📋 Key Information Summary
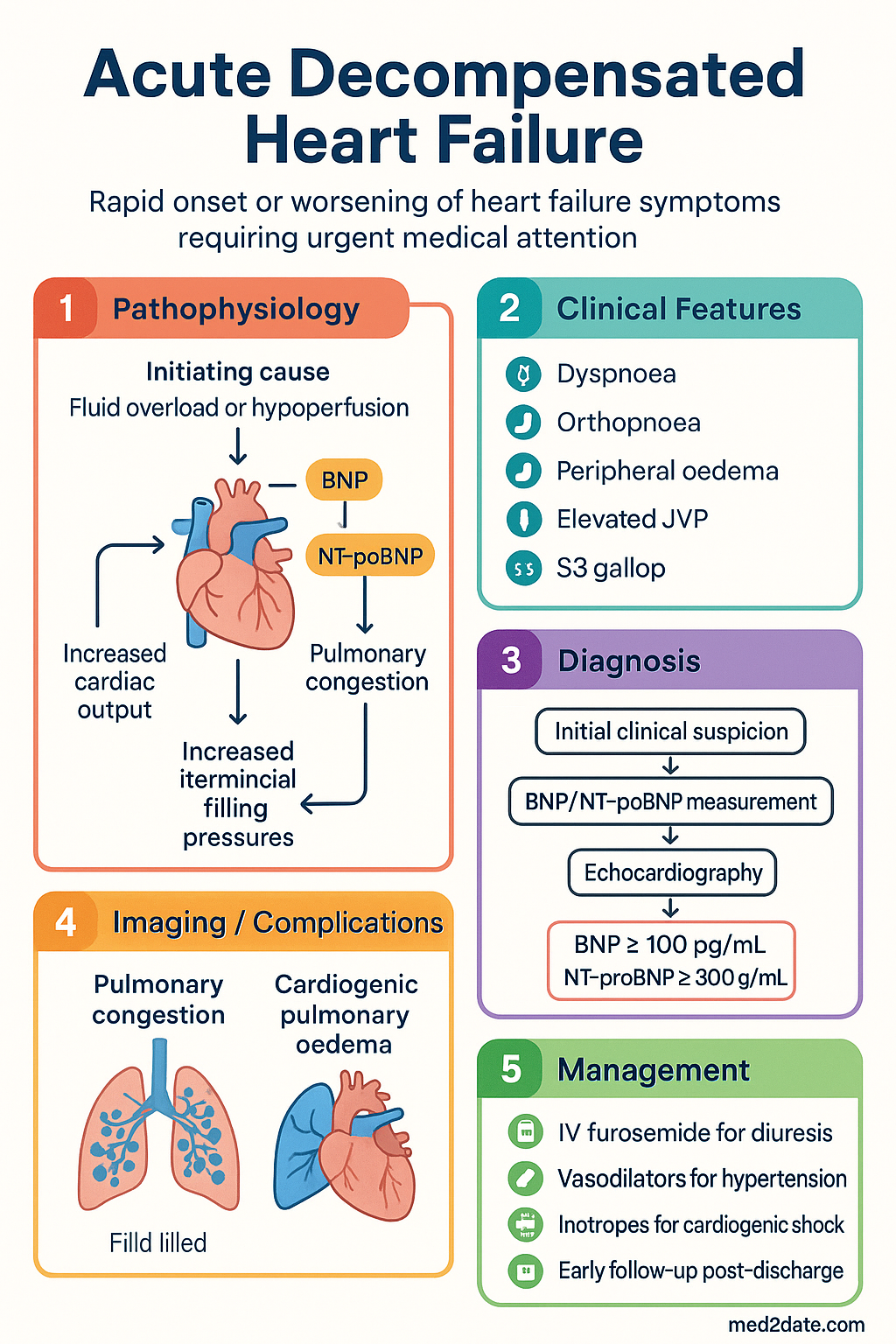
- Acute decompensated heart failure (ADHF) presents with dyspnoea, fluid overload, and/or hypoperfusion and accounts for over 60,000 hospitalisations annually in Australia.
