📋 Key Information Summary
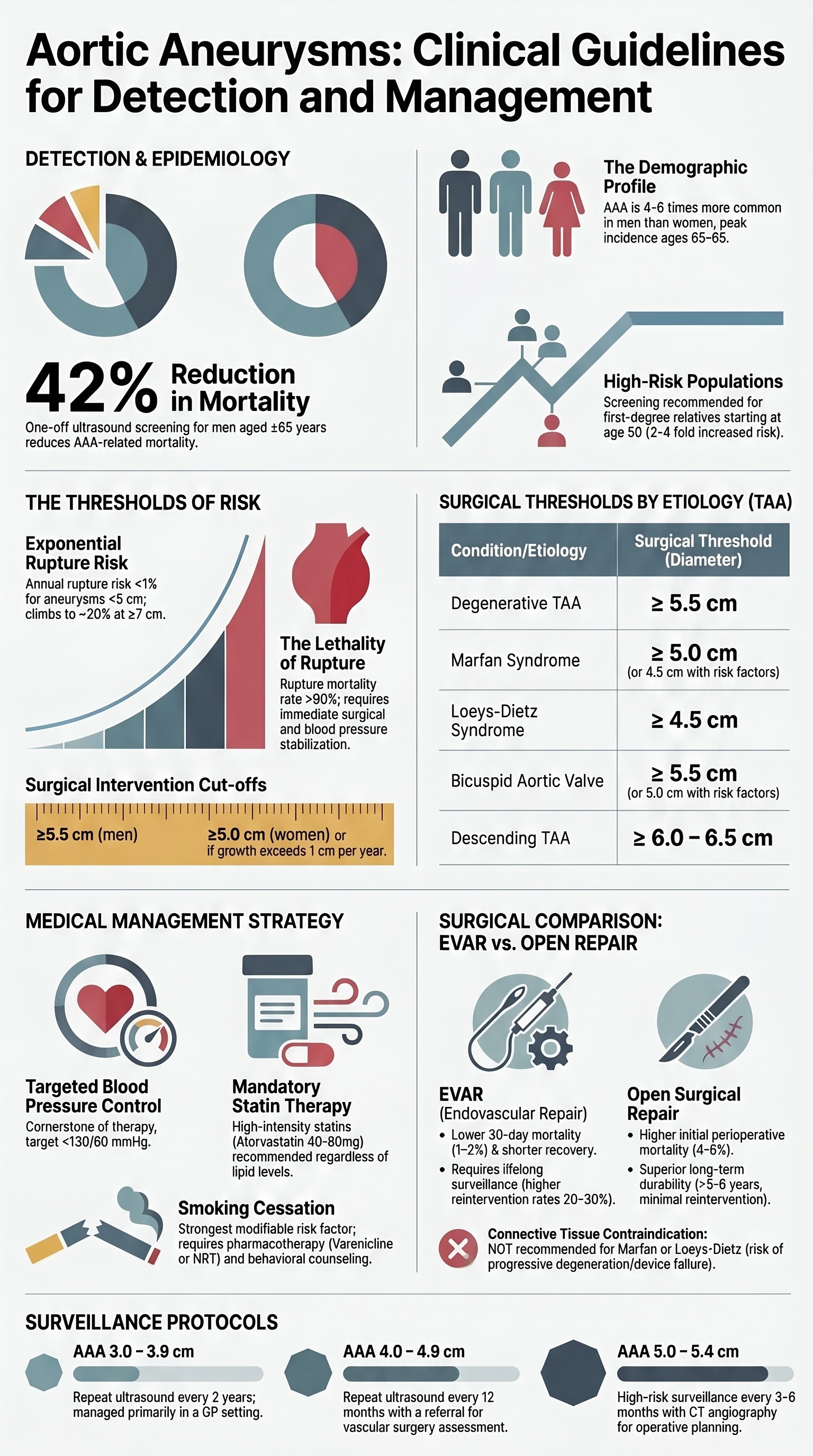
- AAA screening: Ultrasound screening is recommended for all men aged ≥65 years. One-off screening reduces AAA-related mortality by approximately 42%. No routine screening recommended for women in the general population.
- Size thresholds for intervention: Abdominal aortic aneurysm — elective repair recommended when diameter ≥5.5 cm (men) or ≥5.0 cm (women), or rapid growth >1 cm/year. Thoracic aortic aneurysm — surgical threshold generally ≥5.5 cm for degenerative, ≥5.0 cm for Marfan/Loeys-Dietz, and ≥4.5 cm with bicuspid aortic valve plus additional risk factors.
