📋 Key Information Summary
- Tricuspid regurgitation (TR) is the most common valvular lesion and is frequently functional (secondary to annular dilatation and right ventricular remodelling) rather than due to primary leaflet pathology.
- Functional TR is driven by left-sided heart disease (particularly mitral regurgitation), pulmonary hypertension, and atrial fibrillation — addressing the underlying cause is the first-line strategy.
- Pacemaker and ICD lead-related TR affects up to 10–20% of patients with trans-tricuspid leads and should be suspected when TR worsens after device implantation.
- Severity assessment uses a multi-parametric echocardiographic approach: vena contracta width (≥7 mm severe), effective regurgitant orifice area (EROA ≥40 mm²), hepatic vein flow reversal, and RV size/function.
- Severe TR is an independent predictor of mortality regardless of left ventricular function — early recognition and appropriate referral are essential.
- Surgical referral is indicated for severe primary TR, severe TR at the time of left-sided valve surgery, and isolated severe TR with symptoms or progressive RV dilatation/dysfunction.
- Transcatheter tricuspid valve interventions (edge-to-edge repair with TriClip™, annuloplasty with Cardioband™, and emerging valve replacements) offer options for patients deemed high surgical risk — refer to structural heart disease centres.
- Medical management centres on loop diuretics for congestion relief, treatment of atrial fibrillation, and optimisation of left-sided valvular or myocardial disease.
- Diuretic doses in right heart failure are often higher than in left heart failure; combination with metolazone may be required for diuretic resistance.
- Aboriginal and Torres Strait Islander Australians have higher rates of rheumatic heart disease and rheumatic TR, requiring culturally safe screening, outreach echocardiography, and long-term benzathine penicillin prophylaxis.
Introduction & Australian Epidemiology
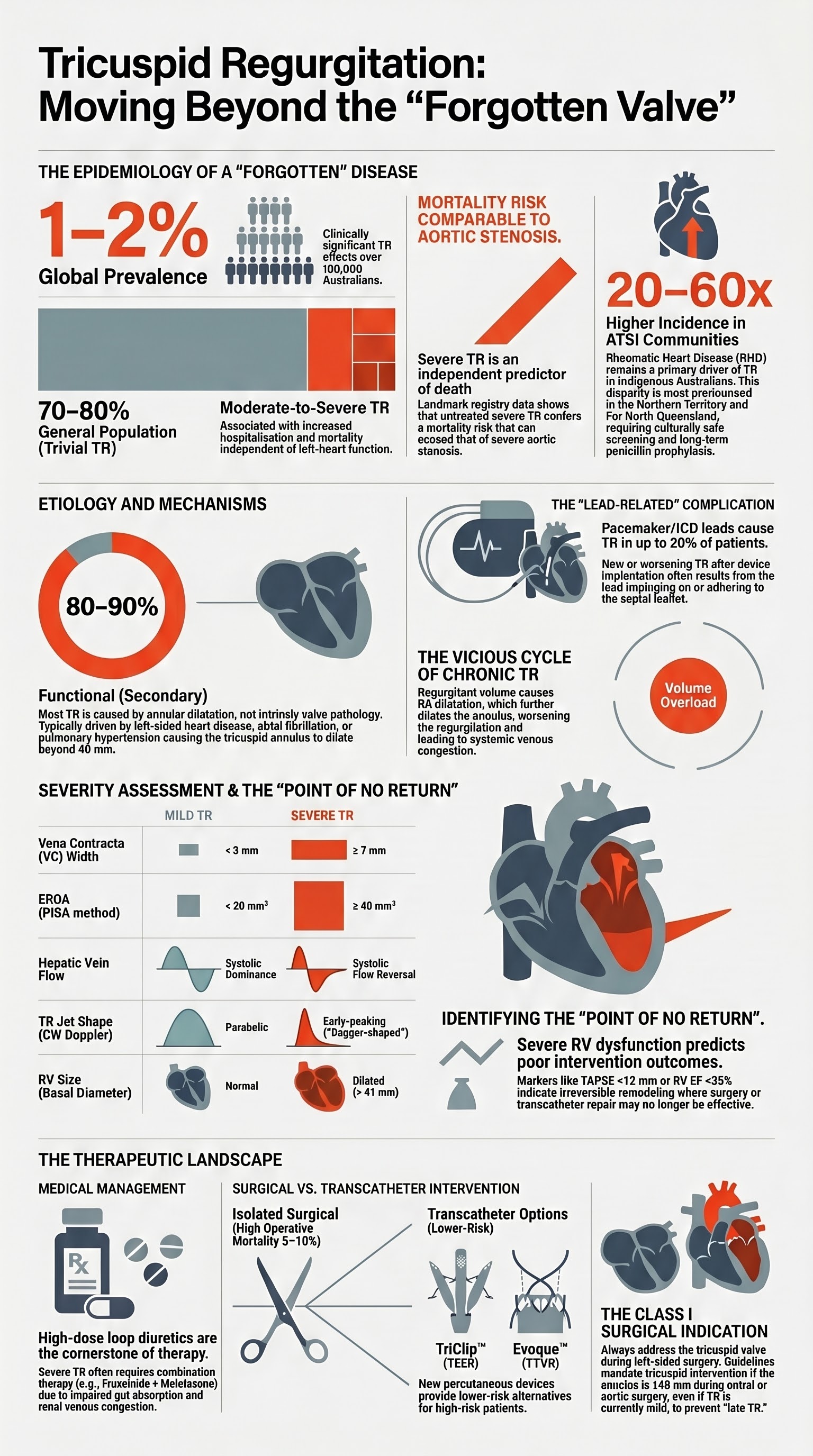
Tricuspid regurgitation (TR) refers to the retrograde flow of blood from the right ventricle (RV) into the right atrium (RA) during systole. TR is the most frequently encountered valvular abnormality on echocardiography, with trivial to mild TR detected in up to 70–80% of the general population. Clinically significant (moderate-to-severe) TR is present in approximately 1–2% of the population and is associated with increased mortality, heart failure hospitalisation, and reduced functional capacity independent of left ventricular function.
