📋 Key Information Summary
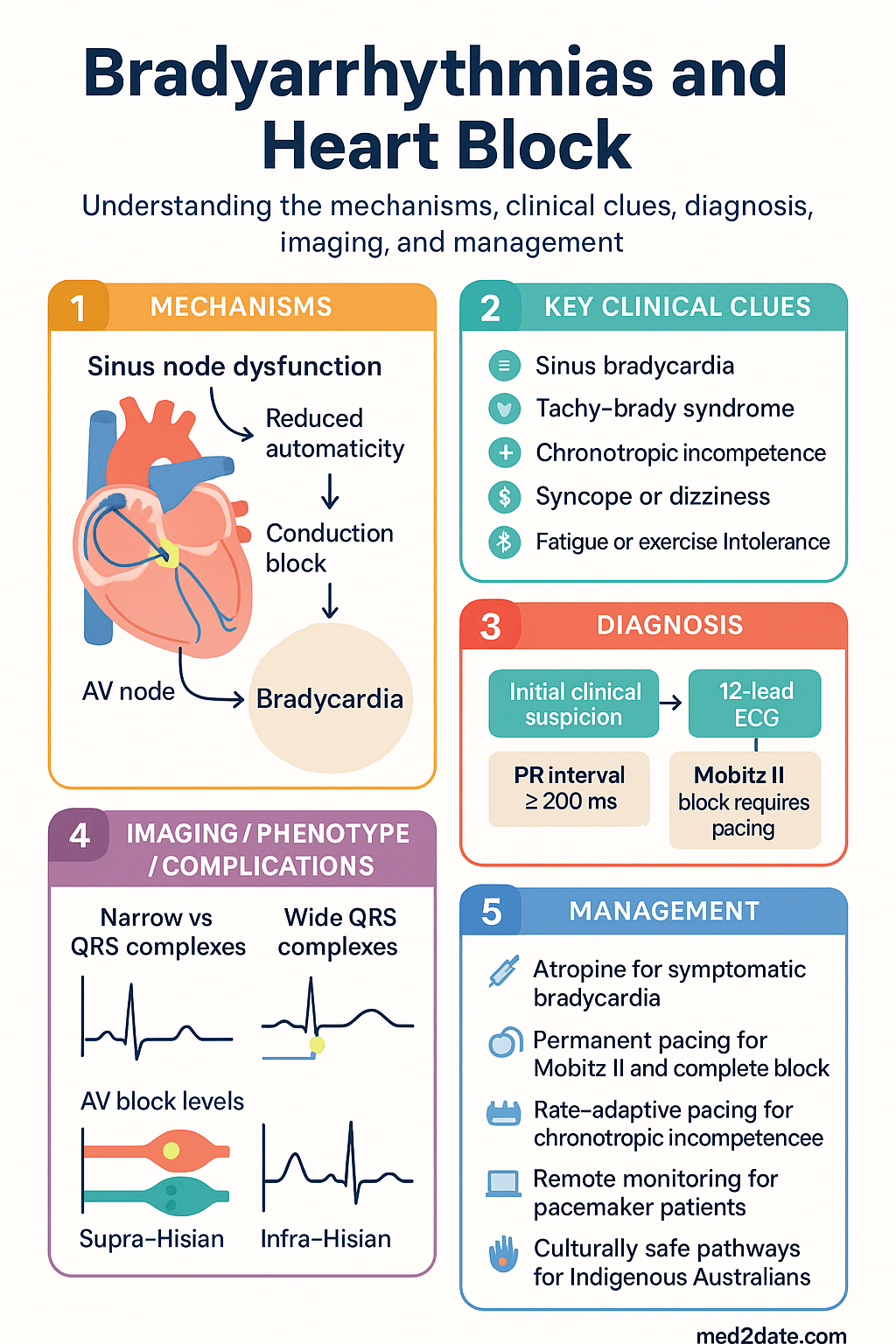
- Bradyarrhythmias encompass disorders of impulse formation (sinus node dysfunction) and impulse conduction (AV block), ranging from asymptomatic ECG findings to life-threatening haemodynamic compromise requiring urgent pacing.
