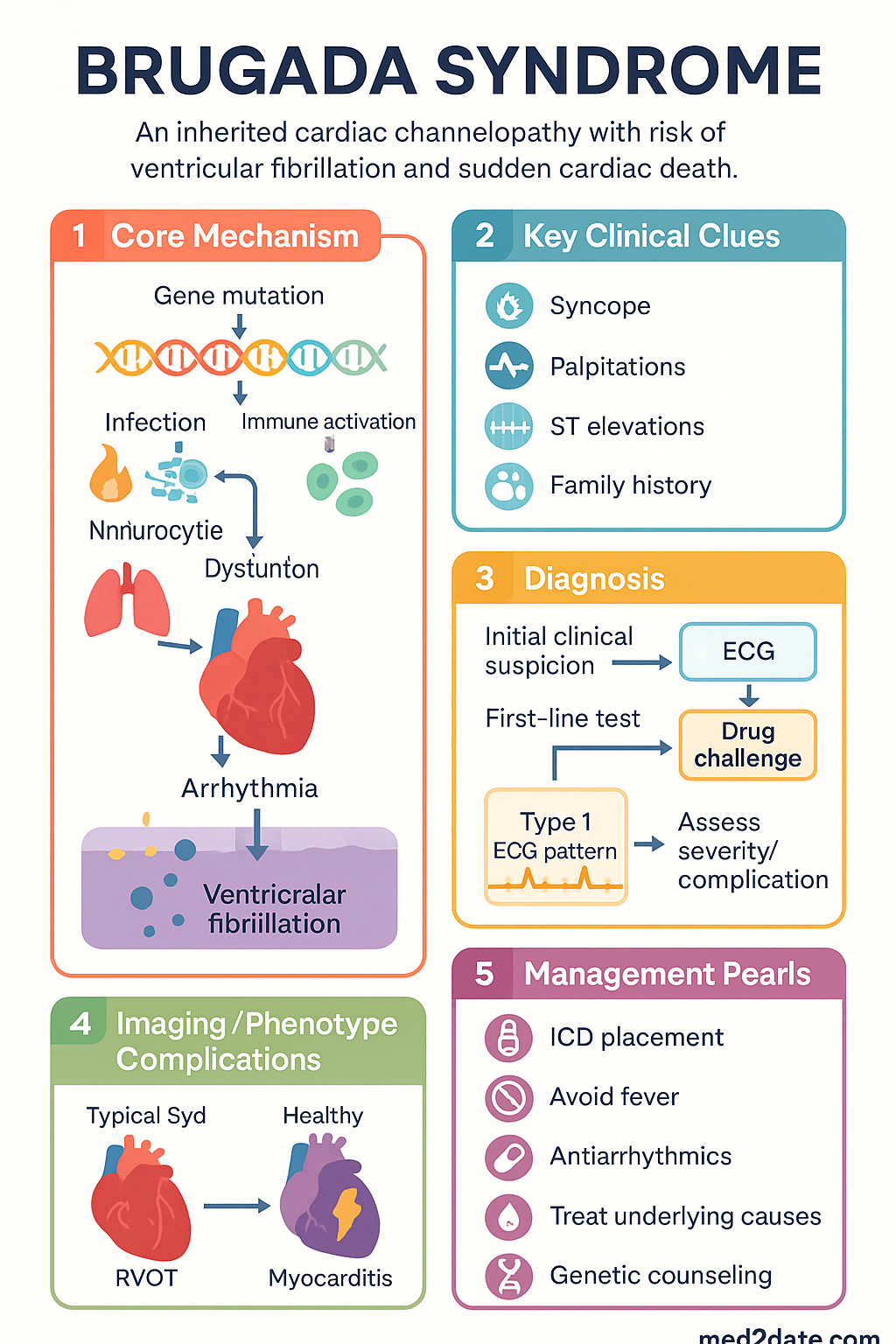
- Brugada syndrome is an autosomal dominant inherited cardiac channelopathy caused predominantly by loss-of-function mutations in the SCN5A gene encoding the cardiac sodium channel (Nav1.5), resulting in a propensity for ventricular fibrillation (VF) and sudden cardiac death (SCD).
