📋 Key Information Summary
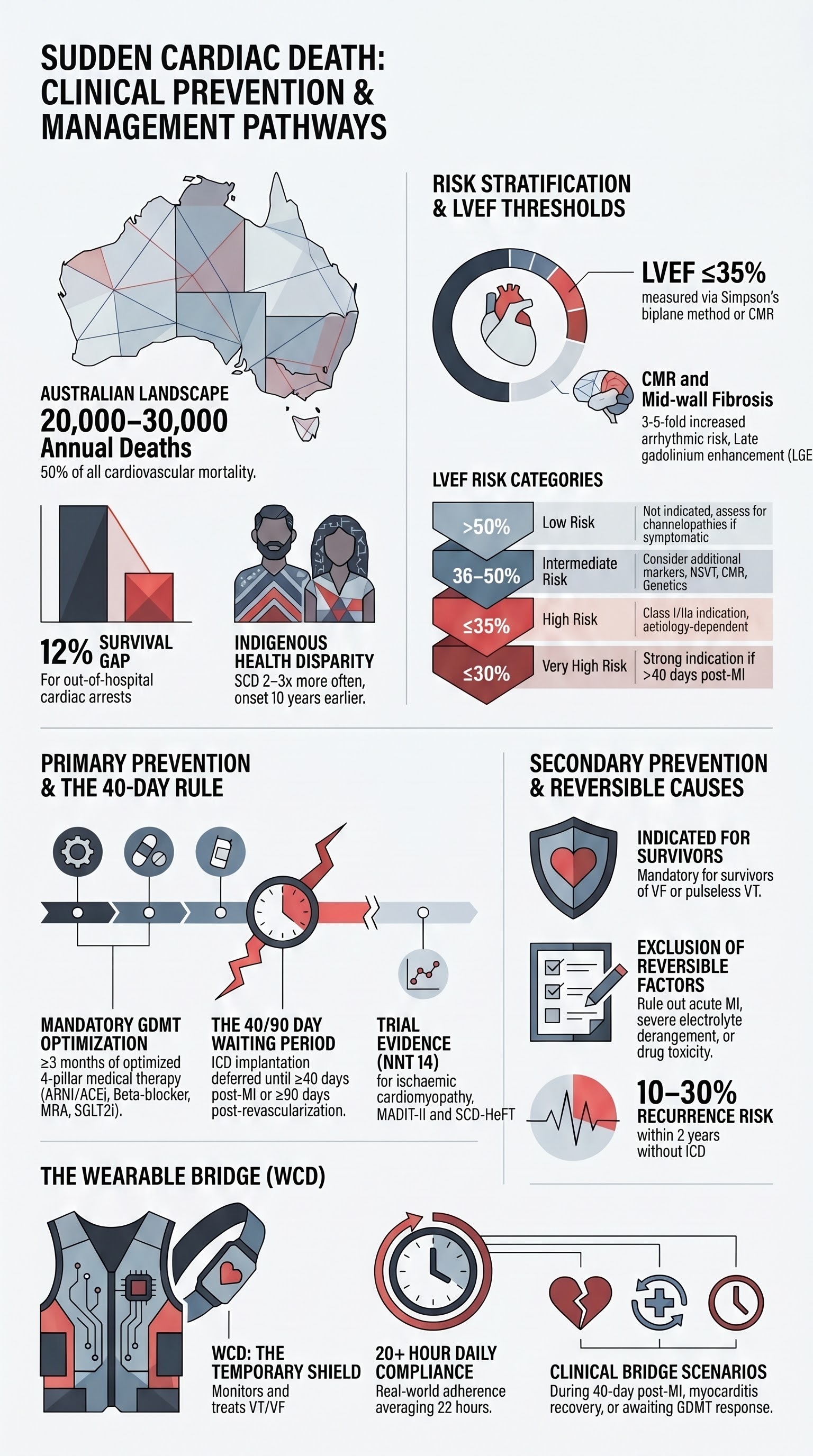
- Sudden cardiac death (SCD) accounts for approximately 20,000–30,000 deaths annually in Australia, representing a major public health burden disproportionately affecting Aboriginal and Torres Strait Islander communities.