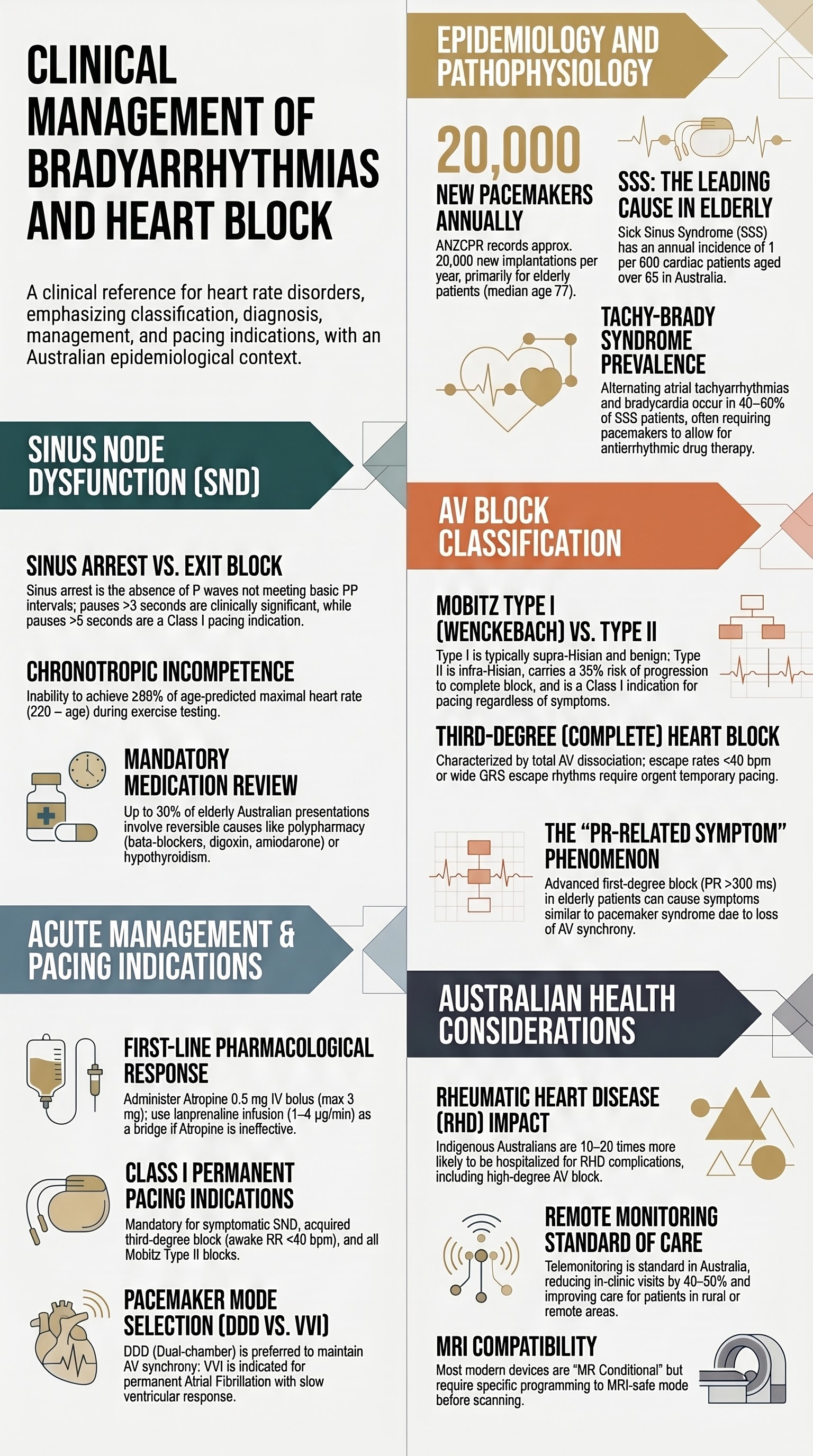
- Sick sinus syndrome (SSS) is the most common cause of bradyarrhythmia in the elderly, with an annual incidence of approximately 1 per 600 cardiac patients aged >65 years in Australia.
- Tachy-brady syndrome (SSS with atrial tachyarrhythmias) occurs in 40–50 % of SSS patients and requires both rate/rhythm control and consideration of permanent pacing.