- Rupture risk rises exponentially with diameter: <1% per year at <5 cm, ~5% at 5–5.9 cm, ~10% at 6–6.9 cm, and ~20% at ≥7 cm. Rupture carries an overall mortality exceeding 80%.
- EVAR vs open repair: Endovascular aneurysm repair (EVAR) offers lower 30-day mortality but requires lifelong surveillance imaging and higher reintervention rates. Open repair has superior long-term durability. Shared decision-making is essential.
- Genetic aortopathies (Marfan syndrome, Loeys-Dietz syndrome, vascular Ehlers-Danlos syndrome) require early specialist referral, family cascade screening, serial imaging, and tailored pharmacotherapy.
- Blood pressure control is the cornerstone of medical management. Target <130/80 mmHg. Beta-blockers are first-line in Marfan syndrome to slow aortic root dilation.
- Smoking cessation is the single most modifiable risk factor for AAA growth and rupture. Offer nicotine replacement therapy, varenicline, or bupropion alongside behavioural support.
- Statin therapy (atorvastatin or rosuvastatin) is recommended for all patients with aortic aneurysm irrespective of lipid levels to reduce cardiovascular events.
- Surveillance intervals: AAA 3.0–3.9 cm — repeat ultrasound every 2 years; 4.0–4.9 cm — every 12 months; 5.0–5.4 cm — every 3–6 months. TAA — CT or MRI at 6- to 12-monthly intervals depending on size and etiology.
- Abdominal pain, hypotension, or syncope in a patient with a known aneurysm is a vascular emergency — arrange immediate CT angiography and urgent vascular surgery consultation.
- ATSI populations have lower documented AAA prevalence but higher rupture mortality due to delayed presentation and limited access to vascular surgical services in remote and rural communities.
- First-degree relatives of patients with AAA should be offered screening ultrasound (≥2% prevalence when index case is male). Genetic referral is indicated for all patients presenting <60 years or with family history of aortic dissection.
Introduction & Australian Epidemiology
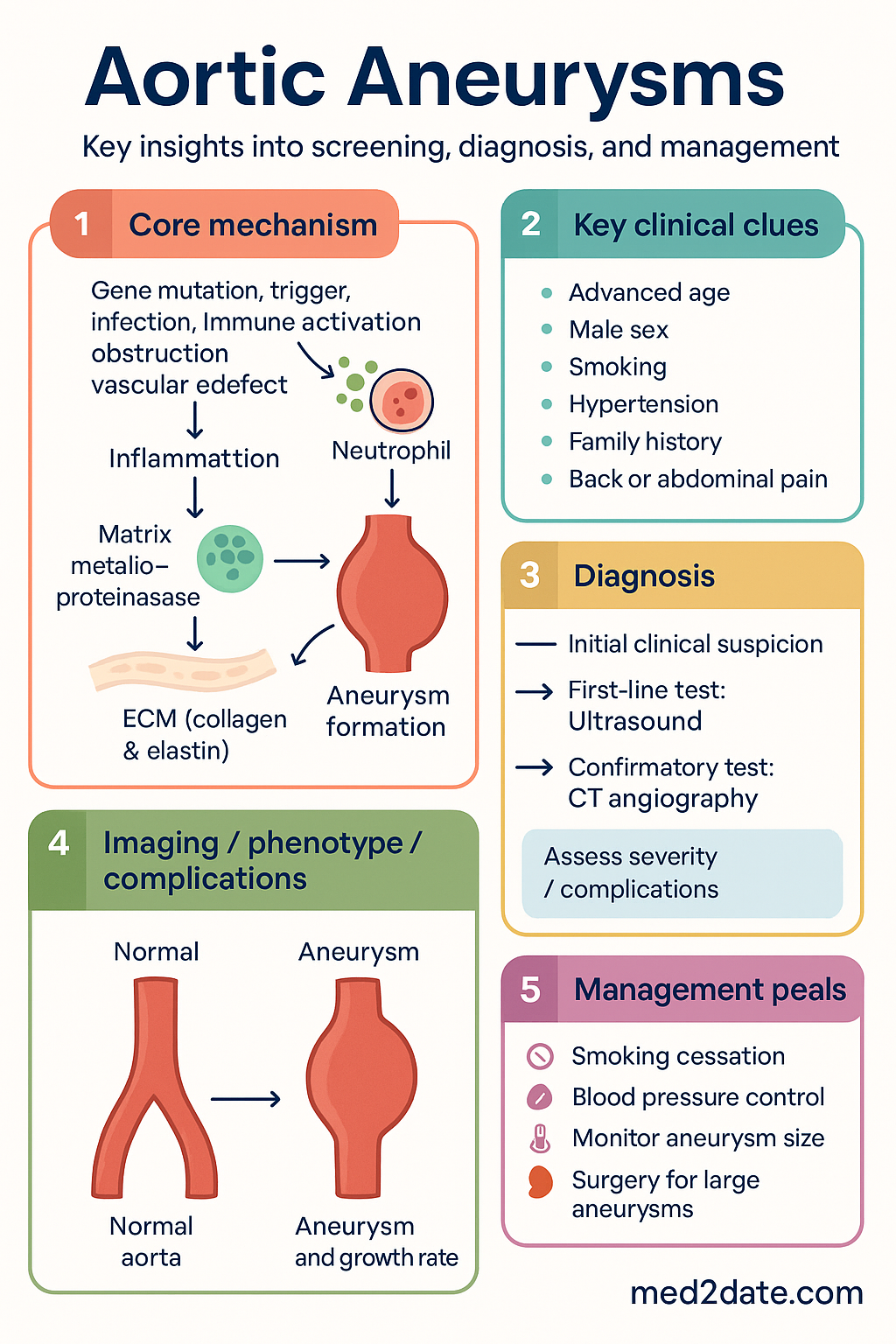
Aortic aneurysm is a localised, permanent dilation of the aorta exceeding 50% of the normal expected diameter. Aneurysms may involve the thoracic aorta (ascending, arch, or descending), the abdominal aorta (infrarenal most commonly), or both (thoraco-abdominal). The condition is often asymptomatic until catastrophic rupture or dissection occurs, earning its reputation as a "silent killer."