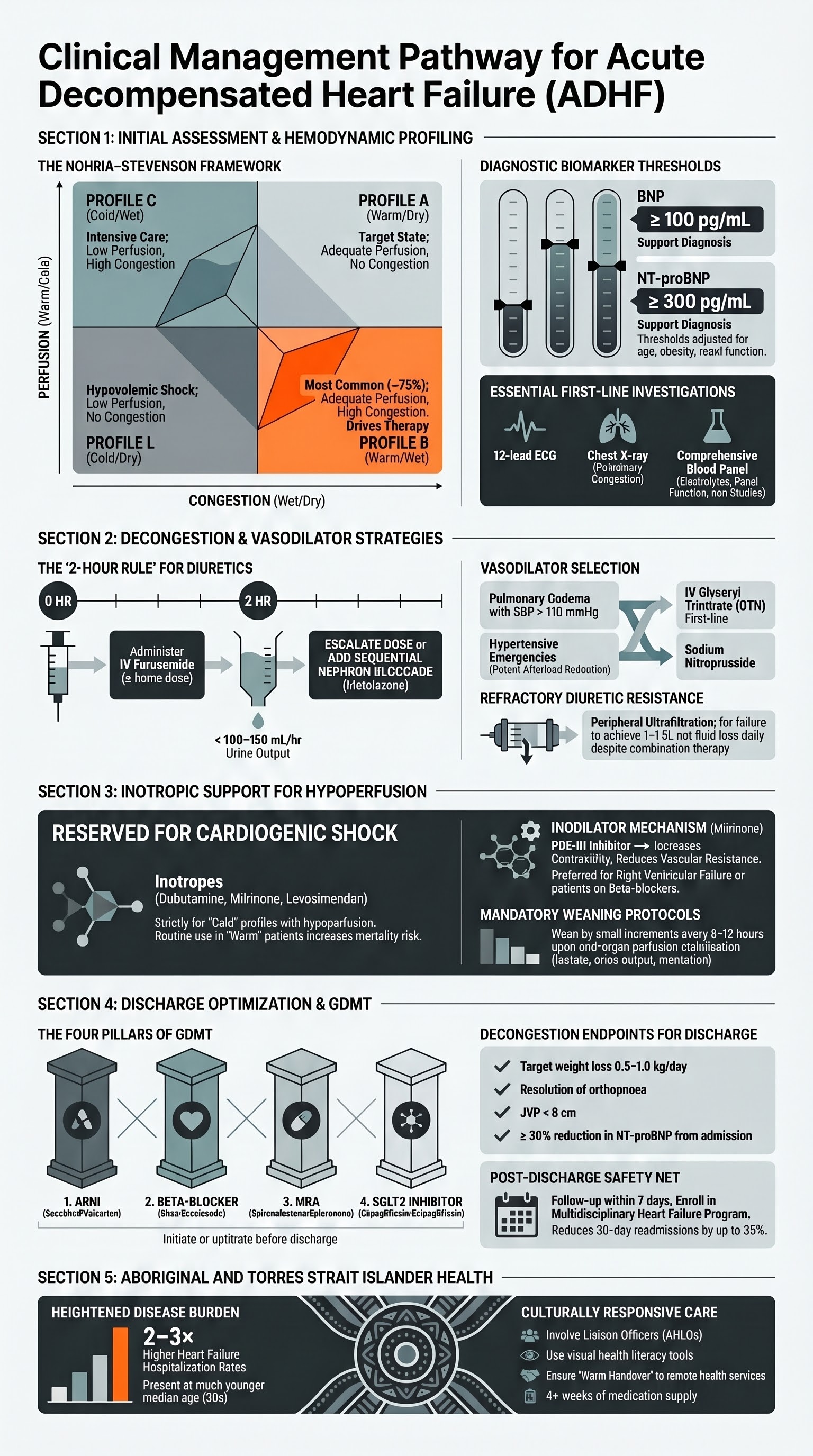
- Classify patients using the Nohria–Stevenson haemodynamic profile: warm–dry (compensated), warm–wet (congestion only), cold–dry (hypoperfusion), cold–wet (congestion + hypoperfusion) — this drives initial therapy.
- BNP ≥ 100 pg/mL or NT-proBNP ≥ 300 pg/mL supports diagnosis; serial measurement aids prognostication but must be interpreted in clinical context (obesity, AF, renal impairment alter thresholds).
- IV furosemide is first-line diuretic therapy; administer at ≥ the patient's home oral dose (or 1 mg IV ≈ 2 mg PO furosemide), given as bolus or continuous infusion, reassessing diuretic response at 2 hours via urine output.