Historically considered a benign and largely ignored finding — often termed the "forgotten valve" — TR has undergone a renaissance in cardiovascular medicine over the past decade. Landmark registry data, including studies from the Society of Thoracic Surgeons (STS) database and European registries, have demonstrated that severe TR confers a mortality risk comparable to or exceeding that of severe aortic stenosis when left untreated.
In Australia, the AIHW reports that valvular heart disease accounts for approximately 12,000 hospital admissions annually. While specific Australian TR prevalence data are limited, international extrapolation and the ageing Australian population suggest that significant TR affects over 100,000 Australians. Importantly, rheumatic heart disease (RHD) remains a significant cause of TR in Aboriginal and Torres Strait Islander communities, with incidence rates 20–60 times higher than in non-Indigenous Australians in the Northern Territory and Far North Queensland.
Access to specialist structural heart disease services varies across Australia. While major tertiary centres in Sydney, Melbourne, Brisbane, Perth, Adelaide, and Hobart offer transcatheter tricuspid interventions through clinical trials and compassionate-use programmes, patients in regional and remote areas face significant barriers to accessing advanced imaging and intervention.
Etiology & Mechanisms
Understanding the aetiology of TR is critical because management strategy differs fundamentally between primary (organic) and secondary (functional) disease. Approximately 80–90% of clinically significant TR is functional in nature.
Functional (Secondary) TR — Most Common
Functional TR results from distortion of the normal tricuspid valve apparatus without intrinsic leaflet pathology. The two primary mechanisms are:
- Annular dilatation: The tricuspid annulus is a complex, non-planar, saddle-shaped structure. Right atrial and RV remodelling leads to annular dilatation (predominantly in the anteroposterior and septolateral dimensions), preventing leaflet coaptation. Annular diameter >40 mm (or >21 mm/m²) is associated with significant functional TR.
- Leaflet tethering (tenting): RV dilatation and dysfunction displace the papillary muscles apically and laterally, causing restricted leaflet motion and increased tenting height (>8 mm) and tenting area (>1.6 cm²).