In Australia, aortic aneurysm and dissection accounted for approximately 2,100 deaths in 2022, representing a significant cardiovascular mortality burden (Australian Bureau of Statistics). The age-standardised mortality rate has declined over the past two decades, largely attributable to increased detection through screening programmes and improvements in elective surgical outcomes.
Key epidemiological points for the Australian context include:
- AAA is 4–6 times more common in men than women
- Peak incidence occurs in the 65–85 age group
- Smoking increases AAA risk 3–7 fold and is the strongest modifiable risk factor
- First-degree relatives of affected individuals have a 2–4 fold increased risk
- Thoracic aortic aneurysms are less common (approximately 6 per 100,000 person-years) but carry significant morbidity from dissection and rupture
- The National Vascular Disease Prevention Alliance recommends integration of AAA screening with existing cardiovascular risk assessments in primary care
Screening & Surveillance
Abdominal Aortic Aneurysm Screening
Screening for AAA with abdominal ultrasound is a cost-effective public health strategy. The primary aim is to identify aneurysms before rupture, allowing timely elective repair with significantly lower perioperative mortality (4–5% elective repair vs >40–50% emergency rupture repair).
Who to Screen
| Population | Recommendation | Evidence Level |
|---|---|---|
| All men aged ≥65 years | One-off ultrasound screening (strong recommendation) | Level I (multiple RCTs) |
| Men aged 50–65 with ≥1 risk factor (smoking, hypertension, family history, hyperlipidaemia) | Consider screening ultrasound (conditional recommendation) | Level II |
| First-degree relatives of AAA patients (any sex) | Ultrasound screening from age 50, or 10 years younger than index case age at diagnosis | Level III |
| Women aged ≥65 with cardiovascular risk factors | Consider screening (individualised) | Level III |
| Patients with known peripheral or coronary artery disease | Ultrasound if not previously imaged | Level III |
Surveillance Protocols by Aneurysm Size
Once an aneurysm is identified, the frequency of surveillance imaging depends on the aneurysm diameter, growth rate, morphology, and patient fitness for eventual intervention.
Thoracic Aortic Aneurysm Surveillance
TAA surveillance is guided by etiology, baseline size, growth rate, and presence of genetic syndromes. Imaging modalities include transthoracic echocardiography (for the ascending aorta), CT angiography, and MRI (preferred in younger patients to reduce cumulative radiation exposure).