- Diuretic resistance (inadequate diuresis despite high-dose loop diuretics) should prompt sequential nephron blockade with metolazone or thiazide, or consideration of ultrafiltration in refractory cases.
- IV glyceryl trinitrate (GTN) is the primary vasodilator for ADHF with hypertension and pulmonary oedema; start at 10–20 mcg/min and titrate to SBP target; avoid in severe aortic stenosis or SBP < 90 mmHg.
- Inotropic agents (dobutamine, milrinone, levosimendan) are reserved for cardiogenic shock or severe hypoperfusion; they increase mortality risk with routine use and should be weaned as soon as clinically feasible.
- Decongestion endpoints include weight loss ≥ 0.5–1.0 kg/day, net fluid loss ≥ 1–1.5 L/day, resolution of orthopnoea, JVP < 8 cm, and absence of peripheral oedema — aim for euvolaemia before discharge.
- Optimise guideline-directed medical therapy (GDMT) before discharge: ACEi/ARB/ARNI, beta-blocker, MRA, SGLT2 inhibitor — initiate or uptitrate during admission where tolerated.
- Early follow-up within 7 days of discharge is critical; multidisciplinary heart failure programs reduce 30-day readmission rates by 25–35% and are recommended by the Australian Clinical Standards for Heart Failure.
- Aboriginal and Torres Strait Islander Australians have 2–3× the heart failure hospitalisation rate; culturally responsive care, remote access pathways, and cardiac rehabilitation programmes are essential to reduce disparities.
- SGLT2 inhibitors (dapagliflozin, empagliflozin) are now a foundational pillar of HF therapy regardless of diabetes status; initiate in-hospital once euvolaemic and haemodynamically stable.
Introduction & Australian Epidemiology
Acute decompensated heart failure (ADHF) is a clinical syndrome characterised by the rapid onset or worsening of symptoms and signs of heart failure requiring urgent medical attention and often hospitalisation. It encompasses a heterogeneous group of presentations ranging from acute pulmonary oedema to cardiogenic shock, and may occur in patients with previously diagnosed chronic heart failure (HF) or as the de novo manifestation of cardiac disease.
In Australia, heart failure affects an estimated 480,000 individuals, with prevalence rising sharply with age — affecting up to 10–15% of Australians aged ≥ 75 years. The Australian Institute of Health and Welfare (AIHW) reports approximately 62,000 hospitalisations per year with a principal diagnosis of heart failure, making it one of the leading causes of acute medical admission. In-hospital mortality ranges from 4–8%, with 30-day readmission rates of 20–30%, representing a significant burden on the Australian healthcare system estimated at over $2.7 billion annually.
Approximately half of all HF hospitalisations in Australia involve heart failure with reduced ejection fraction (HFrEF, LVEF ≤ 40%), while heart failure with preserved ejection fraction (HFpEF, LVEF ≥ 50%) accounts for a growing proportion, particularly in older, female, and hypertensive populations. Heart failure with mildly reduced ejection fraction (HFmrEF, LVEF 41–49%) is increasingly recognised as a distinct entity.
The Australian Clinical Standards for Heart Failure (ACSQHC, 2021) and the National Heart Foundation of Australia / Cardiac Society of Australia and New Zealand (CSANZ) guidelines provide the framework for evidence-based management. This article focuses on the acute in-hospital management of ADHF, with emphasis on classification, pharmacotherapy, and the transition to optimal outpatient care.
Initial Assessment & Classification
Clinical Presentation
Patients with ADHF typically present with one or more of the following: acute dyspnoea at rest or with minimal exertion, orthopnoea, paroxysmal nocturnal dyspnoea, peripheral oedema, weight gain over days, fatigue, and exercise intolerance. Physical examination findings include elevated jugular venous pressure (JVP), bibasilar crackles, S3 gallop, peripheral oedema, hepatomegaly, and cool extremities (in low-output states).
Haemodynamic Classification — The Nohria–Stevenson Profiles
The cornerstone of initial ADHF assessment is the rapid haemodynamic classification using the Nohria–Stevenson framework, which categorises patients along two axes: perfusion (warm vs cold) and volume status (wet vs dry).
Clinical Assessment Priorities
- History: Prior HF diagnosis, LVEF, current medications, dietary indiscretion, medication non-adherence, recent intercurrent illness (AF, ACS, PE, infection, anaemia).