- Chronotropic incompetence — inability to achieve ≥80 % of age-predicted maximal heart rate — is frequently under-recognised and is diagnosed with exercise testing or cardiopulmonary exercise testing.
- First-degree AV block (PR >200 ms) is usually benign but requires monitoring if PR >300 ms or in the presence of bifascicular block, as progression to higher-grade block may occur.
- Second-degree Mobitz type I (Wenckebach) block at the AV node level is often physiological and rarely requires pacing; Mobitz type II block is infra-Hisian, carries a high risk of progression to complete heart block, and is a Class I indication for permanent pacing.
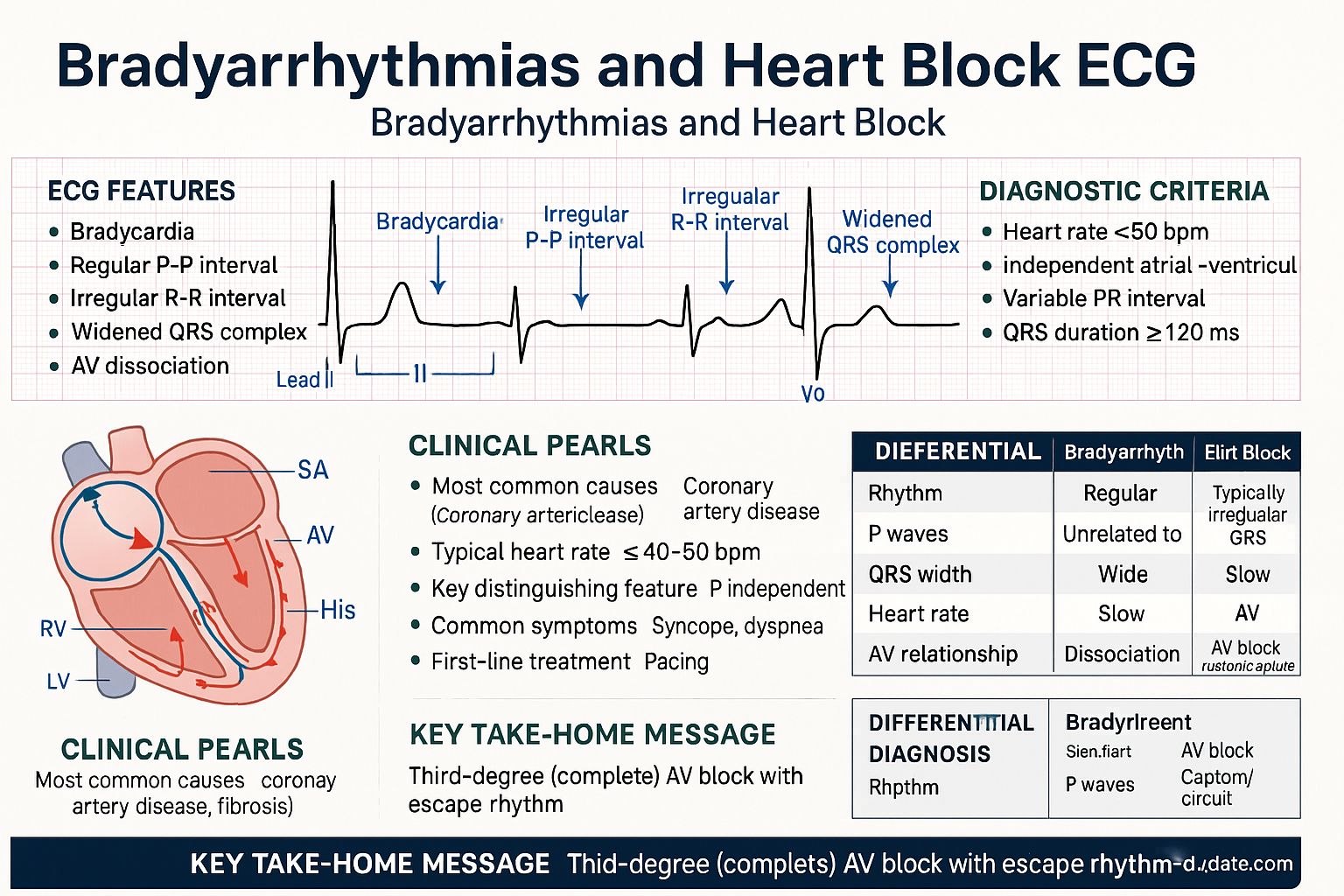
- Third-degree (complete) AV block with symptoms, haemodynamic instability, or an escape rate <40 bpm requires urgent temporary transcutaneous or transvenous pacing, followed by permanent pacemaker implantation.