| Aortic Size | Imaging Interval | Modality |
|---|---|---|
| <4.0 cm (degenerative) | Every 12 months, then every 2–3 years if stable | Echocardiography ± MRI |
| 4.0–4.9 cm | Every 6–12 months | CT or MRI |
| ≥5.0 cm | Every 3–6 months | CT angiography (pre-operative planning) |
| Genetic aortopathy (any size) | Every 6–12 months (lifelong) | MRI preferred |
| Bicuspid aortic valve | Baseline imaging; repeat every 3–5 years if <4.0 cm, annually if ≥4.0 cm | Echocardiography ± MRI |
Genetic Syndrome Screening
Patients with Marfan syndrome, Loeys-Dietz syndrome, vascular Ehlers-Danlos syndrome, Turner syndrome, or bicuspid aortic valve with aortopathy require lifelong aortic surveillance. Family cascade screening using genetic testing and/or imaging is mandatory. Referral to a clinical genetics service is recommended (available at major tertiary centres: Royal Melbourne Hospital, Royal Prince Alfred Sydney, Royal Brisbane and Women's Hospital).
Thoracic Aortic Aneurysm (TAA)
Thoracic aortic aneurysms involve dilation of the ascending aorta (>70% of cases), aortic arch, or descending thoracic aorta. TAA is less common than AAA but carries a high risk of acute aortic dissection and rupture. The natural history is influenced by etiology, growth rate, and associated connective tissue disorders.
Etiology
| Etiology | Proportion | Key Features |
|---|---|---|
| Degenerative / Atherosclerotic | ~60% | Most common in older adults (>65 years), associated with hypertension, smoking, hyperlipidaemia. Typically involves the ascending aorta or descending aorta. |
| Genetic / Connective Tissue | ~20% | Marfan syndrome (fibrillin-1 mutation), Loeys-Dietz syndrome (TGFBR1/2), vascular Ehlers-Dietz (COL3A1). Earlier onset, more aggressive growth. |
| Bicuspid Aortic Valve (BAV) | ~10–15% | Present in 1–2% of the population. Aortopathy independent of valve haemodynamics — mediated by extracellular matrix defects. Ascending aorta predominantly affected. |
| Inflammatory / Infectious | ~5% | Giant cell arteritis, Takayasu arteritis, tertiary syphilis (now rare), mycotic aneurysm. |
| Post-dissection | Variable | Chronic residual dissection flap with false lumen aneurysmal dilation. Requires close surveillance. |
Size Thresholds for Surgery
Surgical thresholds are guided by aneurysm diameter, etiology, rate of growth, presence of symptoms, and concomitant cardiac surgery requirements. The following thresholds apply to elective intervention:
- Degenerative TAA: ≥5.5 cm
- Marfan syndrome: ≥5.0 cm (or ≥4.5 cm with additional risk factors — family history of dissection, rapid growth >0.5 cm/year, severe aortic regurgitation, desire for pregnancy)
- Loeys-Dietz syndrome: ≥4.5 cm (earlier intervention due to higher dissection risk at smaller diameters)
- Bicuspid aortic valve: ≥5.5 cm alone; ≥4.5 cm if undergoing concomitant aortic valve replacement; ≥5.0 cm with additional risk factors (coarctation, family history, hypertension)
- Descending TAA: ≥6.0–6.5 cm (open or TEVAR)
Growth Rates
Understanding growth rates is essential for surgical timing and surveillance intervals:
- Degenerative TAA: mean growth ~0.1–0.2 cm/year; faster in the descending aorta
- Marfan syndrome: mean growth ~0.2–0.3 cm/year; may accelerate during pregnancy
- Loeys-Dietz syndrome: growth rates variable, often faster than Marfan; 0.4–0.5 cm/year reported
- Bicuspid aortic valve: growth ~0.1–0.2 cm/year, similar to degenerative
- Post-dissection: growth may be rapid in the first year; stabilises in chronic phase
- Growth >0.5 cm in 6 months or >1 cm in 12 months is an indication for intervention regardless of absolute diameter
Abdominal Aortic Aneurysm (AAA)
Abdominal aortic aneurysm is the most common form of aortic aneurysm, predominantly involving the infrarenal aorta (90–95% of cases). AAA is a disease of ageing with a strong association with atherosclerosis, smoking, and hypertension. Rupture of AAA remains a leading cause of preventable death in older Australians.