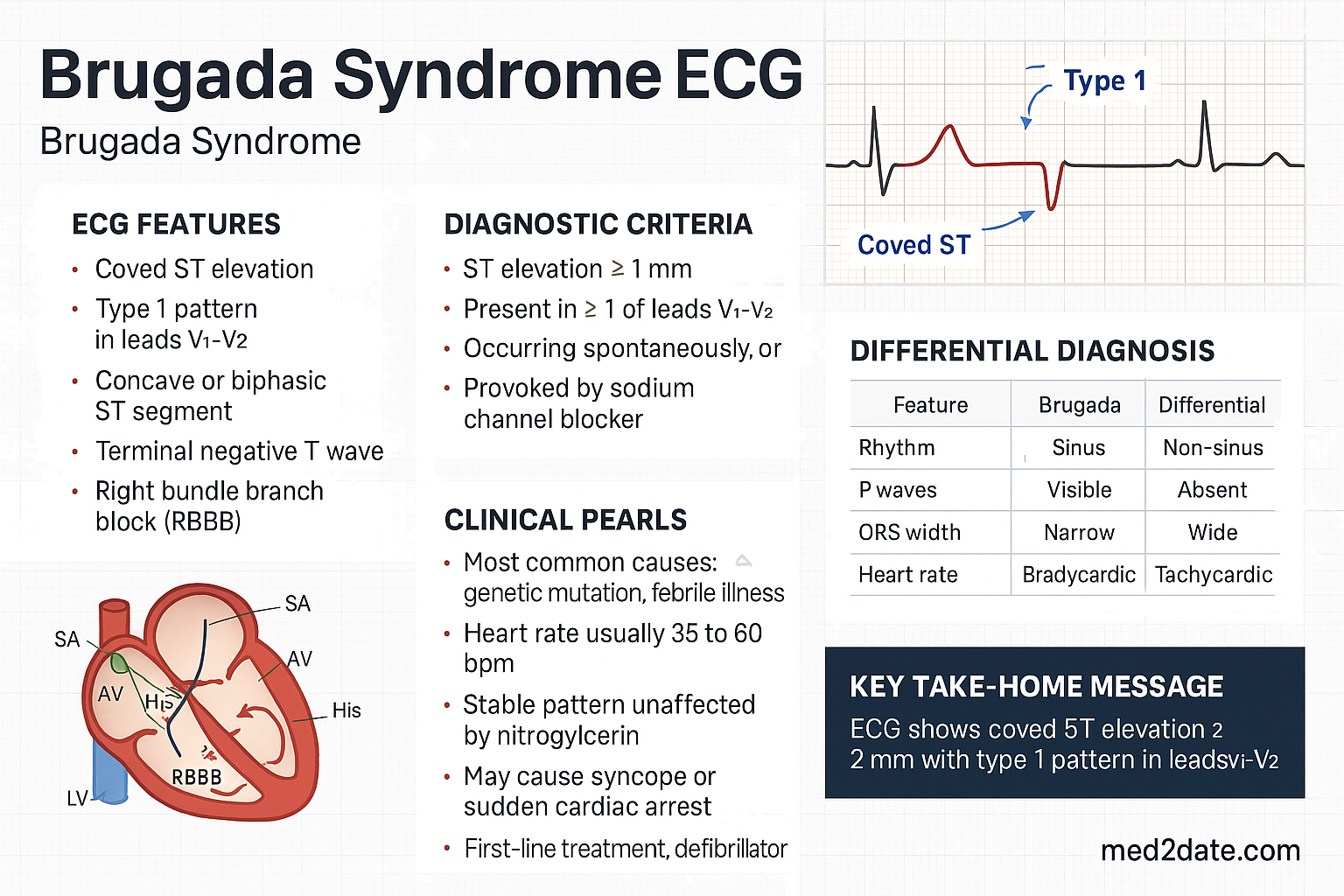
- The hallmark diagnostic finding is a coved-type ST elevation ≥2 mm in the right precordial leads (V1–V3) followed by a negative T wave — the Type 1 (previously coved-type) ECG pattern. class="guideline-li">Type 2 (saddle-back) and Type 3 (non-specific ST elevation) patterns are not diagnostic in isolation and require provocation testing with sodium-channel blockers (e.g., ajmaline 1 mg/kg IV over 10 min) to unmask a Type 1 pattern.