Common causes of functional TR include:
- Left-sided valvular disease (especially mitral regurgitation and mitral stenosis)
- Left ventricular systolic or diastolic dysfunction with secondary pulmonary hypertension
- Atrial fibrillation — causes isolated RA dilatation and annular dilatation without RV dysfunction; increasingly recognised as a major standalone cause
- Pulmonary arterial hypertension (Group 1–5)
- Right ventricular cardiomyopathy (ARVC) and congenital heart disease (Ebstein anomaly, post-Fallot repair)
Primary (Organic) TR
Primary TR involves intrinsic abnormality of the valve leaflets, chordae, or papillary muscles:
| Cause | Mechanism | Australian Context |
|---|---|---|
| Rheumatic heart disease | Commissural fusion, leaflet thickening, chordal shortening; often combined with mitral disease | Endemic in Indigenous communities — see ATSI section |
| Infective endocarditis | Leaflet destruction, vegetations, perforation; predominantly in IVDU and CIED patients | Rising incidence with CIED implantation |
| Ebstein anomaly | Apical displacement of septal and posterior leaflets; atrialised RV | Managed at paediatric/adult congenital heart centres |
| Carcinoid syndrome | Endocardial plaque deposits on valve leaflets causing retraction and rigidity | Rare; managed via neuroendocrine tumour MDTs |
| Traumatic (chest wall injury) | Papillary muscle rupture or chordal tear post-blunt trauma | Consider in MVA presentations with new murmur |
| Myxomatous degeneration | Leaflet prolapse, redundant chordae — often associated with mitral valve prolapse | Common incidental finding |
| Drug-induced (ergot, pergolide, fenfluramine) | Serotonergic valve fibrosis and retraction | Historical; rarely encountered currently |
Pacemaker/ICD Lead-Related TR
Trans-tricuspid leads (pacemaker or ICD) represent an increasingly important and under-recognised cause of TR. Mechanisms include:
- Direct leaflet impingement — the lead interferes with leaflet coaptation, most commonly the septal leaflet
- Lead-induced fibrosis and adhesion of leaflet to lead
- Scarring and retraction of the valve apparatus over time
- Annular distortion from the mechanical presence of the lead
Post-Surgical TR
TR may develop or worsen months to years after left-sided cardiac surgery, particularly mitral valve surgery. This "late TR" occurs in 10–30% of patients and is thought to result from progressive RV remodelling, atrial fibrillation, and failure to address the tricuspid annulus at the time of initial surgery. Current guidelines support concomitant tricuspid annuloplasty when the tricuspid annulus is dilated (≥40 mm or ≥21 mm/m²) at the time of left-sided surgery, even in the absence of significant TR — a strategy that reduces late TR development.
Pathophysiology of Chronic Severe TR
Chronic severe TR initiates a self-perpetuating cycle:
- Regurgitant volume → RA volume overload → RA dilatation → annular dilatation → worsening TR
- Elevated RA pressure → systemic venous congestion → hepatic congestion → cardiac cirrhosis
- RV volume and pressure overload → RV dilatation → septal bowing into LV → reduced LV filling and cardiac output
- Reduced forward cardiac output → neurohormonal activation → further fluid retention → worsening congestion
Severity Assessment
Accurate grading of TR severity is essential for clinical decision-making. Unlike aortic and mitral regurgitation, quantitative assessment of TR has historically been more challenging due to the complex three-dimensional geometry of the tricuspid annulus and the relative paour of validated volumetric methods. Current echocardiographic guidelines recommend a multi-parametric, integrative approach.
Qualitative and Semi-Quantitative Methods
| Parameter | Mild | Moderate | Severe |
|---|---|---|---|
| Colour jet area (RA) | <5 cm² | 5–10 cm² | >10 cm² (use with caution — loading-dependent) |
| Vena contracta (VC) width | <3 mm | 3–6.9 mm | ≥7 mm |
| PISA radius (at Nyquist 28 cm/s) | <5 mm | 5–9 mm | ≥9 mm |
| Hepatic vein flow | Systolic dominance (S > D) | Systolic blunting (S < D) | Systolic flow reversal |
| TR jet density (CW Doppler) | Faint, incomplete envelope | Dense but incomplete | Dense, triangular, early peaking |
| TR jet contour (CW) | Parabolic | Parabolic to early peaking | Early-peaking, "dagger-shaped" |
| Inferior vena cava diameter | Usually normal | May be dilated | Dilated (>21 mm), reduced collapse (<50%) |
| RA/RV size | Normal | May be dilated | Dilated (RA volume >33 mL/m², RV basal >41 mm) |
Quantitative Methods
- Effective regurgitant orifice area (EROA): Calculated using the PISA (proximal isovelocity surface area) method. EROA ≥40 mm² indicates severe TR (or ≥20 mm² in the 2021 ESC/EACTS guidelines for severe classification). The 2020 ACC/AHA guidelines use EROA ≥40 mm² as the severe threshold.