- Left ventricular ejection fraction (LVEF) ≤35% remains the single most important criterion for primary prevention implantable cardioverter-defibrillator (ICD) candidacy; measurement should be obtained ≥40 days post-MI and ≥3 months of optimal guideline-directed medical therapy (GDMT).
- For ischaemic cardiomyopathy, the MUSTT and MADIT-II trial data support ICD implantation in patients with LVEF ≤35% and NYHA class II–III symptoms despite ≥3 months of GDMT; SCD-HeFT extended this to NYHA class III.
- Non-ischaemic dilated cardiomyopathy (DCM) with LVEF ≤35% on GDMT qualifies for primary prevention ICD; however, DANISH trial data showed more modest absolute benefit compared with ischaemic aetiology, mandating shared decision-making.
- Hypertrophic cardiomyopathy (HCM) risk stratification uses the ESC HCM Risk-SCD calculator incorporating septal thickness, left atrial size, LVOT gradient, family history of SCD, non-sustained VT, unexplained syncope, and late gadolinium enhancement on CMR.
- Channelopathies (Long QT syndrome, Brugada syndrome, CPVT) require gene-specific and phenotype-specific risk stratification; β-blockers are first-line for LQTS and CPVT; quinidine or catheter ablation for Brugada with recurrent VF storms.
- Secondary prevention ICD is indicated for survivors of cardiac arrest due to VT/VF (excluding reversible causes), and for patients with sustained VT in the setting of structural heart disease or significant LV dysfunction.
- The wearable cardioverter defibrillator (WCD, LifeVest®) serves as a bridge to ICD during the 40-day post-MI window, during myocarditis recovery, and while awaiting LVEF reassessment after ≥3 months of GDMT optimisation.
- All patients being considered for ICD must undergo assessment by a cardiac electrophysiologist; shared decision-making addressing quality of life, deactivation preferences, and device longevity (typically 7–10 years) is mandatory.
- Antiarrhythmic drug therapy (amiodarone, sotalol, dofetilide) may supplement ICD therapy for arrhythmia burden reduction but does not substitute for ICD in SCD prevention.
- GDMT for heart failure (ACEi/ARB/ARNI, β-blocker, MRA, SGLT2 inhibitor) must be optimised before ICD implantation, as LVEF may improve beyond 35%, potentially removing the indication.
- Peri-procedural complications include pneumothorax (1–2%), lead dislodgement (2–5%), inappropriate shocks (up to 20% at 5 years), and infection (1–2%); CRT-D adds complexity and carries higher procedural risk.
Introduction & Australian Epidemiology
Sudden cardiac death (SCD) is defined as an unexpected death from a cardiac cause occurring within one hour of symptom onset (witnessed) or within 24 hours of the person being last seen alive in a normal state of health (unwitnessed). It remains one of the leading causes of mortality in Australia, responsible for an estimated 20,000–30,000 deaths per year — approximately 10–15% of all-cause mortality and roughly 50% of all cardiovascular deaths.
The epidemiology of SCD in Australia is characterised by significant inequities. Aboriginal and Torres Strait Islander peoples experience SCD at 2–3 times the rate of the non-Indigenous population, with onset at a significantly younger age (median age of SCD approximately 10 years younger than non-Indigenous Australians). Geographically, SCD rates are highest in remote and very remote areas, where access to emergency medical services, cardiac catheterisation laboratories, and electrophysiology expertise is limited.
The Australian Institute of Health and Welfare (AIHW) reports that coronary artery disease underlies approximately 75–80% of SCD cases, with the remaining attributable to non-ischaemic cardiomyopathies (10–15%), channelopathies and inherited arrhythmia syndromes (5–10%), and other structural cardiac diseases including valvular heart disease, myocarditis, and congenital heart disease. Of all out-of-hospital cardiac arrests (OHCA) attended by ambulance services across Australia (approximately 30,000 per year), fewer than 12% survive to hospital discharge, underscoring the critical importance of primary prevention strategies.