- Class I indications for permanent pacing include symptomatic bradycardia due to SSS, acquired third-degree AV block with symptoms or awake rates <40 bpm, and second-degree Mobitz type II AV block regardless of symptoms.
- Pacemaker mode selection: dual-chamber (DDD) is preferred when AV synchrony is beneficial; single-chamber ventricular (VVI) is appropriate for permanent atrial fibrillation with slow ventricular response.
- Rate-adaptive (sensor-driven) pacing is essential for patients with chronotropic incompetence; remote monitoring is standard practice in Australian centres and reduces in-person follow-up visits.
- Atropine 0.5–1 mg IV (maximum 3 mg) is the first-line pharmacological agent for symptomatic bradycardia; isoprenaline or adrenaline infusion may be used as a bridge to pacing when atropine is ineffective.
- Aboriginal and Torres Strait Islander Australians have higher rates of rheumatic heart disease–related conduction abnormalities and reduced access to specialist pacing services in remote communities, necessitating culturally safe pathways and outreach programmes.
- All patients receiving a pacemaker should be provided with a device identification card, information regarding electromagnetic interference (MRI compatibility, diathermy), and a structured follow-up schedule including remote monitoring where available.
Introduction & Australian Epidemiology
Bradyarrhythmias are a heterogeneous group of disorders characterised by a heart rate below the physiological range necessary to maintain adequate cardiac output. They result from abnormalities of impulse generation at the sinoatrial (SA) node or impulse conduction through the atrioventricular (AV) node and His-Purkinje system. Clinical significance ranges from asymptomatic electrocardiographic findings in young, athletic individuals to cardiogenic shock and sudden cardiac death in the setting of complete heart block.
In Australia, the Australian Institute of Health and Welfare (AIHW) reports that cardiac arrhythmias account for over 100,000 hospitalisations annually, with conduction disorders comprising a significant proportion. The Australian and New Zealand Cardiac Pacing and Electrophysiology Registry (ANZCPR) records approximately 20,000 new pacemaker implantations per year, the vast majority indicated for bradyarrhythmic indications. The median age at first implantation is 77 years, reflecting the strong age-dependent incidence of degenerative conduction system disease.
The burden of bradyarrhythmias is disproportionately high among Aboriginal and Torres Strait Islander Australians, driven in part by rheumatic heart disease (RHD) and its sequelae. Data from the End Rheumatic Heart Disease in Australia (End RHD) collaboration indicate that Indigenous Australians are 10–20 times more likely to be hospitalised for RHD complications, including high-degree AV block requiring pacing, compared with non-Indigenous Australians.
This guideline provides an evidence-based, Australian-context framework for the diagnosis, classification, and management of bradyarrhythmias and heart block, incorporating the 2023 ACC/AHA/HRS Guideline for Cardiac Pacing and the relevant Therapeutic Guidelines (eTG) recommendations.
Sinus Node Dysfunction
Overview and Pathophysiology
Sinus node dysfunction (SND), also termed sick sinus syndrome (SSS), encompasses a spectrum of disorders of the sinoatrial node resulting in inappropriate sinus bradycardia, sinus pauses, sinus arrest, or sinoatrial exit block. The pathological substrate is typically fibrosis and fatty infiltration of the SA node and perinodal tissue, a degenerative process that increases in prevalence with age. Reversible causes — including medications (beta-blockers, non-dihydropyridine calcium channel blockers, digoxin, amiodarone, ivabradine), hypothyroidism, hyperkalaemia, and increased vagal tone — must always be excluded before attributing symptoms to intrinsic SND.