Risk Factors
| Risk Factor | Relative Risk / Odds Ratio | Comment |
|---|---|---|
| Male sex | OR 4–6 | AAA is predominantly a disease of men; women have later onset but worse outcomes |
| Age >65 years | Incidence rises steeply | Mean age at diagnosis: 70–75 years |
| Current smoking | OR 3–7 | Dose-response relationship. Accelerates growth and increases rupture risk 4-fold. |
| Family history (1st degree) | OR 2–4 | Screen siblings and offspring. Genetic predisposition (9p21 locus, DAB2IP variants). |
| Hypertension | OR 1.5–2.5 | Contributes to wall stress and aneurysm progression |
| Hyperlipidaemia | OR 1.2–1.5 | Weaker association than for coronary disease; statins still recommended |
| COPD / Emphysema | OR 1.5–2.0 | Shared smoking aetiology; elastin degradation in lung and aortic wall |
| Peripheral artery disease | OR 2–3 | Warrants ultrasound screening for AAA |
Rupture Risk by Diameter
The risk of AAA rupture increases exponentially with diameter and is also influenced by gender (women have higher rupture risk at any given size), blood pressure control, and smoking status.
EVAR vs Open Repair
The choice between endovascular aneurysm repair (EVAR) and open surgical repair depends on aneurysm anatomy, patient comorbidities, fitness for surgery, and patient preference. Both techniques are available at major Australian vascular centres.
| Feature | EVAR | Open Repair |
|---|---|---|
| Approach | Percutaneous femoral artery access; stent-graft deployment | Midline laparotomy or retroperitoneal approach; prosthetic graft interposition |
| 30-day mortality | 1–2% | 4–5% |
| Long-term survival | Similar to open at 5 years | Superior beyond 5–8 years in fit patients |
| Reintervention rate | Higher (20–30% at 5 years — endoleak, graft migration) | Lower (<5% at 5 years) |
| Surveillance requirement | Lifelong CT/ultrasound (30 days, 6 months, 12 months, then annually) | Less intensive — clinical follow-up with imaging if symptoms |
| Suitable anatomy | Adequate neck length (≥15 mm), iliac access, no severe angulation | Hostile anatomy, short neck, young patients, connective tissue disease |
| Hospital stay | 2–3 days | 7–10 days |
| Recovery | 2–4 weeks | 6–12 weeks |
Post-EVAR Surveillance Protocol (Australian Practice)
- 30 days: CT angiography (baseline post-implant)
- 6 months: Duplex ultrasound ± CT if endoleak suspected
- 12 months: CT angiography
- Annually thereafter: Duplex ultrasound (CT reserved for abnormal findings or suspected endoleak)
- Lifelong surveillance — no "discharge" from follow-up
Genetic Aortopathies
Genetic aortopathies are a group of heritable connective tissue disorders characterised by progressive aortic dilation, dissection, and rupture at younger ages and smaller aortic diameters than degenerative aneurysms. Early recognition, genetic testing, and family cascade screening are essential to reduce morbidity and mortality.
Marfan Syndrome
Marfan syndrome is an autosomal dominant disorder caused by mutations in the FBN1 gene encoding fibrillin-1, affecting approximately 1 in 5,000 individuals. Diagnosis is based on the revised Ghent criteria (2010), incorporating aortic root Z-score, ectopia lentis, systemic score, and genetic testing.
Management principles for Marfan syndrome:
- Beta-blockers (atenolol or metoprolol) are first-line to reduce aortic root dilation rate
- Losartan (ARB) may be added or used as an alternative — based on evidence showing reduced TGF-β signalling; trials (COMPARE, Aortic Marfan) show benefit when combined with beta-blockers
- Surgical threshold: aortic root ≥5.0 cm, or ≥4.5 cm with additional risk factors (family history of dissection, rapid growth, desire for pregnancy, severe AR)
- Prophylactic aortic root replacement (David procedure — valve-sparing) is preferred over Bentall (composite valve-graft) in suitable patients
- Avoid competitive sport, isometric exercise, and contact activities
- Pregnancy requires pre-conception counselling; consider prophylactic root replacement if aortic root ≥4.5 cm before conception
Loeys-Dietz Syndrome
Loeys-Dietz syndrome (LDS) is caused by mutations in TGFBR1, TGFBR2, SMAD3, TGFB2, or TGFB3. Characterised by aortic and arterial aneurysms and tortuosity, hypertelorism, bifid uvula or cleft palate, and arterial tortuosity. Dissection can occur at diameters smaller than seen in Marfan syndrome.
Vascular Ehlers-Danlos Syndrome (Type IV)
Vascular EDS is caused by mutations in COL3A1 and is characterised by arterial dissection and rupture, organ rupture (bowel, uterus), thin translucent skin, and characteristic facial features. Life expectancy is markedly reduced (median ~50 years).