- Risk stratification centres on the presence of a spontaneous Type 1 ECG pattern, prior arrhythmic syncope, and electrophysiology study (EPS) inducibility, though EPS remains controversial.
- Asymptomatic patients with a drug-induced Type 1 pattern have a low annual event rate (<0.5%) and generally require observation only.
- An implantable cardioverter-defibrillator (ICD) is the cornerstone of SCD prevention in patients with aborted cardiac arrest, sustained ventricular arrhythmia, or haemodynamically significant syncope attributable to ventricular arrhythmia.
- Quinidine (a class Ia antiarrhythmic and IKACh blocker) is the primary pharmacological option for recurrent VF storms, patients refusing or not meeting ICD criteria, and as adjunctive therapy post-ICD shock.
- Catheter ablation targeting epicardial substrate in the right ventricular outflow tract (RVOT) is an emerging and increasingly effective intervention, particularly in patients with recurrent VT/VF.
- All patients must receive education on fever management (aggressive antipyretics), avoidance of Brugada-contraindicated drugs (www.brugadadrugs.org), and alcohol excess — common triggers of arrhythmic events.
- Genetic testing should be offered to first-degree relatives of index cases with confirmed SCN5A mutations; cascade family screening with serial ECGs is essential for all first-degree relatives.
- Aboriginal and Torres Strait Islander populations may face delayed diagnosis due to limited access to specialist cardiology services and electrophysiology studies, particularly in remote and regional areas.
Introduction & Australian Epidemiology
Brugada syndrome (BrS) is a heritable cardiac channelopathy characterised by distinctive ST-segment changes in the right precordial electrocardiogram leads (V1–V3) and an elevated risk of ventricular fibrillation (VF) and sudden cardiac death (SCD). First described by the Brugada brothers in 1992, the syndrome has since become recognised as one of the most important causes of structurally normal-heart SCD, particularly in young males of Southeast Asian descent.
Brugada syndrome accounts for approximately 20% of sudden unexplained death syndrome (SUDS) cases and up to 12–20% of SCD cases in individuals with structurally normal hearts at autopsy. The estimated worldwide prevalence of the Brugada ECG pattern is 0.1–0.5% in Western populations, rising to 1–5% in Southeast Asian countries. In Australia, the condition is encountered across all ethnic backgrounds, though the highest prevalence of the diagnostic ECG pattern is observed in individuals of Southeast Asian and Polynesian heritage. Australian data suggest the prevalence of a diagnostic Type 1 pattern in the general Australian population is approximately 0.12–0.4%, consistent with international estimates.
The male-to-female ratio for clinical diagnosis is approximately 8–10:1, likely reflecting hormonal modulation of the transient outward potassium current (Ito) and differences in right ventricular outflow tract (RVOT) electrophysiology. The median age at diagnosis is 35–45 years, though the condition can present at any age, including infancy.
Genetics & Pathophysiology (SCN5A Mutation)
Inheritance Pattern
Brugada syndrome is inherited in an autosomal dominant pattern with incomplete penetrance and variable expressivity. This means that approximately 50% of first-degree relatives of an affected individual will carry the pathogenic variant, but not all carriers will manifest the clinical phenotype. Male predominance in clinical expression is well established.
SCN5A and the Cardiac Sodium Channel
Mutations in the SCN5A gene (chromosome 3p21) encoding the α-subunit of the cardiac voltage-gated sodium channel (Nav1.5) account for approximately 20–30% of clinically diagnosed Brugada syndrome cases. Over 300 SCN5A mutations have been identified, predominantly missense mutations leading to loss-of-function of the sodium current (INa).