Clinical Syndromes
| Syndrome | ECG Features | Key Clinical Points |
|---|---|---|
| Sinus bradycardia | Rate <60 bpm, normal P waves, normal PR interval | Often physiological in athletes; pathological if symptomatic or rate <40 bpm at rest |
| Sinoatrial exit block | Type I: progressive PR shortening before dropped P wave. Type II: sudden dropped P wave (pause = multiple of basic PP interval) | Type II more clinically significant; may cause syncope |
| Sinus arrest | Absence of P waves; pause not a multiple of basic PP interval; junctional or ventricular escape may occur | Prolonged pauses (>3 seconds while awake) are significant; pauses >5 seconds during waking hours are a Class I indication for pacing |
| Tachy-brady syndrome | Alternating atrial tachyarrhythmias (AF, flutter, atrial tachycardia) with bradycardia or pauses upon termination | Present in 40–50 % of SSS patients; rate-control drugs may worsen bradycardia; often requires pacemaker to facilitate antiarrhythmic therapy |
| Chronotropic incompetence | Failure to achieve ≥80 % of age-predicted maximal heart rate (220 − age) on exercise testing, or inability to increase heart rate proportionally to metabolic demand | Diagnosed by exercise tolerance test (ETT) or cardiopulmonary exercise testing; may be the sole manifestation of SND; responds to rate-adaptive pacing |
Investigations
Management of Sinus Node Dysfunction
Acute Symptomatic Bradycardia
Chronic Management and Pacing for SND
Permanent pacing is the definitive treatment for symptomatic SND that is not due to reversible causes. The 2023 ACC/AHA/HRS guideline assigns a Class I recommendation for permanent pacing in SND with documented symptomatic bradycardia (including pauses), and Class IIa when symptoms are likely due to bradycardia despite absence of definitive ECG correlation. Pharmacological alternatives are limited; theophylline and caffeine have modest efficacy in mild cases but are not standard of care in Australia.
AV Block Classification
Anatomical Levels of Block
AV block is classified by severity (first-, second-, third-degree) and by anatomical level (supra-Hisian [AV node], intra-Hisian, or infra-Hisian [bundle branches]). The anatomical level determines prognosis, need for pacing, and pacemaker mode selection. His bundle electrogram recording at electrophysiology study can localise the block precisely, but in most clinical scenarios the surface ECG provides sufficient information.
| Feature | Supra-Hisian (AV Node) | Infra-Hisian (His-Purkinje) |
|---|---|---|
| ECG clues | Narrow QRS, Wenckebach pattern, atropine-responsive | Wide QRS (bundle branch block), Mobitz II, atropine-resistant |
| Common causes | Enhanced vagal tone (young, athletes), AV nodal drugs, inferior MI, RHD | Degenerative fibrosis (Lenègre-Lev disease), anterior MI, cardiac surgery, infiltrative disease |
| Prognosis | Generally benign; rarely progresses to complete block | Progression to complete block common; high risk of syncope and sudden death |
| Pacing usually required? | Only if symptomatic and reversible causes excluded | Yes — Class I indication for permanent pacing even if asymptomatic (Mobitz II, alternating bundle branch block) |
First-Degree AV Block
First-degree AV block is defined as a PR interval >200 ms on the surface ECG with 1:1 AV conduction. It is found in up to 5 % of the general population and is usually benign, reflecting prolonged conduction through the AV node. In elderly patients, advanced first-degree AV block (PR >300 ms) may cause symptoms resembling pacemaker syndrome (fatigue, exercise intolerance, cannon A waves) due to loss of AV synchrony — a phenomenon sometimes termed "PR interval–related symptoms." This is a Class IIa indication for permanent dual-chamber pacing.
Second-Degree AV Block
| Parameter | Mobitz Type I (Wenckebach) | Mobitz Type II |
|---|---|---|
| ECG pattern | Progressive PR prolongation before a dropped QRS complex; pause shorter than two PP intervals | Sudden dropped QRS without preceding PR prolongation; constant PR interval for conducted beats |
| Site of block | Usually AV node (supra-Hisian) | His-Purkinje system (infra-Hisian) |
| QRS width | Usually narrow (<120 ms) | Usually wide (≥120 ms), often with bundle branch block |
| Atropine response | Improves conduction (increases AV node conduction) | No benefit or may worsen block |
| Progression to complete block | Rare (<5 %) | Common (up to 35 % within 3 years) |
| Pacing indication | Class IIa if symptomatic; Class IIb if asymptomatic with infra-Hisian block documented on EPS | Class I — permanent pacing regardless of symptoms |
High-Grade AV Block
High-grade AV block is defined as the consecutive dropping of two or more conducted P waves (e.g., 2:1 or 3:1 conduction) with a constant PR interval in conducted beats. It may represent either Mobitz I or Mobitz II type and carries a significant risk of haemodynamic compromise. When the block is at the infra-Hisian level (wide QRS escape), permanent pacing is indicated as for Mobitz II block.