- Surgery is high risk — tissue fragility leads to poor wound healing, anastomotic dehiscence, and vascular complications
- Celiprolol (a β1-blocker with β2-agonist properties) has shown benefit in reducing arterial events (European trial data) — not currently PBS-listed in Australia; may be available via Special Access Scheme
- Avoid invasive angiography and unnecessary surgery
- Medical management with blood pressure optimisation is the mainstay
- Genetic counselling and prenatal/preimplantation genetic testing should be discussed
Family Screening Protocol
| Condition | Screening Method | Age to Start | Frequency |
|---|---|---|---|
| Marfan syndrome | Genetic testing + echocardiography | At diagnosis or birth (if family history known) | Echo every 12 months (6-monthly if aortic dilation) |
| Loeys-Dietz syndrome | Genetic testing + CT/MRI arterial imaging | At diagnosis or infancy | Imaging every 6–12 months |
| Vascular EDS | Genetic testing + MRA (avoid arterial catheterisation) | At diagnosis | Imaging annually or as clinically indicated |
| Bicuspid aortic valve aortopathy | Echo + MRI if ascending dilation | At time of BAV diagnosis | Every 3–5 years if <4.0 cm; annually if ≥4.0 cm |
| Familial AAA (1st degree relative) | Abdominal ultrasound | Age 50 or 10 years before index diagnosis | Every 5 years if normal; per size-based protocol if abnormal |
Australian genetic testing: Genetic testing for heritable aortopathies is available through clinical genetics services at major tertiary hospitals and commercial laboratories (e.g., Sonic Genetics, Douglass Hanly Moir). Medicare rebate is available under MBS items 73286–73304 for targeted gene panels when clinical criteria are met.
Medical Management
Medical management of aortic aneurysms aims to slow aneurysm growth, reduce cardiovascular events, and minimise the risk of rupture. The three pillars of medical therapy are blood pressure control, smoking cessation, and statin therapy, with disease-specific modifications for genetic aortopathies.
Blood Pressure Control
Hypertension is a major modifiable risk factor for both aneurysm growth and rupture. Target blood pressure is <130/80 mmHg in all patients with aortic aneurysm (per ESC 2024 and Australian Heart Foundation guidelines).
Beta-Blockers in Marfan Syndrome
Beta-blockers remain the first-line pharmacotherapy for Marfan syndrome to slow aortic root dilation. The proposed mechanism involves reducing aortic wall stress (dP/dt) through heart rate and blood pressure reduction.
Smoking Cessation
Smoking is the single most important modifiable risk factor for AAA development, growth, and rupture. All patients with aortic aneurysm who smoke must be offered structured smoking cessation support.
Statin Therapy
Statin therapy is recommended for all patients with aortic aneurysm, irrespective of baseline lipid levels. Statins reduce cardiovascular morbidity and mortality (which is the leading cause of death in AAA patients) and may have a modest anti-inflammatory effect on the aneurysm wall, although direct evidence for slowing AAA growth is inconclusive.
Antiplatelet Therapy
Low-dose aspirin (100 mg daily) may be considered in patients with concomitant atherosclerotic cardiovascular disease. However, routine aspirin use in all AAA patients is not mandated due to the lack of evidence showing benefit on aneurysm progression and the potential for increased bleeding risk (particularly relevant in patients on anticoagulation for atrial fibrillation).
Summary — Medical Management Quick Reference
Special Populations
Pregnancy
Haemodynamic changes: Pregnancy increases cardiac output by 30–50% and blood volume by 40–50%, placing significant stress on the aortic wall. Risk of dissection is highest in the third trimester and peripartum period.
Marfan syndrome: Pre-conception aortic root assessment is mandatory. Prophylactic root replacement recommended if ≥4.5 cm before conception. If aortic root <4.0 cm, pregnancy may proceed with close echocardiographic surveillance (every trimester, then 6-weekly from 20 weeks).
Loeys-Dietz syndrome: Pregnancy is HIGH RISK. Multidisciplinary planning with obstetrics, cardiology, cardiothoracic surgery, and anaesthetics is essential.
Medications: Atenolol is teratogenic (FDA category D) — switch to metoprolol or labetalol. Losartan and all ARBs are contraindicated in pregnancy (teratogenic). ACE inhibitors are contraindicated. Statins should be ceased pre-conception.
Mode of delivery: Vaginal delivery with epidural and short second stage preferred if aortic root <4.0 cm. Caesarean section recommended if aortic root ≥4.0–4.5 cm or if there is significant aortic dilation.
Refer all women with aortic aneurysm or genetic aortopathy to a combined cardio-obstetric clinic (available at Royal Women's Hospital Melbourne, Mater Mothers' Brisbane, Royal Hospital for Women Sydney).