- Examination: JVP, lung crackles, S3/S4, peripheral oedema grade, capillary refill time, urine output (insert catheter if oliguric or shock), hepatomegaly, ascites.
- Vital signs: HR, BP (arm + leg if coarctation suspected), SpO₂, RR, temperature, weight (if recent baseline available).
BNP and NT-proBNP
Natriuretic peptides are essential in confirming the diagnosis and assessing severity. BNP and NT-proBNP are available through all Australian public hospital pathology services and most community laboratories (MBS item 66546 — BNP; MBS item 66551 — NT-proBNP).
| Biomarker | Exclusion Threshold | Grey Zone | Likely ADHF |
|---|---|---|---|
| BNP | < 100 pg/mL | 100–400 pg/mL | > 400 pg/mL |
| NT-proBNP | < 300 pg/mL | 300–2000 pg/mL (age-dependent) | > 2000 pg/mL (≥ 75 yrs: > 450; 50–75 yrs: > 900) |
Essential Initial Investigations
Diuretic Strategies
Intravenous loop diuretics are the mainstay of decongestion therapy in ADHF. The goal is to achieve effective diuresis — defined as a net fluid loss of 1–1.5 litres per day and weight loss of 0.5–1.0 kg/day — with attention to renal function and electrolyte balance.
First-Line: IV Furosemide
Alternative: Bumetanide
The "2-Hour Rule" — Assessing Diuretic Response
After each IV diuretic dose, urine output should be measured over 2 hours (indwelling catheter recommended for all inpatients receiving IV diuretics). The response guides escalation:
| 2-Hour Urine Output | Response | Action |
|---|---|---|
| > 200 mL (furosemide) / > 60 mL (bumetanide) | Good response | Repeat same dose at 4–6 hourly intervals or convert to continuous infusion |
| 100–200 mL (furosemide) / 30–60 mL (bumetanide) | Partial response | Double the diuretic dose; reassess at 2 hours |
| < 100 mL (furosemide) / < 30 mL (bumetanide) | Poor response (diuretic resistance) | Add sequential nephron blockade (metolazone) or switch strategy; consider ultrafiltration |
Diuretic Resistance
Diuretic resistance is defined as failure to achieve adequate diuresis despite escalating doses of IV loop diuretics. Causes include: inadequate dose, poor gut absorption (in severe oedema), excessive sodium intake, NSAID use, severe renal impairment, nephrotic syndrome, and neurohormonal activation causing sodium avidity.
Ultrafiltration
Peripheral ultrafiltration (UF) involves extracorporeal removal of isotonic fluid via a central venous catheter or large-bore peripheral IV. The AVOID-HF and CARRESS-HF trials have provided mixed evidence; UF is generally reserved for patients with refractory congestion unresponsive to combination diuretic therapy, particularly when renal function is deteriorating ("cardiorenal syndrome"). Australian centres with HF specialist services (e.g., major tertiary hospitals) offer UF; referral to a HF cardiologist is required. Rate of fluid removal is typically 200–500 mL/hr, tailored to haemodynamic tolerance.
Vasodilator Therapy
Vasodilators are indicated in ADHF with congestion and adequate or elevated blood pressure (warm–wet profile, typically SBP > 110 mmHg). They reduce preload (venodilation) and afterload (arteriolar dilation), rapidly improving symptoms of pulmonary oedema. The choice of vasodilator depends on severity, blood pressure, and local availability.
Vasodilator Selection Guide
| Scenario | Preferred Agent | Rationale |
|---|---|---|
| Acute pulmonary oedema, SBP > 140 | IV GTN | Rapid onset, titratable, widely available |
| Hypertensive HF emergency | IV Nitroprusside or GTN (high dose) | Potent afterload reduction; requires arterial line |
| Warm–wet, SBP 100–140 | IV GTN (conservative titration) ± diuretic | Titrate cautiously; monitor BP closely |
| ADHF with RV predominant failure | Avoid GTN; consider nitroprusside if afterload excess | RV preload-dependent; nitrates can precipitate cardiovascular collapse |
Inotropic Support
Inotropic agents are reserved for ADHF with evidence of hypoperfusion (cold profiles — Nohria–Stevenson C or L) manifesting as: hypotension (SBP < 90 mmHg or MAP < 65 mmHg), signs of end-organ hypoperfusion (oliguria, altered mentation, rising lactate, cool extremities), and cardiogenic shock. These agents carry significant risk — including arrhythmia, myocardial ischaemia, and increased mortality — and should be used at the lowest effective dose for the shortest possible duration.