Third-Degree (Complete) AV Block
Third-degree AV block describes complete dissociation of atrial and ventricular activity, with no atrial impulses conducted to the ventricles. The ventricular escape rate depends on the level of the escape focus:
Conduction Disturbances in Acute Myocardial Infarction
| MI Type | Conduction Block | Level | Prognosis | Pacing |
|---|---|---|---|---|
| Inferior STEMI | First-degree, Mobitz I, or complete block | AV node (supra-Hisian) | Usually transient (days); often resolves with reperfusion | Temporary pacing if symptomatic / HR <40 / haemodynamic compromise; permanent pacing if block persists >14 days |
| Anterior STEMI | Mobitz II, new BBB, or complete block | His-Purkinje (infra-Hisian) | High mortality (associated with large infarct); may not recover | Immediate temporary pacing; permanent pacemaker if block persists beyond the acute phase |
Pacemaker Indications
ACC/AHA/HRS Class System
The 2023 ACC/AHA/HRS Guideline for Cardiac Pacing uses the following classification:
- Class I: Benefit >>> Risk — pacing is recommended/is indicated.
- Class IIa: Benefit >> Risk — reasonable to perform pacing; additional studies with focused objectives needed.
- Class IIb: Benefit ≥ Risk — pacing may be considered; additional studies with broad objectives needed.
- Class III (No Benefit): Risk ≥ Benefit — pacing is not recommended.
Class I Indications for Permanent Pacing
Class IIa Indications
- SND with heart rate <40 bpm when a clear temporal relationship with symptoms has not been established (but symptoms are likely bradycardia-related).
- Advanced first-degree AV block (PR >300 ms) with haemodynamic symptoms attributable to loss of AV synchrony.
- Mobitz type I (Wenckebach) AV block with symptoms clearly related to the block itself.
- Asymptomatic third-degree AV block with awake escape rate ≥40 bpm, especially if cardiomegaly or LV dysfunction is present.
- Syncope of undetermined origin when clinically significant infra-Hisian block is found at EPS.
Class IIb Indications
- Minimally symptomatic SND with awake heart rate <40 bpm.
- Asymptomatic Mobitz type I AV block at intra-Hisian level identified at EPS.
- Neuromuscular diseases (e.g., myotonic dystrophy, Kearns-Sayre syndrome) with any degree of AV block, even if asymptomatic, due to unpredictable progression.
Temporary vs Permanent Pacing
- Acute MI with symptomatic bradycardia not responsive to atropine
- Drug toxicity (e.g., beta-blocker, calcium channel blocker, digoxin overdose) with haemodynamic compromise
- Bridge to permanent pacemaker implantation
- Peri-operative bradycardia (e.g., cardiac surgery, certain neurosurgical procedures)
- Overdrive pacing for torsades de pointes or certain atrial tachyarrhythmias
Modalities: Transcutaneous (non-invasive, limited by patient discomfort, muscle capture), transvenous (internal jugular or subclavian, reliable), epicardial (during cardiac surgery).