Paediatrics
Paediatric aortic aneurysms are rare and almost always associated with genetic conditions (Marfan, LDS, Turner syndrome, bicuspid aortic valve, Williams syndrome).
Imaging: Echocardiography is the primary modality. MRI preferred over CT to reduce cumulative radiation in children. Use Z-scores (indexed to body surface area) for aortic root assessment — absolute diameter thresholds are unreliable in growing children.
Pharmacotherapy: Beta-blockers (atenolol 1–2 mg/kg/day or metoprolol 1–2 mg/kg/day) are first-line in Marfan syndrome. Losartan (0.7 mg/kg/day) may be added. Ensure regular growth monitoring.
Activity restriction: Avoid competitive sport and isometric exercise. Isotonic aerobic exercise at moderate intensity is permissible. Individualised exercise prescription guided by a sports cardiologist.
Surgical thresholds: Less defined in paediatrics; surgery considered when Z-score >5 or when rapid growth occurs despite optimal medical therapy.
Refer to a paediatric cardiology service (Royal Children's Hospital Melbourne, Children's Health Queensland, The Children's Hospital at Westmead).
Elderly
Comorbidity burden: Elderly patients with AAA frequently have significant comorbidities (ischaemic heart disease, COPD, CKD, diabetes) that influence the decision to offer elective repair.
EVAR vs open: EVAR is preferred in elderly patients with significant comorbidities due to lower 30-day mortality and shorter recovery. However, lifelong surveillance requirements must be factored in.
Conservative management: May be appropriate for patients with limited life expectancy (<2 years), severe comorbidities precluding any intervention, or patient preference. This decision should be made in partnership with the patient and family.
Blood pressure targets: Cautious reduction in the very elderly (>80 years) to avoid orthostatic hypotension and falls — systolic target 130–150 mmHg may be acceptable.
Renal protection: Minimise contrast studies; use CO2 angiography or low-osmolar contrast with pre-hydration if imaging is required. Monitor renal function post-EVAR (contrast-induced nephropathy risk).
Functional status assessment (frailty scoring, e.g., Clinical Frailty Scale) should inform surgical decision-making. Consider referral for comprehensive geriatric assessment.
Renal Impairment
CKD prevalence: Approximately 20–30% of AAA patients have CKD (eGFR <60 mL/min). CKD is associated with faster aneurysm growth and higher operative mortality.
Contrast precautions: Use lowest possible contrast volume for CT angiography. Pre-hydrate with normal saline (1 mL/kg/h for 12 hours pre- and post-procedure). Consider CO2 angiography. Avoid metformin for 48 hours post-contrast if eGFR <30.
Drug adjustments: Reduce statin dose with caution (atorvastatin does not require renal dose adjustment; rosuvastatin max 10 mg if eGFR <30). Reduce amlodipine is not required. Adjust beta-blocker doses (atenolol dose reduction if eGFR <30). ARBs require potassium monitoring.
EVAR considerations: Suprarenal fixation stent-grafts may further compromise renal function. Monitor serum creatinine and eGFR at 1, 3, and 6 months post-EVAR.
Renal artery involvement in thoraco-abdominal aneurysms requires planning with renal perfusion preservation (fenestrated/branched endografts or renal artery reimplantation).
Immunocompromised
Infective (mycotic) aneurysm: Immunocompromised patients (HIV, transplant recipients, chemotherapy) are at increased risk of mycotic aneurysm from bacteraemia (Salmonella, Staphylococcus aureus). These aneurysms are typically saccular, rapidly expanding, and require urgent surgical intervention combined with prolonged IV antibiotics (6 weeks minimum).
Inflammatory aortitis: Consider giant cell arteritis, IgG4-related disease, and other vasculitides as causes of aortic dilation in immunocompromised or immunosuppressed patients. Biopsy and immunosuppressive therapy (corticosteroids ± tocilizumab) may be required.
Post-operative infections: Prosthetic graft infections are a serious complication (mortality 25–50%). Higher risk in immunocompromised patients. Use prophylactic antibiotics per eTG guidelines; lifelong graft surveillance may be required.
Consult infectious disease specialist for any suspected mycotic aneurysm. Blood cultures (×3 sets) must be obtained before antibiotic initiation.
Aboriginal and Torres Strait Islander Health
While the prevalence of AAA appears to be lower in Aboriginal and Torres Strait Islander populations compared to non-Indigenous Australians, the consequences of delayed diagnosis and limited access to vascular surgical services are disproportionately severe. Culturally safe healthcare delivery, community-based screening, and improved specialist access are critical to reducing the burden of aortic aneurysm disease.
