📋 Key Information Summary
- Infective endocarditis (IE) carries a mortality of 15–30% even with optimal treatment; early diagnosis and multidisciplinary management are critical.
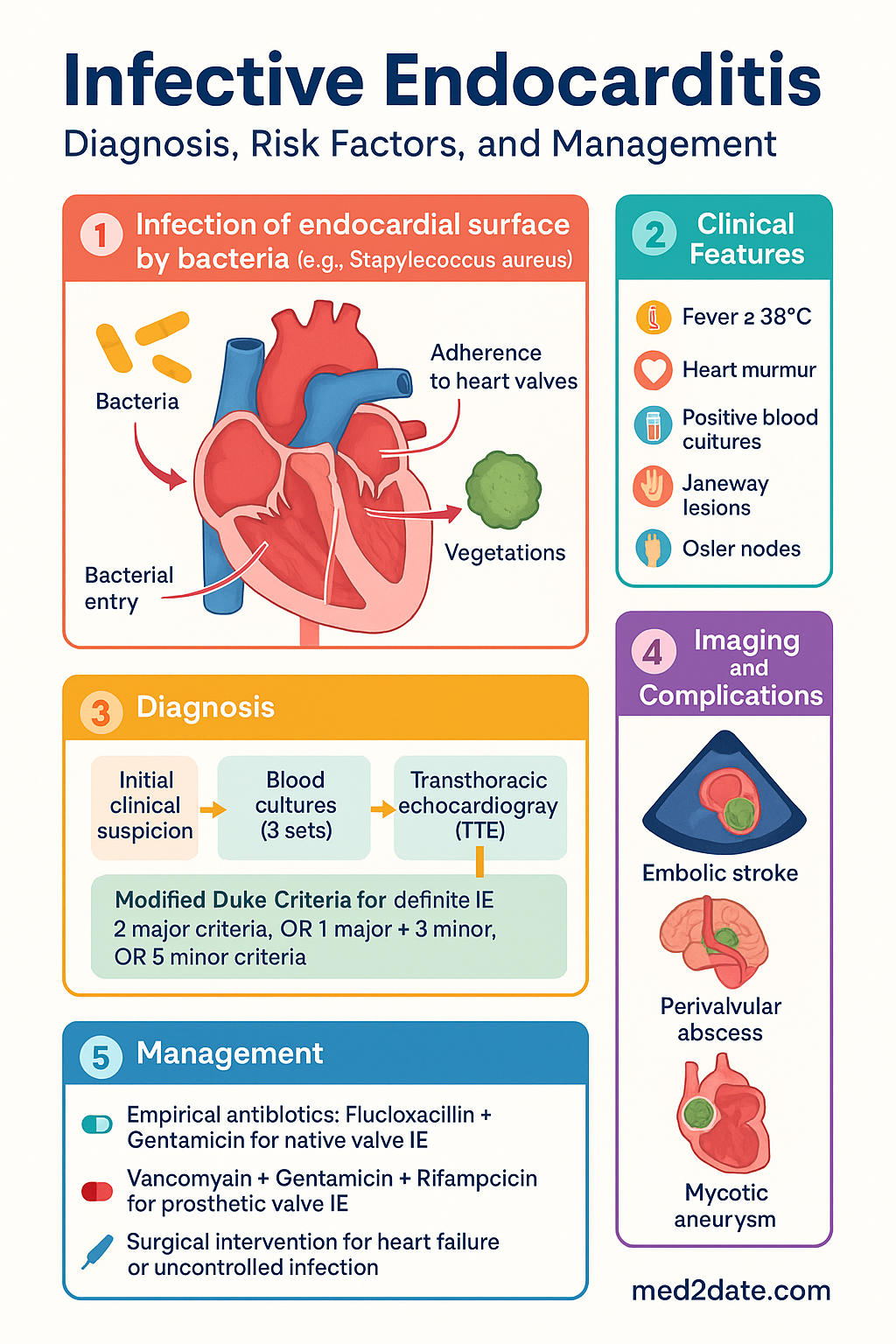
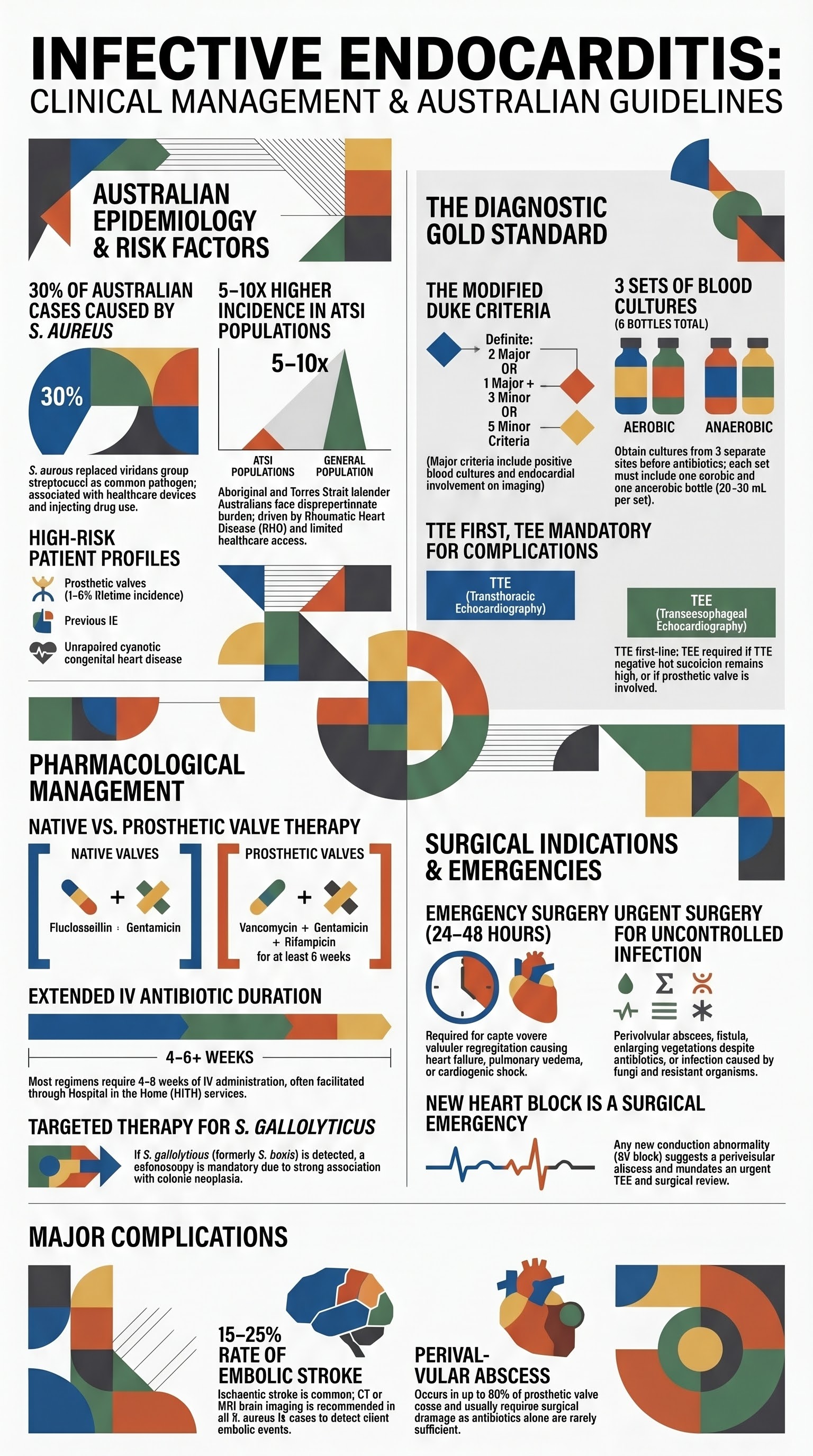
- The modified Duke criteria remain the gold standard for diagnosis, classifying cases as definite or possible IE based on pathological, major, and minor criteria.
- Three sets of blood cultures from separate venepuncture sites must be obtained before empirical antibiotics; each set includes an aerobic and anaerobic bottle.
- Transthoracic echocardiography (TTE) is the first-line imaging; transoesophageal echocardiography (TEE) is mandatory if TTE is negative, if prosthetic valve IE is suspected, or if complications are suspected.
- Staphylococcus aureus is the most common cause in Australia (≈30% of cases), including community-associated methicillin-resistant S. aureus (CA-MRSA) in Aboriginal and Torres Strait Islander communities.
- Empirical therapy for native valve IE is flucloxacillin + gentamicin; prosthetic valve IE requires vancomycin + gentamicin + rifampicin pending culture results.
- Antibiotic durations are typically 4–6 weeks for native valve IE and ≥6 weeks for prosthetic valve IE, administered IV for the full course.
- Surgical indications include heart failure from valvular dysfunction, uncontrolled infection (abscess, fistula, persistently positive cultures), recurrent embolic events with large vegetations, and prosthetic valve IE with complications.