- Regurgitant volume (RVol): ≥45 mL/beat indicates severe TR. Can be calculated by the PISA method or by volumetric (3D echo or CMR) approach: RVol = (RVOT area × RVOT VTI) – (mitral annular area × mitral VTI), though this method carries considerable measurement error.
- 3D echocardiography: Emerging as the preferred method for TR quantification. Direct planimetry of the vena contracta area on 3D colour Doppler provides improved accuracy over 2D methods. 3D vena contracta area ≥0.75 cm² has been proposed for severe TR.
Cardiac MRI for TR Quantification
Cardiac magnetic resonance (CMR) is the gold standard for RV volumetric assessment and can quantify TR by comparing RV stroke volume (by cine volumetry) with forward flow (by phase-contrast flow in the pulmonary artery). A regurgitant fraction ≥35% is consistent with severe TR. CMR is particularly valuable when echo quality is suboptimal or when accurate RV volumes are needed for surgical decision-making. CMR is available at major tertiary centres across Australian capital cities (MBS item 63018).
Integrative Grading Approach
Right Ventricular Function Assessment
RV function is a critical determinant of outcomes in TR and a key factor in surgical and transcatheter decision-making:
- TAPSE (tricuspid annular plane systolic excursion): <17 mm suggests RV systolic dysfunction
- RV S' (tissue Doppler): <9.5 cm/s suggests reduced RV longitudinal function
- Fractional area change (FAC): <35% indicates RV systolic dysfunction
- RV free wall global longitudinal strain (GLS): >–20% (absolute value <20%) suggests impaired RV mechanics; increasingly used in research and emerging clinical practice
- RV end-systolic volume index (RVEDSI) on CMR: Important for surgical timing — severe RV dilatation with preserved EF may be a window for intervention before irreversible dysfunction
Clinical Presentation & Diagnostic Criteria
Symptoms
Mild and moderate TR are frequently asymptomatic. Symptoms develop insidiously with severe TR and are related to systemic venous congestion and reduced cardiac output:
- Exertional dyspnoea — often attributed to left-sided disease or deconditioning
- Fatigue and exercise intolerance — due to reduced forward cardiac output
- Peripheral oedema — ankle swelling, ascites, anasarca in advanced disease
- Right upper quadrant discomfort — hepatic congestion and capsular stretch
- Pulsations in the neck — prominent "c-v" waves of the jugular venous pulse
- Early satiety and nausea — gut congestion from systemic venous hypertension
- Weight gain and fluid retention
Physical Examination
- Jugular venous pressure (JVP): Elevated with prominent systolic "c-v" waves (Lancisi sign) — pathognomonic of severe TR. The JVP waveform shows loss of the normal x-descent and a prominent systolic wave that may be visible as ear-lobe pulsation.
- Auscultation: Pansystolic murmur at the left lower sternal border that increases with inspiration (Carvallo sign). The murmur may be soft and difficult to hear despite severe TR due to low RV-RA pressure gradient. A right-sided S3 gallop indicates RV volume overload.
- Hepatomegaly: Tender, pulsatile liver (systolic pulsation transmitted through the hepatic veins). Chronic congestion leads to cardiac cirrhosis.
- Peripheral oedema: Dependent oedema (ankles in ambulatory patients, sacral in bedbound patients).
- Ascites: May be prominent in severe, chronic TR — refractory to diuretics in advanced cases.
- Pleural effusions: Typically bilateral or right-sided; transudative.
Key Diagnostic Criteria
Diagnosis of significant TR relies on:
- Clinical features of right heart failure (elevated JVP, hepatomegaly, oedema)
- Transthoracic echocardiography confirming moderate-to-severe TR with multi-parametric grading
- Identification of aetiology (functional vs primary) and underlying cause
- Assessment of RV size and function (TAPSE, FAC, GLS, RV volumes)
- Estimation of pulmonary pressures to assess for secondary pulmonary hypertension
Investigations
Essential First-Line Investigations
Advanced / Specialist Investigations
Surgical Indications
Surgical treatment of TR remains the established intervention for severe disease, though it carries significant perioperative risk. The optimal timing of surgery is critical — intervention before irreversible RV dysfunction offers the best outcomes.