Indications for Inotropic Support
- Cardiogenic shock (SBP < 90 mmHg + signs of hypoperfusion + raised filling pressures)
- Low-output syndrome post-cardiac surgery or acute myocardial infarction
- Bridge to decision / bridge to advanced therapies (transplant, LVAD)
- Acute decompensation of severe chronic HF (LVEF < 25%) with end-organ dysfunction despite optimal diuretic and vasodilator therapy
- Right ventricular failure with haemodynamic compromise
Weaning Protocols
Weaning of inotropic support should begin as soon as clinical improvement permits. The approach varies by agent:
Discharge Planning
Discharge planning begins on the day of admission and is a critical determinant of 30-day readmission — the key quality metric for ADHF care in Australia. The ACSQHC Clinical Standards for Heart Failure (2021) mandate structured discharge processes including medication reconciliation, patient education, and early follow-up.
Decongestion Endpoints Before Discharge
Patients should not be discharged until adequate decongestion is achieved. Residual congestion at discharge is the single strongest predictor of 30-day readmission. Clinical targets include:
| Endpoint | Target | Assessment |
|---|---|---|
| Weight loss | ≥ 0.5–1.0 kg/day during active diuresis | Daily weight (same time, same scale, same clothing) |
| Net fluid loss | ≥ 1–1.5 L/day (or ≥ 100 mL/hr urine during diuresis) | Strict I&O chart; catheter removal once target reached |
| Orthopnoea | Resolution (can lie flat or ≤ 1 pillow) | Patient report |
| JVP | < 8 cm H₂O (not visible at 45°) | Clinical examination |
| Peripheral oedema | Trace or absent | Pitting oedema grading |
| NT-proBNP trajectory | ≥ 30% reduction from admission level | Pre-discharge bloods (BNP/NT-proBNP) |
| Renal function | Stable or acceptable rise (up to 30% ↑ creatinine tolerated if congestion resolving) | UEC on day of discharge |
Guideline-Directed Medical Therapy (GDMT) Optimisation
Every ADHF admission is an opportunity to initiate or uptitrate the four foundational pillars of HFrEF therapy. The "Start Low, Go Slow" approach applies during acute illness, but therapy should be started before discharge whenever feasible.
Additional Medications at Discharge
- Oral diuretic: Transition IV furosemide to oral at 2× the IV dose (e.g. 40 mg IV → 80 mg PO). Some patients require 1:1 conversion with bumetanide. Discharge on a maintenance dose; patients may self-adjust (HF nurse-led titration) based on daily weight.
- Iron replacement: If iron deficiency identified (ferritin < 100 or ferritin 100–299 with TSAT < 20%), IV iron (ferric carboxymaltose/Ferinject® 500–1000 mg IV single dose) improves symptoms and exercise capacity (AFFIRM-AHF, IRONMAN trials). PBS Authority Required for IV iron in HF.
- Anticoagulation: If concurrent AF, ensure appropriate anticoagulation (DOAC preferred: apixaban, rivaroxaban, dabigatran, edoxaban). Assess CHA₂DS₂-VASc and HAS-BLED scores.
- Vaccination: Ensure influenza (annual) and pneumococcal (Prevenar 13® + Pneumovax 23®) vaccination are up to date.
Early Follow-Up & Readmission Prevention
Special Populations
Pregnancy
- Peripartum cardiomyopathy: Presents in the last month of pregnancy or within 5 months postpartum. LVEF < 45% in the absence of other causes. Incidence in Australia ~1:1000 pregnancies.
- ACEi/ARB/ARNI: Contraindicated in pregnancy (teratogenic — renal agenesis, oligohydramnios). Use hydralazine + nitrate combination as alternative vasodilator.
- Beta-blockers: Labetalol or metoprolol preferred (relatively safe in pregnancy). Carvedilol — limited safety data; avoid if possible.
- Diuretics: Furosemide — may reduce placental perfusion; use cautiously for fluid overload. Avoid thiazides (neonatal thrombocytopaenia risk).
- MRA: Spironolactone — anti-androgenic effects in first trimester; contraindicated. Eplerenone — limited data; avoid.
- SGLT2 inhibitors: Contraindicated in pregnancy and breastfeeding.