Loss of INa produces the Brugada phenotype through the repolarisation hypothesis and the depolarisation hypothesis:
- Repolarisation hypothesis: Reduced INa in the RVOT epicardium unmasks the transient outward potassium current (Ito), creating a transmural voltage gradient between epicardium and endocardium during phase 1 of the action potential. This produces the characteristic ST elevation and creates a substrate for phase 2 re-entry, which can degenerate into VF.
- Depolarisation hypothesis: Reduced INa causes conduction delay in the RVOT, resulting in delayed activation and ST-segment elevation through partial right bundle branch block-like effects. Slowed conduction creates a substrate for re-entrant arrhythmias.
- Both mechanisms may coexist, with the RVOT being the critical anatomical region due to its naturally high Ito density and heterogeneous expression of ion channels.
Additional Gene Loci
Mutations in other genes encoding ion channel subunits and regulatory proteins have been implicated in smaller subsets of BrS:
| Gene | Protein / Channel | Functional Effect | Frequency |
|---|---|---|---|
| SCN5A | Nav1.5 (INa) | ↓ INa | 20–30% |
| SCN1B | β1-subunit | ↓ INa | Rare |
| CACNA1C | Cav1.2 (ICa,L) | ↓ ICa,L | Rare |
| CACNB2 | Cavβ2 subunit | ↓ ICa,L | Rare |
| KCNE3 | MiRP2 (Ito) | ↑ Ito | Rare |
| KCNJ8 | Kir6.1 (IK-ATP) | ↑ IK-ATP | Rare |
| HEY2 | Transcription factor | RVOT development | GWAS locus |
In approximately 60–70% of BrS cases, no pathogenic variant is identified on current genetic testing panels. Genetic testing, when performed, should include at minimum SCN5A; expanded panels may include the additional loci listed above. Genetic testing is available through major Australian genetic testing laboratories (e.g., Sonic Genetics, Victorian Clinical Genetics Services) and is Medicare-rebatable under MBS item 73307 where clinical criteria are met.
Genotype-Phenotype Correlations
SCN5A-positive patients tend to exhibit greater PR prolongation, more conduction abnormalities, and a higher rate of atrial fibrillation than SCN5A-negative patients.
Triggers and Modulators
The Brugada ECG pattern and arrhythmic events are often unmasked or exacerbated by:
- Fever: The most common trigger; fever ≥38°C increases Ito density and further reduces INa, widening the transmural gradient.
- Drugs: Sodium-channel blockers, tricyclic antidepressants, lithium, cocaine, anaesthetic agents (propofol, bupivacaine), and others listed at www.brugadadrugs.org.
- Vagal stimulation: Increased vagal tone during sleep (nocturnal predominance of events), postprandial states, and alcohol excess.
- Hypokalaemia, hyperkalaemia, and hypothermia.
Diagnostic ECG Patterns (Type 1, 2, 3)
ECG Criteria
The diagnostic criteria for Brugada syndrome are centred on the morphology of the ST segment in the right precordial leads V1–V3, ideally recorded from the 2nd, 3rd, and 4th intercostal spaces (high V1–V3 positions) in addition to standard positions.
| Pattern | ST-T Morphology | ST Elevation | T Wave | Diagnostic? |
|---|---|---|---|---|
| Type 1 (Coved) | Coved / upward convexity, gradually descending | ≥2 mm at J-point | Negative | Yes — diagnostic |
| Type 2 (Saddle-back) | Saddle-back / concave upward with a high take-off | ≥2 mm at high take-off, ≥0.5 mm at J-point | Positive or biphasic | Not diagnostic alone — requires ajmaline challenge |
| Type 3 (Non-specific) | Coved or saddle-back morphology | <2 mm | Variable | Not diagnostic alone — requires ajmaline challenge |
Diagnostic Criteria (Brugada Consensus, 2013)
A diagnosis of Brugada syndrome requires a Type 1 ECG pattern (spontaneous or drug-induced) plus at least one of the following:
- Documented ventricular fibrillation or polymorphic ventricular tachycardia
- Self-terminating polymorphic VT or VF
- A family history of SCD (<45 years) in a first-degree relative
- Type 1 ECG pattern in family members
- Arrhythmic syncope (nocturnal agonal respiration)
- Inducibility of VT/VF on electrophysiology study
Pharmacological Provocation Testing
When a Type 2 or Type 3 ECG pattern is identified, a sodium-channel blocker challenge may unmask a Type 1 pattern. Testing must be performed in a monitored setting with continuous ECG and haemodynamic monitoring, with defibrillation capability immediately available.