Indications for Tricuspid Valve Surgery
Surgical Techniques
| Procedure | Indication | Key Points |
|---|---|---|
| Ring annuloplasty (rigid or flexible ring) | Functional TR with annular dilatation | First-line surgical approach for functional TR; reduces annular dimensions and improves leaflet coaptation. Pericardial bands may be used if ring unavailable. |
| De Vega annuloplasty (suture) | Functional TR — when ring not available | Suture-based plication of the annulus; higher recurrence rate than ring annuloplasty. |
| Tricuspid valve repair (Kay, commissuroplasty) | Specific leaflet pathology, localised prolapse | Leaflet and subvalvular repair techniques; preserve native valve when possible. |
| Tricuspid valve replacement (bioprosthetic) | Severe primary TR not amenable to repair; rheumatic valve disease; failed prior repair | Bioprosthesis preferred over mechanical valve (lower thrombotic risk in low-pressure RV position). 10-year freedom from reoperation ~80%. |
| Tricuspid valve replacement (mechanical) | Young patients when long-term anticoagulation acceptable | High thrombosis risk in low-flow RV position; rarely used in current practice. If used, requires lifelong warfarin with target INR 2.5–3.5. |
| Lead extraction ± valve intervention | Lead-related severe TR | Transvenous lead extraction by experienced operator, with or without concomitant TV surgery. Epicardial or leadless pacing subsequently. |
Surgical Outcomes and Risk
Concomitant TV surgery at the time of left-sided valve repair/replacement carries an additional 30-minute cross-clamp time and modestly increases perioperative morbidity, but the long-term benefit of preventing late TR progression generally justifies the strategy.
Australian Surgical Centres
Tricuspid valve surgery is performed at all major cardiothoracic surgical centres across Australia, including Royal Prince Alfred and Westmead (Sydney), Monash and Alfred (Melbourne), Royal Brisbane, Fiona Stanley and Royal Perth (Perth), Royal Adelaide, and Royal Hobart. Isolated TV surgery and re-operative TV surgery should be referred to high-volume centres with expertise in complex valve surgery.
Transcatheter Therapies
Transcatheter tricuspid valve intervention (TTVI) represents one of the most rapidly evolving areas in structural heart disease. Given the high surgical mortality for isolated tricuspid valve surgery, multiple percutaneous technologies have been developed to address TR in patients deemed prohibitive or high surgical risk.
Edge-to-Edge Repair (Leaflet Approximation)
TriClip™ / TriClip G4™ (Abbott) — the most extensively studied transcatheter TR therapy. Based on the MitraClip™ platform adapted for the tricuspid valve.
Direct Annuloplasty
Cardioband™ (Edwards Lifesciences) — transcatheter tricuspid annuloplasty system delivered via transfemoral approach.
- Mechanism: Percutaneous implantation of an adjustable annuloplasty band on the tricuspid annulus under fluoroscopic and TOE guidance. Anchors are placed in the annular tissue from the anteroseptal to the posteros commissure, and cinching reduces annular diameter to improve leaflet coaptation.
- Key trial: TRI-REPAIR (2017) and ongoing studies demonstrated feasibility with significant annular reduction and TR grade improvement.
- Advantages: Addresses the primary mechanism of functional TR (annular dilatation); can be combined with edge-to-edge repair.
- Challenges: Technically demanding with a steep learning curve; requires meticulous imaging guidance; risk of anchor dislodgement and coronary sinus injury.
- Australian availability: Limited; available at select structural heart disease centres as part of clinical research programmes.
Caval Valve Implantation (CAVI)
SAPIEN valve in the inferior vena cava (TricValve®, Edwards; SAPIEN 3 off-label) — a novel concept that does not treat the tricuspid valve itself but places a bioprosthetic valve in the inferior vena cava (and optionally superior vena cava) to prevent retrograde flow into the systemic venous system during systole.
- Concept: "Bailout" strategy that treats the haemodynamic consequences of severe TR rather than the valve itself. Reduces hepatic congestion and improves forward cardiac output without touching the tricuspid valve.