- Class I or IIa indication documented by guidelines
- Irreversible or non-correctable cause
- Life expectancy and quality of life considerations
- Patient informed consent (including discussion of device longevity, MRI compatibility, electromagnetic interference)
- Prophylactic antibiotics per local protocol (usually cefazolin 2 g IV at induction)
Pacemaker Programming & Follow-up
Mode Selection
| Mode | Code (NBG) | Chambers Paced / Sensed | Best Indication | Limitations |
|---|---|---|---|---|
| Dual-chamber | DDD / DDDR | Atrium + Ventricle (both paced and sensed) | SND with intact AV conduction; AV block with normal sinus node function. Maintains AV synchrony. DDDR adds rate response for chronotropic incompetence. | More complex programming; higher cost; single lead failure affects one chamber; risk of pacemaker-mediated tachycardia (PMT); inappropriate mode switching |
| Single-chamber atrial | AAI / AAIR | Atrium only | Isolated SND with normal AV conduction. Rarely used in modern practice as DDD is preferred to accommodate future AV block. | No ventricular pacing backup; risk if AV block develops (estimated 1–2 % per year in SND) |
| Single-chamber ventricular | VVI / VVIR | Ventricle only | Permanent atrial fibrillation with slow ventricular response (most common indication for VVI in Australia). Also used in elderly patients with limited mobility where AV synchrony is less important. | Loss of AV synchrony → risk of pacemaker syndrome (15–20 %); reduced cardiac output; possible increased risk of AF and thromboembolism |
| Conduction system | His-bundle or LBBAP | Pacing the His bundle or left bundle branch area | Patients with reduced LVEF or high expected ventricular pacing burden; prevents pacing-induced dyssynchrony | Technically more demanding; higher thresholds in some patients; long-term data emerging |
Rate-Adaptive Pacing
Rate-adaptive (sensor-driven) pacing is indicated when chronotropic incompetence is demonstrated or anticipated. The most common sensor is the accelerometer (activity sensor), which detects body movement and adjusts pacing rate accordingly. Minute ventilation sensors measure transthoracic impedance to estimate respiratory rate and tidal volume, providing a more physiological response. Dual-sensor systems (accelerometer + minute ventilation) offer the best rate response in most clinical scenarios.
Remote Monitoring
Remote monitoring (telemonitoring) is now standard of care for all pacemaker and ICD patients in Australia. Major manufacturers (Medtronic CareLink, Abbott Merlin.net, Boston Scientific Latitude, Biotronik Home Monitoring) offer remote interrogation platforms. Evidence from the IN-TIME, CONNECT, and TRUST trials demonstrates that remote monitoring:
- Reduces time to clinical action for significant arrhythmias and device alerts
- Decreases the number of in-clinic follow-up visits by approximately 40–50 %
- Enables earlier detection of lead failure, battery depletion, and atrial fibrillation
- Improves patient satisfaction, particularly in rural and remote Australia where travel to specialist centres is burdensome
Recommended follow-up schedule: first in-clinic review at 2–6 weeks post-implantation, then remote transmission monthly with in-clinic review every 6–12 months. Increase frequency as battery reaches elective replacement indicator (ERI).
Battery Longevity and Device Replacement
| Device Type | Typical Longevity | ERI to EOS Interval | Factors Affecting Longevity |
|---|---|---|---|
| Single-chamber pacemaker (VVIR) | 10–15 years | 3–6 months | Percentage ventricular pacing; lead impedance; programmed output |
| Dual-chamber pacemaker (DDDR) | 8–12 years | 3–6 months | Atrial and ventricular pacing percentage; AF burden; sensor usage |
| His-bundle / LBBAP pacemaker | 7–10 years (variable, data emerging) | 3–6 months | Capture thresholds; may be higher than conventional RV pacing |
Device replacement (generator change) is a day-procedure performed under local anaesthesia with prophylactic antibiotics. Battery depletion to ERI is confirmed by remote or in-clinic interrogation. Lead integrity should be assessed — abandoned leads may remain if functional and not infected; however, lead revision or addition may be performed concurrently if indicated. Australian hospital-in-the-home programmes may facilitate post-procedure monitoring.
MRI Compatibility
Most modern pacemakers and leads are labelled "MR Conditional" and can safely undergo MRI scanning under specified conditions (typically ≤1.5 Tesla, whole-body SAR ≤2 W/kg, with appropriate programming). Patients must carry their device identification card. At MRI booking, the device must be interrogated and programmed to MRI-safe mode (typically asynchronous pacing, deactivation of tachycardia therapies) by cardiac physiology staff. Post-scan reprogramming to normal parameters is mandatory. This pathway is available at most major Australian imaging centres but may require coordination in regional areas.