The National Heart Foundation of Australia and the Cardiac Society of Australia and New Zealand (CSANZ) endorse a systematic approach to SCD risk stratification and ICD therapy aligned with international guidelines from the European Society of Cardiology (ESC, 2022) and the American College of Cardiology/American Heart Association/Heart Rhythm Society (ACC/AHA/HRS, 2017 with 2023 focused updates). Australian practice also reflects Therapeutic Guidelines (Cardiovascular) recommendations and PBS funding arrangements that shape real-world access to device therapy.
This article provides a comprehensive clinical guideline for the prevention of SCD in Australian practice, covering risk assessment methodologies, indications for primary and secondary prevention ICD implantation, the role of the wearable cardioverter defibrillator, and considerations for special populations including Indigenous Australians.
Risk Assessment for Sudden Cardiac Death
Risk stratification for SCD is the cornerstone of prevention, guiding patient selection for ICD therapy. The approach differs fundamentally depending on whether the patient has known structural heart disease or is being evaluated for a primary electrical disease (channelopathy).
Ejection Fraction–Based Criteria
Left ventricular ejection fraction (LVEF) remains the most validated and widely used parameter for SCD risk stratification in patients with structural heart disease. The pivotal trials (MADIT, MUSTT, MADIT-II, SCD-HeFT) all used LVEF thresholds to define high-risk populations.
| LVEF Threshold | Risk Category | Key Trials | ICD Recommendation |
|---|---|---|---|
| >50% | Low risk (if no other risk factors) | — | Not indicated; assess for channelopathies if appropriate |
| 36–50% | Intermediate risk | DANISH post-hoc, MASTER trial | Consider additional risk markers (PVC burden, NSVT, CMR LGE, EPS, genetics) |
| ≤35% | High risk | MADIT-II, SCD-HeFT, DANISH | Class I/IIa indication for primary prevention ICD (aetiology-dependent) |
| ≤30% | Very high risk | MADIT-II subset, DINAMIT | Strong indication if >40 days post-MI and on GDMT |
Non-Ischaemic Dilated Cardiomyopathy
In non-ischaemic dilated cardiomyopathy (NIDCM), the relationship between LVEF and arrhythmic risk is less linear than in ischaemic cardiomyopathy. The DANISH trial (2016) demonstrated that prophylactic ICD in NIDCM reduced sudden cardiac death but did not significantly reduce all-cause mortality over a median 5.6-year follow-up, driven by competing risks of pump-failure death and improved GDMT outcomes.
Additional risk markers in NIDCM that may strengthen ICD candidacy include:
- Mid-wall fibrosis on cardiac MRI (late gadolinium enhancement) — associated with 3–5-fold increased risk of arrhythmic events; this is a particularly strong discriminator in NIDCM
- Non-sustained VT on Holter monitoring (≥3 consecutive beats, rate ≥120 bpm, duration <30 seconds)
- Syncope of undetermined aetiology
- LV end-diastolic diameter >65 mm (indexed >40 mm/m²)
- Genetic testing identifying pathogenic variants in lamin A/C (LMNA), which carries particularly high arrhythmic risk and may warrant ICD even at higher LVEF (36–49%)
Channelopathies and Inherited Arrhythmia Syndromes
Patients with structurally normal hearts may still be at significant SCD risk due to inherited ion channel disorders. Risk stratification is gene-specific and phenotype-specific:
| Channelopathy | Key Risk Factors | First-Line Therapy | ICD Indications |
|---|---|---|---|