ECG Modifiers
- Record ECGs in multiple right precordial positions (V1–V3 at 2nd, 3rd, and 4th intercostal spaces) to increase diagnostic yield.
- Repeat ECGs during febrile episodes and at different times of day (nocturnal vagal predominance may unmask pattern).
- Signal-averaged ECG (SAECG) may reveal late potentials, particularly in SCN5A-positive patients.
- Baseline PR prolongation and QRS widening are more common in SCN5A carriers.
Clinical Presentation & Diagnostic Criteria
Typical Presentations
- Sudden cardiac arrest (SCA) / VF: Approximately 4–12% of BrS patients present with aborted SCA as the first manifestation.
- Syncope: Arrhythmic syncope, often nocturnal or occurring at rest, is the most common symptomatic presentation. Nocturnal agonal respiration (gasping during sleep reported by bed partner) is a key historical feature.
- Palpitations: May reflect atrial fibrillation (present in 10–20% of BrS patients) or ventricular ectopy.
- Asymptomatic ECG detection: An increasing proportion of patients are identified incidentally or through family screening.
- SIDS / SUADS: BrS has been implicated in sudden infant death syndrome and sudden unexplained death in the young.
Differential Diagnosis
The Type 1 ECG pattern must be distinguished from other causes of right precordial ST elevation:
- Right bundle branch block (RBBB) — typically without coved ST morphology
- Acute anterior STEMI / coronary vasospasm
- Arrhythmogenic right ventricular cardiomyopathy (ARVC)
- Right ventricular hypertrophy / acute right heart strain (e.g., pulmonary embolism)
- Early repolarisation pattern
- Pericarditis / myocarditis
- Hyperkalaemia, hypothermia
- Duchenne muscular dystrophy
- Mechanical mediastinal compression (thymoma, mediastinal haematoma)
An echocardiogram and cardiac MRI should be performed to exclude structural heart disease (especially ARVC) before confirming a BrS diagnosis.
Formal Diagnostic Criteria (2023 HRS/EHRA/APHRS Expert Consensus)
- Spontaneous or drug-induced Type 1 ECG pattern in ≥1 right precordial lead (V1–V3), recorded from standard or superior (2nd/3rd intercostal space) positions, AND
- At least one clinical criterion: (a) documented VF or polymorphic VT; (b) arrhythmic syncope; (c) nocturnal agonal respiration; (d) family history of SCD or Type 1 pattern in first-degree relatives; (e) inducible VT/VF at EPS in selected cases.
Investigations
The following investigations are recommended in the workup of suspected Brugada syndrome:
Risk Stratification
Risk stratification in Brugada syndrome remains challenging and is an area of active research. The following framework is based on the 2022 ESC and 2023 HRS/EHRA/APHRS guidelines:
Key Risk Factors
| Risk Factor | Evidence | Role |
|---|---|---|
| Prior SCA / VF | Recurrence rate 10–15%/year | Strongest risk factor — ICD indicated |
| Arrhythmic syncope | Event rate 1.5–3%/year | ICD indicated if truly arrhythmic |
| Spontaneous Type 1 ECG | 5–7× increased risk vs drug-induced | Major risk modifier |
| EPS inducibility | Controversial; PRELUDE, FINGER registries | May assist in borderline cases |
| Male sex | Higher event rates | Consider in risk-benefit assessment |
| SCN5A mutation | Does not independently predict events | Useful for cascade screening, not ICD decisions |
| Fragmented QRS / late potentials | Emerging data | Research interest |
Management (ICD, Quinidine, Ablation)
1. Implantable Cardioverter-Defibrillator (ICD)
The ICD remains the cornerstone of sudden cardiac death prevention in Brugada syndrome. It is the only intervention with proven mortality benefit in high-risk patients.