- Major complications include perivalvular abscess, conduction abnormalities (new heart block warrants urgent TEE), embolic stroke, mycotic aneurysm, and renal failure.
- Antibiotic prophylaxis is recommended before dental and certain invasive procedures in patients with prosthetic valves, previous IE, or congenital heart disease with residual defects.
- Aboriginal and Torres Strait Islander peoples have a significantly higher incidence of IE due to rheumatic heart disease, higher rates of CA-MRSA, and barriers to healthcare access in remote communities.
- All cases should be discussed with an endocarditis team comprising cardiology, cardiothoracic surgery, infectious diseases, and microbiology at the earliest opportunity.
Introduction & Australian Epidemiology
Infective endocarditis (IE) is a life-threatening infection of the endocardial surface of the heart, most commonly involving the heart valves. Despite advances in diagnosis and treatment, IE remains associated with significant morbidity and mortality, with in-hospital mortality rates of 15–30% and 5-year mortality approaching 40%.
In Australia, the estimated incidence of IE is approximately 3–7 per 100,000 population per year, though this is likely an underestimate. The epidemiology has shifted over recent decades: Staphylococcus aureus has replaced viridans group streptococci as the leading cause, healthcare-associated IE has increased, and there is a persistent burden among people who inject drugs (PWID) and those with rheumatic heart disease (RHD).
Key Australian trends include:
- Healthcare-associated IE: Increasing proportion of cases related to indwelling intravascular devices, haemodialysis access, and nosocomial bacteraemia.
- Injecting drug use: Right-sided (tricuspid valve) IE is the predominant pattern, most commonly caused by S. aureus.
- Prosthetic valve IE: Accounts for 10–30% of all IE cases; early (within 12 months of surgery) and late (>12 months) forms have distinct microbiological profiles.
- Rheumatic heart disease: Remains a significant risk factor in Indigenous Australians, particularly in the Northern Territory and Western Australia.
- Ageing population: Degenerative valvular disease in older Australians increases susceptibility, with a median age at diagnosis now exceeding 60 years.
| Risk Factor | Comment |
|---|---|
| Prosthetic heart valve | Highest risk; 1–6% lifetime incidence |
| Previous infective endocarditis | Recurrence rate 2–6% per patient-year |
| Rheumatic heart disease | Significant burden in ATSI populations |
| Congenital heart disease | Particularly unrepaired cyanotic lesions |
| Injecting drug use | Right-sided IE, typically S. aureus |
| Indwelling intravascular devices | Central lines, ports, pacemakers |
| Haemodialysis | AV fistula or catheter-related |
| Immunosuppression | Transplant recipients, HIV (low CD4) |
| Poor dental health | Periodontitis as portal of entry for oral streptococci |
Diagnosis
Modified Duke Criteria
The modified Duke criteria remain the cornerstone of IE diagnosis. They stratify patients into definite, possible, or rejected IE based on major and minor clinical criteria. Pathological criteria (histology or culture of excised tissue or embolic material) provide definitive diagnosis.
| Criterion Type | Criteria |
|---|---|
| Major — Blood cultures | 1. Typical organism from ≥2 separate blood cultures: S. aureus, viridans group streptococci, S. gallolyticus (formerly S. bovis), HACEK group, or community-acquired Enterococcus spp. with no primary focus 2. Persistently positive blood cultures: ≥2 positive cultures drawn >12 h apart, or all of 3 or majority of ≥4 separate cultures positive |
| Major — Endocardial involvement | 1. Echocardiographic findings: oscillating intracardiac mass on a valve or supporting structure, in the path of regurgitant jets, or on implanted material (in the absence of alternative explanation); perivalvular abscess; new partial dehiscence of a prosthetic valve 2. New valvular regurgitation (worsening or changing of pre-existing murmur not sufficient) |
| Minor criteria | 1. Predisposing heart condition or intravenous drug use 2. Fever ≥38°C 3. Vascular phenomena: major arterial emboli, septic pulmonary infarcts, mycotic aneurysm, intracranial haemorrhage, conjunctival haemorrhage, Janeway lesions 4. Immunological phenomena: glomerulonephritis, Osler nodes, Roth spots, positive rheumatoid factor 5. Microbiological evidence not meeting major criteria (single positive culture of an atypical organism, or serological evidence of active infection) |
Blood Culture Protocol
Blood cultures are the single most important microbiological investigation and must be collected before any antibiotic therapy is initiated.