- Incorporate abdominal aortic ultrasound into MBS 715 health assessments for men aged ≥50 years (earlier threshold than non-Indigenous screening)
- Aggressively manage cardiovascular risk factors — smoking cessation is the priority intervention
- Establish pathways for vascular surgery referral through regional hospitals and ACCHS networks
- Use telehealth to connect patients with metropolitan vascular specialists for ongoing surveillance
- Advocate for expanded visiting vascular surgery and interventional radiology services to regional and remote centres
Investigations
Imaging is the cornerstone of aortic aneurysm diagnosis, surveillance, and operative planning. The choice of modality depends on the clinical context, anatomical location, patient factors, and need for procedural planning.
Baseline Investigations for All Patients with Aortic Aneurysm
- Full blood count, renal function (eGFR), liver function tests, HbA1c, lipid profile
- ECG — assess for ischaemic heart disease, LVH, arrhythmia
- Echocardiography — assess aortic root, LV function, valvular disease
- Ankle-brachial pressure index (ABPI) — assess for concomitant peripheral artery disease
- Pulmonary function tests if COPD suspected — impacts fitness for open repair
📚 References
- 1. Wanhainen A, Verzini F, Van Herzeele I, et al. European Society for Vascular Surgery (ESVS) 2019 clinical practice guidelines on the management of abdominal aorto-iliac artery aneurysms. Eur J Vasc Endovasc Surg. 2019;57(1):8–93.
- 2. Erbel R, Aboyans V, Boileau C, et al. 2014 ESC guidelines on the diagnosis and treatment of aortic diseases. Eur Heart J. 2014;35(41):2873–2926.
- 3. Hiratzka LF, Bakris GL, Beckman JA, et al. 2010 ACCF/AHA/AATS/ACR/ASA/SCA/SCAI/SIR/STS/SVM guidelines for the diagnosis and management of patients with thoracic aortic disease. Circulation. 2010;121(13):e266–e369.
- 4. Loeys BL, Dietz HC, Braverman AC, et al. The revised Ghent nosology for the Marfan syndrome. J Med Genet. 2010;47(7):476–485.
- 5. Loeys BL, Schwarze U, Holm T, et al. Aneurysm syndromes caused by mutations in the TGF-beta receptor. N Engl J Med. 2006;355(8):788–798.
- 6. Brady AR, Thompson SG, Fowkes FGR, Greenhalgh RM, Powell JT. Abdominal aortic aneurysm expansion: risk factors and time intervals for surveillance. Circulation. 2004;110(1):16–21.
- 7. United Kingdom Small Aneurysm Trial Participants. Long-term outcomes of immediate repair compared with surveillance of small abdominal aortic aneurysms. N Engl J Med. 2002;346(19):1445–1452.
- 8. IMPROVE Trial Investigators. Endovascular or open repair strategy for ruptured abdominal aortic aneurysm: 30 day outcomes from the IMPROVE randomised trial. BMJ. 2014;348:f7661.
- 9. Groenink M, den Hartog AW, Franken R, et al. Losartan reduces aortic rate of dilation in patients with Marfan syndrome: a randomised controlled trial (COMPARE). Eur Heart J. 2013;34(45):3491–3500.
- 10. Moll FL, Powell JT, Fraedrich G, et al. Management of abdominal aortic aneurysms: clinical practice guidelines of the European Society for Vascular Surgery. Eur J Vasc Endovasc Surg. 2011;41(Suppl 1):S1–S58.
- 11. Australian Institute of Health and Welfare (AIHW). Cardiovascular disease in Australia 2024. Canberra: AIHW; 2024.
- 12. Golledge J, Muller J, Daugherty A, Norman P. Abdominal aortic aneurysm: pathogenesis and implications for management. Arterioscler Thromb Vasc Biol. 2006;26(12):2605–2613.
- 13. National Health and Medical Research Council (NHMRC). National statement on ethical conduct in human research. Canberra: NHMRC; 2023.
- 14. Bown MJ, Sutton AJ, Bell PR, Sayers RD. A meta-analysis of 50 years of ruptured abdominal aortic aneurysm repair. Br J Surg. 2002;89(6):714–730.
- 15. Devereux RB, de Simone G, Arnett DK, et al. Normal limits in relation to age, body size and gender of two-dimensional echocardiographic aortic root dimensions in persons ≥15 years of age. Am J Cardiol. 2012;110(8):1189–1194.