- Survivors of cardiac arrest (aborted SCA with documented VF/PMVT)
- Patients with documented sustained VT causing haemodynamic compromise
- Arrhythmic syncope in a patient with spontaneous Type 1 ECG pattern
- Asymptomatic patients with spontaneous Type 1 ECG and inducible VF at EPS
- Nocturnal agonal respiration with spontaneous Type 1 pattern
Australian considerations: ICD implantation is performed at all major tertiary cardiac centres and is covered under standard hospital funding. Single-chamber ICD (VVI) is preferred in young patients to minimise lead-related complications and tricuspid valve interference. Subcutaneous ICD (S-ICD) may be considered to avoid transvenous lead complications in younger patients without pacing indications. Post-implantation, regular device clinic follow-up is essential (typically 3–6 monthly).
2. Quinidine
Quinidine is the primary pharmacological therapy for Brugada syndrome. It blocks the transient outward potassium current (Ito), thereby reducing the transmural voltage gradient that underlies the Brugada ECG pattern and arrhythmogenesis.
Indications for quinidine:
- Adjunctive therapy in patients with recurrent appropriate ICD shocks (VF storm)
- Primary therapy in patients who refuse ICD implantation or are not candidates
- Asymptomatic patients with spontaneous Type 1 ECG and additional risk factors (consideration)
- Treatment and prevention of atrial fibrillation in BrS patients
- Children with BrS and arrhythmic events (paediatric dosing under specialist supervision)
3. Catheter Ablation
Epicardial catheter ablation of the arrhythmogenic substrate in the right ventricular outflow tract (RVOT) has emerged as an effective intervention for Brugada syndrome, particularly in patients with recurrent VT/VF despite ICD and quinidine therapy.
Procedural details:
- Approach: Combined epicardial (percutaneous subxiphoid) and endocardial mapping and ablation.
- Target: Low-voltage fractionated electrograms, late potentials, and broad duration electrograms predominantly in the RVOT epicardium.
- Endpoint: Elimination of abnormal electrograms, normalisation of the Type 1 ECG pattern, and non-inducibility of VT/VF at post-ablation PES.
- Australian availability: Performed at major specialised EP centres (e.g., Alfred Hospital Melbourne, RPAH Sydney, Royal Adelaide Hospital, Prince Charles Hospital Brisbane). Referral to a high-volume BrS ablation centre is recommended.
Indications for catheter ablation:
- VF storm or recurrent appropriate ICD shocks despite quinidine therapy
- Quinidine intolerance or contraindication with recurrent VT/VF
- Consideration as first-line therapy in high-volume centres with demonstrated expertise
4. General Measures and Trigger Avoidance
- Fever management: Aggressive antipyretic therapy (paracetamol + ibuprofen) for any febrile illness. Fever is the most common trigger for arrhythmic events. Consider home temperature monitoring.
- Drug avoidance: Refer to the international Brugada Drugs Registry (www.brugadadrugs.org) before any new medication. Key avoidances include class I antiarrhythmics (except quinidine), tricyclic antidepressants, lithium, cocaine, excessive alcohol.
- Avoidance of excessive alcohol consumption and recreational drugs.
- Avoidance of electrolyte disturbances: Prompt correction of hypokalaemia and hypomagnesaemia.
- Pre-operative counselling: Alert anaesthetic team before any surgical procedure; avoid propofol, bupivacaine, and other BrS-contraindicated anaesthetic agents.
5. Other Pharmacological Considerations
| Agent | Mechanism | Role in BrS | Notes |
|---|---|---|---|
| Isoproterenol (isoprenaline) | β-agonist → ↑ ICa,L | Acute VF storm / recurrent VT in ED or ICU | IV infusion 0.003–0.03 µg/kg/min. TGA Special Access. |
| Cilostazol | PDE-3 inhibitor → ↑ ICa,L, ↑ HR | Case reports of ECG normalisation | Off-label; limited evidence; not PBS for BrS |
| Amiodarone | Multi-channel blocker | Limited efficacy; may be used for AF | Not first-line for VF prevention in BrS |
Monitoring
- Cardiology follow-up: Annual review with an electrophysiologist or specialised inherited arrhythmia clinic. More frequent review if symptomatic, post-ICD implantation, or on quinidine therapy.