Echocardiography
| Modality | Sensitivity | Indications | Limitations |
|---|---|---|---|
| Transthoracic echocardiography (TTE) | 50–60% for vegetations overall; ~90% for native valve vegetations >5 mm | First-line investigation in all suspected IE | Poor sensitivity for prosthetic valve IE, small vegetations (<5 mm), perivalvular abscess; limited by body habitus and lung disease |
| Transoesophageal echocardiography (TEE) | 90–95% overall; superior for prosthetic valve and complications | Negative or inconclusive TTE with high clinical suspicion; suspected prosthetic valve IE; suspected complications (abscess, fistula); S. aureus bacteraemia; persistently positive blood cultures | Semi-invasive; requires sedation or GA; small risk of oesophageal perforation |
Additional Imaging
- 18F-FDG PET/CT: Increasingly used for prosthetic valve IE diagnosis (added as a major criterion in the 2023 ESC guidelines) and detection of embolic events. Useful for diagnosis of prosthetic valve IE when echo is inconclusive. Availability is limited to major metropolitan centres.
- Gallium-67 or labelled white cell scanning: May be considered for cardiac device infection where PET/CT is unavailable.
- CT brain (± CT angiography): Recommended in all patients with S. aureus IE to detect silent embolic events or mycotic aneurysms.
- CT chest: Septic pulmonary emboli (especially in right-sided IE); may show peripheral wedge-shaped nodular opacities with cavitation.
- CT abdomen/pelvis: Assess for splenic infarction, renal infarction, mycotic aneurysms, spondylodiscitis.
- MRI brain: Superior to CT for detection of cerebral microabscesses, septic emboli, and mycotic aneurysms. Perform if neurological symptoms or signs are present.
- Cardiac CT (ECG-gated): Valuable for assessing perivalvular anatomy, abscess, and pseudoaneurysm, especially in prosthetic valve IE where echocardiographic windows are poor.
Microbiology & Antibiotic Therapy
Common Causative Organisms
| Organism | Frequency | Typical Setting | Key Points |
|---|---|---|---|
| Staphylococcus aureus | 30–40% | Healthcare-associated, PWID, community | Most common cause overall; aggressive course; high embolic risk. MRSA prevalent in ATSI communities and hospital-acquired cases. |
| Viridans group streptococci | 15–25% | Community-acquired, dental source | Oral flora; usually penicillin-susceptible; associated with subacute presentation. Includes S. sanguinis, S. mutans, S. mitis/oralis. |
| Streptococcus gallolyticus (formerly S. bovis) | 5–10% | GI source | Strong association with colonic neoplasia; colonoscopy is mandatory in all cases. |
| Enterococcus spp. | 5–10% | Healthcare-associated, GU source, elderly | Usually E. faecalis; often requires combination therapy (ampicillin + gentamicin or ceftriaxone). E. faecium may be ampicillin-resistant — vancomycin required. |
| HACEK group | 2–5% | Community-acquired, oral source | Haemophilus, Aggregatibacter, Cardiobacterium, Eikenella, Kingella. Slow-growing; extended incubation needed. Usually β-lactamase negative — ceftriaxone is the treatment of choice. |
| Coagulase-negative staphylococci | 5–10% | Prosthetic valve IE (especially S. epidermidis) | Most common cause of prosthetic valve IE; often methicillin-resistant. Rifampicin is added for prosthetic valve infections. |
| Fungi (Candida, Aspergillus) | <2% | Prosthetic valve, immunocompromised, PWID | Very high mortality (>50%); almost always requires surgical intervention. Blood cultures often negative — consider fungal serology and beta-D-glucan. |
Culture-Negative Infective Endocarditis
Culture-negative IE accounts for 5–15% of cases in Australia. Causes include prior antibiotic exposure (most common), fastidious organisms, and non-infectious mimics.
- Prior antibiotic use: Most common cause; may need to cease antibiotics and re-culture after a washout period if clinically safe.
- Fastidious organisms: HACEK group (extend incubation to 14–21 days), Coxiella burnetii (Q fever — serology), Bartonella spp. (serology and PCR), Tropheryma whipplei (PCR, small bowel biopsy), Brucella spp. (serology, extended incubation).
- Q fever endocarditis: Australia is endemic for Q fever; Coxiella burnetii serology (phase I IgG >1:800) should be sent in all culture-negative IE cases. Treatment is doxycycline + hydroxychloroquine.
- Molecular diagnostics: 16S rRNA PCR on excised valve tissue or embolic material; broad-range PCR on blood may assist.