- Delivery planning: Multidisciplinary team (obstetrics, cardiology, anaesthesia). Vaginal delivery preferred with epidural and passive second stage. C-section only for obstetric indications.
Paediatrics
- Aetiology: Congenital heart disease, myocarditis, dilated cardiomyopathy, and inborn errors of metabolism are the leading causes of paediatric HF in Australia.
- Diuretics: Furosemide 0.5–1 mg/kg/dose IV q6–12h (max 6 mg/kg/day). Oral: 1–2 mg/kg BD. Monitor closely for dehydration and electrolyte disturbance.
- ACEi: Enalapril 0.1 mg/kg PO BD (start low, titrate). Captopril 0.1–0.3 mg/kg PO TDS for neonates.
- Beta-blockers: Carvedilol 0.05 mg/kg PO BD, uptitrate to 0.4 mg/kg BD. Limited paediatric evidence — use with specialist guidance.
- BNP in children: Higher baseline values than adults. NT-proBNP > 300 pg/mL is suggestive in children; age-specific reference ranges apply.
- Referral: All paediatric HF patients should be managed at a paediatric cardiac centre (e.g., Royal Children's Melbourne, Children's Hospital Westmead, Queensland Children's Hospital).
Elderly (≥ 75 years)
- HFpEF prevalence: Over 50% of HF admissions in those ≥ 75 years are HFpEF. Diagnostic criteria include typical symptoms, preserved LVEF, and evidence of diastolic dysfunction/raised filling pressures.
- Diuretic caution: Increased risk of hypotension, falls, prerenal AKI, and electrolyte derangement. Start at lower doses and titrate slowly. Avoid over-diuresis (dry = hypotension + AKI).
- Polypharmacy: Conduct a comprehensive medication review. Deprescribe nephrotoxic agents (NSAIDs), anticholinergics, and medications contributing to fluid retention. Involve a pharmacist.
- Frailty assessment: Use validated tools (Clinical Frailty Scale). Frailty predicts mortality independent of HF severity and informs goals of care.
- SGLT2 inhibitors: Effective in HFpEF (EMPEROR-Preserved, DELIVER trials). Well tolerated in the elderly — monitor for genital mycotic infections and volume depletion.
Renal Impairment
- Cardiorenal syndrome: Worsening renal function during ADHF treatment is common (up to 30%). A creatinine rise of up to 30% is acceptable if congestion is improving ("pseudo-worsening"). Avoid stopping diuretics prematurely.
- Diuretics: Higher IV furosemide doses needed (up to 250 mg IV bolus). Continuous infusion may be more effective. Metolazone retains efficacy in severe CKD (unlike thiazides).
- ACEi/ARB/ARNI: Continue if eGFR ≥ 25 and K⁺ < 5.5. May need dose reduction. Monitor UEC at 48 hrs after initiation or dose change.
- MRA: Contraindicated if eGFR < 30 or K⁺ ≥ 5.0. Use lower doses (12.5–25 mg spironolactone). Monitor closely.
- SGLT2 inhibitors: Can be initiated if eGFR ≥ 20 (per current PBS criteria). Benefits attenuate but do not disappear with declining GFR. Do not use for glycaemic control below eGFR 45; use for HF benefit regardless.
- Dialysis: Refractory fluid overload with CKD may require haemodialysis or haemodiafiltration. Discuss with nephrology early.
Hepatic Impairment
- Congestive hepatopathy: Raised ALT/AST and bilirubin are common in ADHF from hepatic venous congestion. Differentiate from ischaemic hepatitis (acute ALT > 1000) which suggests severe low cardiac output.
- Diuretics: Hepatomegaly and ascites may impair GI absorption of oral diuretics — use IV route. Monitor for hepatorenal physiology (Type 2 HRS) in severe right heart failure.
- ACEi/ARB: Use with caution in severe hepatic impairment (Child-Pugh C). Metabolism of some agents is hepatic (e.g. losartan). No adjustment needed for most agents in mild-moderate impairment.
- Anticoagulation: DOACs contraindicated in Child-Pugh C; warfarin with INR monitoring preferred. Apixaban may be used in Child-Pugh B with caution.
Immunocompromised
- Consider broader differentials: Myocarditis (viral, CMV, EBV, HIV), cardiac allograft rejection (post-transplant), drug-induced cardiotoxicity (anthracyclines, checkpoint inhibitors, trastuzumab), cardiac sarcoidosis.