- ECG surveillance: Serial 12-lead ECGs at each clinic visit. Repeat ECG during any febrile illness. High V1–V3 recording recommended.
- ICD management: Device clinic review every 3–6 months. Interrogation for appropriate/inappropriate shocks, arrhythmia burden, and battery status. Consider remote monitoring.
- Quinidine therapy monitoring: Serum quinidine levels (target 2–5 µg/mL), renal function, LFTs, FBC at baseline and every 6–12 months. ECG for QTc monitoring.
- Family screening: First-degree relatives should have baseline and serial ECGs. Genetic testing of the index case facilitates targeted cascade testing in relatives. Repeat ECG screening of genotype-negative relatives during adolescence and early adulthood.
- Psychological support: Diagnosis of an inheritable SCD syndrome has significant psychosocial impact. Screen for anxiety and depression; referral to psychology/counselling services as needed. Driver's licence implications (Australasian Fitness to Drive guidelines — private licence generally unrestricted if ICD implanted and asymptomatic; commercial licence restrictions apply).
Special Populations
Aboriginal and Torres Strait Islander Health Considerations
📚 References
- 1. Brugada P, Brugada J. Right bundle branch block, persistent ST segment elevation and sudden cardiac death: a distinct clinical and electrocardiographic syndrome. J Am Coll Cardiol. 1992;20(6):1391–1396.
- 2. Antzelevitch C, Yan GX, Ackerman MJ, et al. J-Wave syndromes expert consensus conference report: emerging concepts and gaps in knowledge. Heart Rhythm. 2016;13(10):e295–e324.
- 3. Priori SG, Wilde AA, Horie M, et al. HRS/EHRA/APHRS expert consensus statement on the diagnosis and management of patients with inherited primary arrhythmia syndromes. Heart Rhythm. 2013;10(12):1932–1963.
- 4. Wilde AAM, Semsarian C, Márquez MF, et al. European Heart Rhythm Association (EHRA)/Heart Rhythm Society (HRS)/Asia Pacific Heart Rhythm Society (APHRS)/Latin American Heart Rhythm Society (LAHRS) expert consensus statement on the state of genetic testing for cardiac diseases. Heart Rhythm. 2023;20(9):e97–e172.
- 5. Probst V, Veltmann C, Eckardt L, et al. Long-term prognosis of patients diagnosed with Brugada syndrome: results from the FINGER Brugada Syndrome Registry. Circulation. 2010;121(5):635–643.
- 6. Brugada J, Pappone C, Berruezo A, et al. Brugada syndrome phenotype elimination by epicardial substrate ablation. Circ Arrhythm Electrophysiol. 2015;8(6):1373–1381.
- 7. Viskin S, Wilde AAM, Tan HL, et al. Empiric quinidine therapy for asymptomatic Brugada syndrome: time for a prospective registry. Heart Rhythm. 2009;6(3):401–404.
- 8. Casado-Arroyo R, Berne P, Rao JY, et al. Long-term trends in newly diagnosed Brugada syndrome: implications for risk stratification. J Am Coll Cardiol. 2016;68(6):614–623.
- 9. Postema PG, Wolpert C, Amin AS, et al. Drugs and Brugada syndrome patients: review of the literature, recommendations, and an up-to-date website (www.brugadadrugs.org). Heart Rhythm. 2009;6(9):1335–1341.
- 10. Australian Institute of Health and Welfare (AIHW). Sudden cardiac death in young Australians. AIHW Bulletin. 2020. Cat. no. AUS 233.
- 11. Brugada R, Campuzano O, Sarquella-Brugada G, et al. Brugada syndrome. In: Adam MP, Feldman J, Mirzaa GM, et al., editors. GeneReviews®. University of Washington, Seattle; 2005 (updated 2023).
- 12. Australasian College of Sport and Exercise Physicians / Austroads. Austroads Fitness to Drive Guidelines. Sydney: Austroads; 2022 (updated online). Available from: www.austroads.com.au.