| Long QT Syndrome (LQTS) | QTc >500 ms (LQT1/2/3), prior cardiac arrest, syncope on β-blockers, genotype (LQT3 highest risk) | Nadolol (LQT1/2) or propranolol; mexiletine adjunct for LQT3 | Prior CA/VF, recurrent syncope on β-blockers, QTc >550 ms with high-risk features |
| Brugada Syndrome | Spontaneous Type 1 ECG pattern, prior syncope, male sex, SCN5A mutation, VF inducibility on EPS (controversial) | Quinidine (for VF storms); catheter ablation for recurrent VT/VF | Prior CA/VF (Class I); syncope with spontaneous Type 1 (Class IIa); asymptomatic — risk score–guided (SHFM, Appelboom) |
| Catecholaminergic Polymorphic VT (CPVT) | Bidirectional VT on exercise testing, RYR2/CASQ2 mutations, recurrent syncope on β-blockers | Nadolol or propranolol; flecainide adjunct | Prior CA, recurrent VT despite maximal medical therapy, high-risk genotype (RYR2 exon 3 region) |
Family History and Genetic Screening
A family history of SCD (especially first-degree relatives <40 years) is an independent risk modifier. The CSANZ and Heart Foundation recommend:
- Cardiac screening (12-lead ECG, echocardiography, exercise stress test) for all first-degree relatives of SCD victims, ideally through a dedicated inherited cardiac disease clinic
- Genetic counselling and targeted genetic testing when a channelopathy or cardiomyopathy is suspected (MBS item 73287 for genetic consultation in select states; panel-based next-generation sequencing available at major Australian centres including Royal Melbourne, Royal Prince Alfred, Westmead, and the Victor Chang Cardiac Research Institute)
- Cascade screening of family members when a pathogenic variant is identified
- Comprehensive post-mortem evaluation (including genetic autopsy/molecular autopsy) for all sudden unexplained deaths, particularly in those aged 1–40 years, coordinated through state coronial services and the Australian National SUDI/SIDS Register
Electrophysiology Study and Additional Risk Markers
Invasive electrophysiology study (EPS) with programmed ventricular stimulation may be considered in selected patients (particularly ischaemic cardiomyopathy with LVEF 36–49%) to refine risk stratification. Sustained monomorphic VT inducibility predicts higher arrhythmic event rates and may strengthen ICD candidacy. Non-invasive risk markers with emerging evidence include:
- Fragmented QRS on 12-lead ECG
- T-wave alternans (MTWA) — negative predictive value is high but positive predictive value is modest
- Heart rate variability (HRV) and heart rate turbulence
- Quantification of myocardial scar burden on CMR (LGE mass, % total LV mass)
- Speckle tracking echocardiography — global longitudinal strain (GLS) as a complementary parameter to LVEF
Primary Prevention ICD Therapy
Primary prevention ICD therapy is indicated for patients at high risk of SCD who have not yet experienced a life-threatening arrhythmic event. Selection requires a multi-factorial approach combining LVEF assessment, clinical status, aetiology of cardiomyopathy, and guideline-directed medical therapy (GDMT) optimisation.
Ischaemic Cardiomyopathy — Primary Prevention
Ischaemic cardiomyopathy is the most common indication for primary prevention ICD worldwide. The evidence base is the most robust among all aetiologies.
Non-Ischaemic Dilated Cardiomyopathy — Primary Prevention
For non-ischaemic dilated cardiomyopathy, the indication for primary prevention ICD requires LVEF ≤35% despite ≥3 months of GDMT, NYHA class II–III symptoms, and expected survival >1 year. The strength of recommendation is tempered by the DANISH trial results.