- Key trial: TRICAVAL (2020) demonstrated feasibility and early safety; TRICUS PERCEVAL and other trials ongoing.
- Ideal patient: Severe symptomatic TR with significant IVC dilatation, poor RV function, and prohibitive surgical risk — particularly those with prior failed interventions.
- Australian availability: Very limited; compassionate use at select centres.
Transcatheter Tricuspid Valve Replacement (TTVR)
Several dedicated transcatheter tricuspid valve replacement systems are in clinical development:
| Device | Manufacturer | Status | Key Features |
|---|---|---|---|
| Evoque™ | Edwards Lifesciences | FDA approved (Feb 2024); CE-marked; pivotal trial (TRISCEND II) positive | Self-expanding nitinol frame with bovine pericardial tissue valve; native leaflet capture anchoring; transfemoral delivery |
| Intrepid™ | Medtronic | Early feasibility studies (EXPAND TEER TTVR) | Self-expanding frame; dual stent design for annular and supra-annular positioning |
| LuX-Valve™ | Jenscare Biotechnology | Early clinical experience; right atrial anchoring system | Transatrial (transjugular) access; designed for patients with large annuli |
Patient Selection for Transcatheter Interventions
Australian Access to Transcatheter Tricuspid Interventions
Transcatheter tricuspid valve interventions are currently available at a limited number of structural heart disease centres in Australia, primarily through clinical trials, compassionate-use programmes, and emerging commercial availability of TriClip™. Centres with active transcatheter tricuspid programmes include (but are not limited to):
- Royal Prince Alfred Hospital, Sydney
- Monash Health, Melbourne
- The Alfred Hospital, Melbourne
- St Vincent's Hospital, Sydney
- Royal Brisbane and Women's Hospital
- Fiona Stanley Hospital, Perth
Patients in regional and remote areas require transfer to these centres. Telehealth consultation with the structural heart disease team can facilitate initial assessment. The TGA has approved TriClip™ in 2024, and PBS listing for device reimbursement remains under assessment.
Medical Management
Medical therapy for TR focuses on symptom management (congestion relief), treatment of underlying causes, and optimisation of associated conditions. Medical therapy alone does not alter the natural history of severe TR but plays a critical role in stabilising patients for potential intervention and managing those who are not candidates for valve intervention.
Diuretic Therapy — Cornerstone of Medical Management
Optimisation of Left-Sided Disease
For functional TR secondary to left-sided heart disease, treating the underlying cause is paramount:
- Mitral regurgitation: Mitral valve repair/replacement (surgical or transcatheter with MitraClip™) is the most effective intervention for MR-related functional TR. Significant TR often improves or resolves after successful mitral intervention.
- Mitral stenosis: Percutaneous mitral balloon valvotomy or surgical MVR/repair addresses the primary cause of pulmonary hypertension driving functional TR.
- Heart failure with reduced ejection fraction (HFrEF): Optimise guideline-directed medical therapy (ACEi/ARB/ARNI, beta-blocker, MRA, SGLT2 inhibitor). Sacubitril-valsartan (Entresto®) may improve secondary TR by reducing left-sided filling pressures and pulmonary hypertension.
- Heart failure with preserved EF (HFpEF): Sodium-glucose cotransporter-2 (SGLT2) inhibitors (dapagliflozin 10 mg PO daily or empagliflozin 10 mg PO daily — both PBS-listed for heart failure) have shown benefit in HFpEF and may reduce pulmonary congestion contributing to functional TR.
Management of Associated Conditions
Pulmonary Hypertension Management
When TR is secondary to pulmonary hypertension (PH), treating the underlying PH is essential:
- Group 2 PH (left heart disease): Treat the underlying cardiac condition; PAH-specific therapy is generally NOT recommended (may worsen pulmonary oedema).
- Group 3 PH (lung disease): Optimise COPD/ILD management; long-term oxygen therapy if hypoxic.
- Group 1 PAH: Refer to a pulmonary hypertension centre. Bosentan, sildenafil, ambrisentan, macitentan, riociguat, and treprostinil are PBS-listed under authority for PAH with various restrictions.