- Immunosuppression interactions: Cyclosporin and tacrolimus cause renal impairment and hypertension — interacts with diuretic and ACEi therapy. Corticosteroids cause fluid retention and hyperglycaemia.
- Chemotherapy-related HF: If anthracycline-related cardiomyopathy suspected, initiate standard HF GDMT. ACEi/ARB + carvedilol may have cardioprotective role if initiated early (OVERCOME trial). Refer cardio-oncology.
- Infection risk: Patients on high-dose diuretics or inotropes with indwelling catheters are at increased risk of line-related sepsis. Minimise line duration; aseptic technique for all central access.
Aboriginal and Torres Strait Islander Health Considerations
Aboriginal and Torres Strait Islander Australians experience heart failure at 2–3 times the rate of non-Indigenous Australians, with significantly younger age at presentation, higher rates of HFrEF (often rheumatic heart disease-related in remote communities), and poorer outcomes including higher 30-day readmission and in-hospital mortality rates (AIHW, 2023). The burden is greatest in remote and very remote communities, where access to cardiology services, echocardiography, and cardiac rehabilitation is limited.
📚 References
- 1. Atherton JJ, Sindone A, De Pasquale CG, et al. National Heart Foundation of Australia and Cardiac Society of Australia and New Zealand: Australian Clinical Guidelines for Heart Failure 2018. Heart Lung Circ. 2018;27(10):1123-1208.
- 2. Australian Commission on Safety and Quality in Health Care (ACSQHC). Clinical Care Standards: Acute Heart Failure Clinical Care Standard. Sydney: ACSQHC; 2021.
- 3. Heidenreich PA, Bozkurt B, Aguilar D, et al. 2022 AHA/ACC/HFSA Guideline for the Management of Heart Failure: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation. 2022;145(18):e895-e1032.
- 4. Felker GM, Lee KL, Bull DA, et al. Diuretic strategies in patients with acute decompensated heart failure. N Engl J Med. 2011;364(9):797-805.
- 5. O'Connor CM, Starling RC, Hernandez AF, et al. Effect of nesiritide in patients with acute decompensated heart failure (ASCEND-HF trial). N Engl J Med. 2011;365(1):32-43.
- 6. Cuffe MS, Califf RM, Adams KF Jr, et al. Short-term intravenous milrinone for acute exacerbation of chronic heart failure: a randomized controlled trial (OPTIME-CHF). JAMA. 2002;287(12):1541-1547.
- 7. Mebazaa A, Nieminen MS, Packer M, et al. Levosimendan vs dobutamine for patients with acute decompensated heart failure (SURVIVE trial). JAMA. 2007;297(17):1883-1891.
- 8. McMurray JJV, Solomon SD, Inzucchi SE, et al. Dapagliflozin in patients with heart failure and reduced ejection fraction (DAPA-HF). N Engl J Med. 2019;381(21):1995-2008.
- 9. Packer M, Butler J, Filippatos GS, et al. Empagliflozin in patients with heart failure, reduced ejection fraction, and volume overload (EMPEROR-Reduced). N Engl J Med. 2020;383(15):1413-1424.
- 10. Anker SD, Butler J, Filippatos G, et al. Empagliflozin in heart failure with a preserved ejection fraction (EMPEROR-Preserved). N Engl J Med. 2021;385(16):1451-1461.
- 11. Vaduganathan M, Claggett BL, Jhund PS, et al. Estimating lifetime benefits of comprehensive disease-modifying pharmacological therapies in patients with heart failure with reduced ejection fraction: a comparative analysis of three randomised controlled trials. Lancet. 2024;403(10422):147-156.
- 12. Australian Institute of Health and Welfare (AIHW). Heart, stroke and vascular disease — Australian facts. AIHW; Canberra: 2023.
- 13. RHDAustralia (ARF/RHD writing group). The 2020 Australian guideline for prevention, diagnosis and management of acute rheumatic fever and rheumatic heart disease. 3rd ed. Darwin: Menzies School of Health Research; 2020.
- 14. Ponikowski P, Voors AA, Anker SD, et al. 2016 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure. Eur Heart J. 2016;37(27):2129-2200.
- 15. Bart BA, Goldsmith SR, Lee KL, et al. Ultrafiltration in decompensated heart failure with cardiorenal syndrome (CARRESS-HF). N Engl J Med. 2012;367(24):2296-2304.