Factors strengthening ICD candidacy in NIDCM:
- Mid-wall LGE on CMR (strongest independent predictor — HR ~4.5 for arrhythmic death)
- LMNA pathogenic variant with ≥2 additional risk factors (non-sustained VT, LVEF <45%, male sex, missense mutation, age of onset <40)
- Syncope of undetermined aetiology
- Young age (<60 years) with preserved functional capacity
Hypertrophic Cardiomyopathy — Risk Stratification and ICD
HCM carries an annual SCD risk of approximately 0.5–1.0%, with higher rates in children and adolescents. The ESC 2020 guidelines recommend the HCM Risk-SCD calculator (https://www.doc2000.com/hcm) to estimate 5-year SCD risk, which integrates seven variables:
| Risk Factor | Hazard Ratio | Assessment |
|---|---|---|
| Age at evaluation | Inverse relationship | Clinical assessment |
| Maximal LV wall thickness | 1.04 per mm | Echocardiography or CMR |
| Left atrial diameter | 1.06 per mm | Echocardiography |
| Maximal LVOT gradient at rest/Valsalva | 1.01 per mmHg | Echocardiography with provocative manoeuvres |
| Family history of SCD | 1.96 | First-degree relative <40 years |
| Non-sustained VT on Holter | 2.19 | 48-hour Holter monitoring (≥3 beats, ≥120 bpm) |
| Unexplained syncope | 2.13 | Clinical history; exclude vasovagal, orthostatic |
ICD recommendations in HCM:
- Class I: Prior cardiac arrest or sustained VT; 5-year SCD risk ≥6% (HCM Risk-SCD calculator)
- Class IIa: 5-year SCD risk 4–6% with additional risk factors (extensive LGE, LV apical aneurysm, LVEF <50%)
- Class IIb: 5-year SCD risk <4% but ≥1 major conventional risk factor (NSVT, syncope, wall thickness ≥30 mm, family history, LA >45 mm)
Antiarrhythmic Drug Considerations
Antiarrhythmic drugs do not substitute for ICD in SCD prevention but may be used adjunctively:
GDMT Optimisation Before ICD Consideration
Before ICD implantation, GDMT for heart failure must be maximised for ≥3 months. LVEF reassessment after optimisation is mandatory, as a significant proportion of patients (25–40%) will demonstrate LVEF improvement to >35%, potentially obviating the need for a primary prevention ICD. The four pillars of GDMT are:
Secondary Prevention ICD Therapy
Secondary prevention ICD therapy is indicated for patients who have survived a cardiac arrest or experienced sustained ventricular tachycardia (VT) in the context of structural heart disease, where the arrhythmia is not due to a completely reversible cause. The evidence base (AVID, CIDS, CASH trials) demonstrates a significant mortality reduction compared with antiarrhythmic drug therapy alone.
Indications
Exclusion of Reversible Causes
Before implanting a secondary prevention ICD, a systematic evaluation for reversible or treatable causes of VT/VF must be completed:
- Acute myocardial infarction (within 48 hours): VT/VF occurring in the setting of acute STEMI/NSTEMI and treated with timely revascularisation may not require ICD if LVEF recovers
- Electrolyte derangement: Severe hypokalaemia (<3.0 mmol/L), hypomagnesaemia (<0.5 mmol/L), hyperkalaemia (>6.5 mmol/L)
- Drug/toxin-induced: Cocaine, methamphetamine, tricyclic antidepressant overdose, antipsychotic-induced QT prolongation
- Brugada pattern due to fever: Fever-induced Type 1 pattern resolving with antipyretic therapy (though cardiology follow-up is warranted)
Catheter Ablation as Adjunct
Catheter ablation for VT should be considered in patients with recurrent VT episodes despite antiarrhythmic drugs, particularly in ischaemic cardiomyopathy where substrate-based ablation targeting the scar border zone has the strongest evidence (VTACH, VANISH trials). In Australia, VT ablation is available at major tertiary centres (Royal Melbourne, Royal Prince Alfred, Westmead, Flinders, Royal Adelaide, Princess Alexandra, Sir Charles Gairdner) and is MBS-reimbursed under item 38250 (catheter ablation of cardiac arrhythmia). Ablation should not delay ICD implantation in secondary prevention patients.