Medical Therapy Limitations
Monitoring
Surveillance Schedule
Key Monitoring Parameters
- TR severity grade (multi-parametric) — watch for progression
- RV size (RV basal diameter, RV end-diastolic area) and function (TAPSE, FAC, RV GLS)
- RA size and IVC diameter with respiratory variation
- Estimated pulmonary artery systolic pressure (PASP)
- Symptoms: NYHA class, 6-minute walk distance, quality of life (Kansas City Cardiomyopathy Questionnaire)
- Renal function (eGFR, creatinine) — renal congestion is a key driver of cardiorenal syndrome in severe TR
- Liver function tests — hepatic congestion pattern
- NT-proBNP / BNP — prognostic and guides therapy
- Body weight — daily monitoring for fluid management
- Electrolytes — potassium, magnesium, sodium (diuretic-related)
Red Flags Requiring Urgent Reassessment
- New or worsening symptoms of right heart failure despite optimised diuretic therapy
- Progressive RV dilatation or declining TAPSE/FAC on serial echocardiography
- Worsening renal function despite adequate decongestion (cardiorenal syndrome)
- New atrial fibrillation or loss of sinus rhythm
- New or worsening hepatic congestion with rising bilirubin or coagulopathy
- Recurrent hospital admissions for fluid overload
Special Populations
Pregnancy
Paediatrics
Elderly (≥75 years)
Renal Impairment
Hepatic Impairment
Immunocompromised
Aboriginal and Torres Strait Islander Health
📚 References
- 1. Vahanian A, Beyersdorf F, Praz F, et al. 2021 ESC/EACTS Guidelines for the management of valvular heart disease. Eur Heart J. 2022;43(7):561–632.
- 2. Otto CM, Nishimura RA, Bonow RO, et al. 2020 ACC/AHA Guideline for the management of patients with valvular heart disease. Circulation. 2021;143(5):e72–e227.
- 3. Hahn RT, Kodali S, Fam N, et al. Early multinational experience of transcatheter tricuspid valve replacement for severe tricuspid regurgitation: the TRISCEND study. JACC Cardiovasc Interv. 2022;15(24):2499–2511.
- 4. Lurz P, Stephan von Bardeleben R, Weber M, et al. Transcatheter edge-to-edge repair for treatment of tricuspid regurgitation (TRILUMINATE). N Engl J Med. 2023;388(12):1089–1098.
- 5. Dandel M, Hetzer R. Severe tricuspid regurgitation: current understanding of mechanisms, natural history, and the forgotten valve. Eur Heart J. 2022;43(18):1700–1712.
- 6. Taramasso M, Gavazzoni M, Maisano F, et al. Tricuspid regurgitation: what is the real clinical impact? JACC Cardiovasc Imaging. 2023;16(1):115–128.
- 7. Australian Institute of Health and Welfare. Rheumatic heart disease and acute rheumatic fever in Australia: 2017–2021. AIHW; 2023.
- 8. RHDAustralia (ARF/RHD writing group). Australian guideline for prevention, diagnosis and management of acute rheumatic fever and rheumatic heart disease (3rd edition). Menzies School of Health Research; 2020.
- 9. Utsunomiya H, Itabashi Y, Mihara H, et al. Functional tricuspid regurgitation: current understanding and treatment strategies. J Cardiol. 2022;79(5):580–587.
- 10. Praz F, Muraru D, Kreidel F, et al. Transcatheter treatment for tricuspid valve disease. Eur Heart J. 2021;42(38):3909–3923.
- 11. Asch FM, Toolan K, Weissman NJ, et al. Comprehensive echocardiographic assessment of the tricuspid valve: a consensus statement from the American Society of Echocardiography. J Am Soc Echocardiogr. 2024;37(2):135–172.
- 12. Dworakowski R, Bhamra-Ariza P, Gallivan S, et al. Caval valve implantation for severe tricuspid regurgitation: systematic review and meta-analysis. JACC Cardiovasc Interv. 2023;16(4):393–404.
- 13. National Heart Foundation of Australia and Cardiac Society of Australia and New Zealand. Australian clinical guidelines for heart failure 2024. Heart Lung Circ. 2024;33(1):1–120.
- 14. Monteagudo Ruiz JM, Doltra A, Sitges M, et al. Pacemaker-lead-related tricuspid regurgitation: a review. JACC Clin Electrophysiol. 2023;9(6):836–849.