Electromagnetic Interference and Patient Education
- Safe: Mobile phones (use contralateral ear), household appliances, security screening arches (walk through, do not linger), modern induction cooktops
- Avoid / Caution: Electrocautery (monopolar — use bipolar if possible), diathermy, MRI (unless MR Conditional and properly programmed), strong magnets, industrial welding equipment
- Medical procedures: Inform all healthcare providers; TENS units may interfere; lithotripsy requires reprogramming; radiotherapy fields should avoid the generator
- Provide Pacemaker ID card at all times; register with manufacturer; ensure ambulance service is aware
Special Populations
Pregnancy
Paediatrics
Elderly (≥75 Years)
Renal Impairment
Immunocompromised
Aboriginal and Torres Strait Islander Health Considerations
📚 References
- 1. Kusumoto FM, Schoenfeld MH, Barrett C, et al. 2018 ACC/AHA/HRS Guideline on the Evaluation and Management of Patients With Bradycardia and Cardiac Conduction Delay: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Rhythm Society. J Am Coll Cardiol. 2019;74(7):e51-e156. doi:10.1016/j.jacc.2018.10.043
- 2. Writing Committee Members, Tchou PJ, Chung MK, et al. 2023 ACC/AHA/ACCP/HRS Guideline for Diagnosis and Management of Atrial Fibrillation: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation. 2024;149(1):e1-e156.
- 3. Epstein AE, DiMarco JP, Ellenbogen KA, et al. 2012 ACCF/AHA/HRS Focused Update Incorporated Into the ACCF/AHA/HRS 2008 Guidelines for Device-Based Therapy of Cardiac Rhythm Abnormalities. J Am Coll Cardiol. 2013;61(3):e6-e75.
- 4. Mond HG, Proclemer A. The 11th World Survey of Cardiac Pacing and Implantable Cardioverter-Defibrillators: Calendar Year 2009 — A World Society of Arrhythmia's Project. Pacing Clin Electrophysiol. 2011;34(8):1013-1027.
- 5. Australian Institute of Health and Welfare. Heart, stroke and vascular disease — Australian facts. AIHW, Canberra; 2023.
- 6. Katzenellenbogen JM, Bond-Smith D, Seth RJ, et al. The contemporary incidence and prevalence of rheumatic fever and rheumatic heart disease in Australia, using linked data. J Am Heart Assoc. 2022;11(14):e025760.
- 7. Remme WJ, Swedberg K. Comprehensive guidelines for the diagnosis and treatment of chronic heart failure. Task Force for the Diagnosis and Treatment of Chronic Heart Failure of the European Society of Cardiology. Eur Heart J. 2001;22(2):1527-1560.
- 8. Australian Commission on Safety and Quality in Health Care (ACSQHC). National Safety and Quality Health Service Standards. 2nd ed. Sydney: ACSQHC; 2021.
- 9. Crossley GH, Boyle A, Vitense H, et al. The CONNECT (Clinical Evaluation of Remote Notification to Reduce Time to Clinical Decision) Trial. J Am Coll Cardiol. 2011;57(10):1181-1189.
- 10. Hindricks G, Taborsky M, Glikson M, et al. Implant-based multiparameter telemonitoring of patients with heart failure (IN-TIME): a randomised controlled trial. Lancet. 2014;384(9943):583-590.
- 11. Boriani G, Da Costa A, Quesada A, et al. Effects of remote monitoring on clinical outcomes and use of healthcare resources in heart failure patients with biventricular defibrillators: results of the MORE-CARE multicentre randomized controlled trial. Eur J Heart Fail. 2017;19(3):416-425.
- 12. RHDAustralia (RHD Australia) and the Australian Government Department of Health and Ageing. The 2020 Australian guideline for prevention, diagnosis and management of acute rheumatic fever and rheumatic heart disease. 3rd ed. Darwin: Menzies School of Health Research; 2020.
- 13. Mulpuru SK, Madhavan M, McLeod CJ, et al. Cardiac Pacemakers: Function, Troubleshooting, and Management: Part 1 of a 2-Part Series. J Am Coll Cardiol. 2017;69(2):189-210.
- 14. Vijayaraman P, Chung MK, Dandamudi G, et al. His Bundle Pacing: JACC Scientific Expert Panel. J Am Coll Cardiol. 2020;75(11):1347-1363.