Post-Implantation Antiarrhythmic Drug Therapy
Many secondary prevention patients require ongoing antiarrhythmic drug therapy to reduce VT burden and ICD shocks:
- Amiodarone is the most effective agent for VT suppression; reduces appropriate and inappropriate ICD shocks; requires organ monitoring (TFTs, LFTs, PFTs, ophthalmology annually)
- Sotalol may be used as an alternative (class III + β-blocker effect); must be initiated in hospital with cardiac monitoring; less effective than amiodarone for VT
- Mexiletine (available through Special Access Scheme in Australia) may be added to amiodarone for refractory VT
- β-blockers alone are appropriate for patients with infrequent arrhythmia and ICD in situ
Wearable Cardioverter Defibrillator (WCD)
The wearable cardioverter defibrillator (WCD; LifeVest®, ZOLL Medical) is a vest-worn device that continuously monitors cardiac rhythm and delivers defibrillation therapy (typically 75–150 J biphasic) for detected VT/VF. It serves as a temporary external defibrillation bridge during clinical windows when a patient is at high SCD risk but an ICD is either contraindicated or premature.
Indications for WCD Use
Practical Considerations in Australia
- Availability: The WCD (LifeVest) is available in Australia through ZOLL Medical Australia. It is prescribed via specialist cardiology/electrophysiology clinics and typically funded through a combination of private health insurance, hospital funding, and patient co-payment. There is currently no dedicated PBS or MBS listing for WCD.
- Wear time: Patients should aim for ≥20 hours/day of continuous wear; compliance monitoring is built into the device software and reported to the prescribing physician. Real-world adherence averages 22 hours/day in motivated patients.
- Contraindications: Inability to wear the vest (severe skin disease, extreme body habitus outside available sizes), lack of cognitive capacity to respond to alarms, patients already in hospital with continuous cardiac monitoring
- Alert fatigue: Non-sustained VT and artefact can trigger alarms, causing patient anxiety. Education regarding alarm management is essential. Reassurance that not all alarms indicate a life-threatening event is important.
LVEF Reassessment Pathway
After the WCD bridge period, patients must undergo systematic reassessment:
| LVEF on Reassessment | Action | Rationale |
|---|---|---|
| Remains ≤35% | Proceed to primary prevention ICD implantation | Persistent high-risk profile; WCD bridge complete |
| Improved to 36–49% | Electrophysiology review; consider CMR (LGE), EPS, Holter; risk-stratify further | Intermediate risk — additional markers needed |
| Recovered to ≥50% | Continue GDMT; serial echo (3–6-monthly initially); ICD not indicated | Low arrhythmic risk; monitor for relapse (especially if non-ischaemic, peripartum, myocarditis) |
Special Populations
Pregnancy
Paediatrics
Elderly (>75 years)
Chronic Kidney Disease
Immunocompromised
Aboriginal and Torres Strait Islander Health Considerations
Aboriginal and Torres Strait Islander peoples experience disproportionately high rates of SCD, with onset at a younger age and significantly worse outcomes from out-of-hospital cardiac arrest. The AIHW reports cardiovascular disease as the leading cause of the health gap between Indigenous and non-Indigenous Australians, contributing to approximately 20% of the life expectancy gap. SCD prevention must be contextualised within a holistic health framework that acknowledges the social determinants of health, cultural safety, and the chronic under-resourcing of remote and regional cardiac services.
📚 References
- 1. Bardy GH, Lee KL, Mark DB, et al. Amiodarone or an implantable cardioverter-defibrillator for congestive heart failure. N Engl J Med. 2005;352(3):225-237. doi:10.1056/NEJMoa043399
- 2. Moss AJ, Zareba W, Hall WJ, et al. Prophylactic implantation of a defibrillator in patients with myocardial infarction and reduced ejection fraction. N Engl J Med. 2002;346(12):877-883. doi:10.1056/NEJMoa013474
- 3. Køber L, Thune JJ, Nielsen JC, et al. Defibrillator implantation in patients with nonischemic systolic heart failure. N Engl J Med. 2016;375(13):1221-1230. doi:10.1056/NEJMoa1608029
- 4. The Antiarrhythmics versus Implantable Defibrillators (AVID) Investigators. A comparison of antiarrhythmic-drug therapy with implantable defibrillators in patients resuscitated from near-fatal ventricular arrhythmias. N Engl J Med. 1997;337(22):1576-1583. doi:10.1056/NEJM199711273372202
- 5. Ommen SR, Mital S, Burke MA, et al. 2020 AHA/ACC guideline for the diagnosis and treatment of patients with hypertrophic cardiomyopathy. J Am Coll Cardiol. 2020;76(25):e159-e240. doi:10.1016/j.jacc.2020.08.045
- 6. Zeppenfeld K, Tfelt-Hansen J, de Riva M, et al. 2022 ESC guidelines for the management of patients with ventricular arrhythmias and the prevention of sudden cardiac death. Eur Heart J. 2022;43(40):3997-4126. doi:10.1093/eurheartj/ehac262
- 7. Olgin JE, Pletcher MJ, Vittinghoff E, et al. Wearable cardioverter-defibrillator after myocardial infarction. N Engl J Med. 2018;379(13):1205-1215. doi:10.1056/NEJMoa1800781
- 8. Priori SG, Wilde AA, Horie M, et al. HRS/EHRA/APHRS expert consensus statement on the diagnosis and management of patients with inherited primary arrhythmia syndromes. Heart Rhythm. 2013;10(12):1932-1963. doi:10.1016/j.hrthm.2013.05.014
- 9. Halliday BP, Gulati A, Ali A, et al. Association between midwall late gadolinium enhancement and sudden cardiac death in patients with dilated cardiomyopathy and mild and moderate left ventricular systolic dysfunction. Circulation. 2017;135(22):2106-2115. doi:10.1161/CIRCULATIONAHA.116.026910
- 10. Connolly SJ, Gent M, Roberts RS, et al. Canadian implantable defibrillator study (CIDS): a randomized trial of the implantable cardioverter defibrillator against amiodarone. Circulation. 2000;101(11):1297-1302. doi:10.1161/01.CIR.101.11.1297
- 11. Kuck KH, Cappato R, Siebels J, Rüppel R. Randomized comparison of antiarrhythmic drug therapy with implantable defibrillators in patients resuscitated from cardiac arrest: the Cardiac Arrest Study Hamburg (CASH). Circulation. 2000;102(7):748-754. doi:10.1161/01.CIR.102.7.748
- 12. Australian Institute of Health and Welfare. Cardiovascular disease in Aboriginal and Torres Strait Islander people. AIHW; 2023. Cat. no. CVD 89.
- 13. National Heart Foundation of Australia and Cardiac Society of Australia and New Zealand. Guidelines for the prevention, detection, and management of heart failure in Australia 2018. Heart Lung Circ. 2018;27(10):1123-1208. doi:10.1016/j.hlc.2018.06.1042
- 14. RHDAustralia (ARF/RHD writing group). The 2020 Australian guideline for prevention, diagnosis, and management of acute rheumatic fever and rheumatic heart disease. 3rd ed. Menzies School of Health Research; 2020.
- 15. Kadish A, Dyer A, Daubert JP, et al. Prophylactic defibrillator implantation in patients with nonischemic dilated cardiomyopathy. N Engl J Med. 2004;350(21):2151-2158. doi:10.1056/NEJMoa033088
- 16. Hohnloser SH, Kuck KH, Dorian P, et al. Prophylactic use of an implantable cardioverter-defibrillator after acute myocardial infarction. N Engl J Med. 2004;351(24):2481-2488. doi:10.1056/NEJMoa041489
- 17. Steinberg JS, Beckles MI, Socoteanu M, et al. Usefulness of the wearable cardioverter defibrillator in bridging the ICD waiting period. Circ Arrhythm Electrophysiol. 2019;12(6):e007208.
- 18. Connolly SJ, Hallstrom AP, Cappato R, et al. Meta-analysis of the implantable cardioverter defibrillator secondary prevention trials. Eur Heart J. 2000;21(24):2071-2078. doi:10.1053/euhj.2000.2476