Empirical Antibiotic Therapy
Empirical Regimens
| Clinical Scenario | Empirical Regimen | Duration |
|---|---|---|
| Native valve — community-acquired | Flucloxacillin 2 g IV 4-hourly + Gentamicin 1 mg/kg IV 8-hourly | Pending culture; adjust to targeted regimen |
| Native valve — suspected MRSA or penicillin allergy (anaphylaxis) | Vancomycin 15–20 mg/kg IV 8–12-hourly (AUC-guided) | Pending culture; may add gentamicin for synergy |
| Prosthetic valve IE (any timing) | Vancomycin 15–20 mg/kg IV 8–12-hourly + Gentamicin 1 mg/kg IV 8-hourly + Rifampicin 300–450 mg PO/IV 12-hourly | Pending culture; ≥6 weeks for staphylococcal PVE |
| Suspected enterococcal IE | Ampicillin 2 g IV 4-hourly + Gentamicin 1 mg/kg IV 8-hourly | 4–6 weeks |
| Injecting drug use (right-sided) | Flucloxacillin 2 g IV 4-hourly ± Gentamicin 1 mg/kg IV 8-hourly | 2 weeks (if S. aureus MSSA, right-sided only, no complications — short-course possible); otherwise 4–6 weeks |
Directed Therapy by Organism — Summary
| Organism | First-Line Regimen | Duration (Native Valve) | Duration (Prosthetic Valve) |
|---|---|---|---|
| S. aureus (MSSA) | Flucloxacillin 2 g IV 4-hourly ± Gentamicin 1 mg/kg IV 8-hourly (first 2 weeks for synergy) | 4–6 weeks | ≥6 weeks + rifampicin |
| S. aureus (MRSA) | Vancomycin (AUC-guided) ± Gentamicin; or Daptomycin 8–10 mg/kg IV daily | 6 weeks | ≥6 weeks + rifampicin |
| Viridans streptococci (Pen MIC ≤0.12 mg/L) | Benzylpenicillin 1.8–2.4 g IV 4-hourly ± Gentamicin (first 2 weeks) | 4 weeks | 6 weeks |
| Viridans streptococci (Pen MIC 0.25–2 mg/L) | Benzylpenicillin 2.4 g IV 4-hourly + Gentamicin (2 weeks) | 4 weeks | 6 weeks |
| E. faecalis (Pen-susceptible) | Ampicillin 2 g IV 4-hourly + Gentamicin 1 mg/kg IV 8-hourly; OR Ampicillin + Ceftriaxone (if aminoglycoside contraindicated) | 4–6 weeks | ≥6 weeks |
| E. faecium (ampicillin-resistant) | Vancomycin + Gentamicin; consult ID for linezolid or daptomycin if VRE | 6 weeks | ≥6 weeks |
| HACEK group | Ceftriaxone 2 g IV once daily | 4 weeks | 6 weeks |
| CoNS (prosthetic valve) | Vancomycin + Rifampicin 300 mg PO 12-hourly + Gentamicin (first 2 weeks) | N/A | ≥6 weeks |
| Coxiella burnetii | Doxycycline 100 mg PO BD + Hydroxychloroquine 200 mg PO TDS | ≥18 months (lifelong in some cases) | ≥18 months |
| Candida spp. | Liposomal amphotericin B ± flucytosine; step down to fluconazole (lifelong suppressive if not surgically excised) | Lifelong suppression if valve retained | Lifelong suppression |
Surgical Indications
Surgery is required in approximately 40–50% of IE cases during the index admission. An endocarditis team (cardiologist, cardiothoracic surgeon, infectious diseases physician, microbiologist, neurologist, and imaging specialist) should discuss all cases early. Urgent surgery (within 48 hours) may be lifesaving.
Indications for Surgery
Relative Indications for Surgery
- Staphylococcal prosthetic valve IE (frequently requires surgery)
- Fungal IE (almost always requires surgery)
- Left-sided IE with large vegetations (>10 mm) and significant valvular dysfunction
- Conduction abnormalities suggesting perivalvular extension (new AV block)
- Relapse after completion of appropriate antibiotic therapy
- Persistent fever >10 days without alternative explanation
Contraindications to Surgery
- Severe irreversible neurological deficit (discuss with neurology — moderate stroke may still proceed to surgery after 1–2 weeks if haemorrhagic transformation excluded)
- Severe comorbidities with unacceptably high operative risk
- Severe septic shock unresponsive to resuscitation (relative)
Complications
Complications of IE are a major driver of morbidity and mortality. They may arise from direct infection spread (local), embolic phenomena (systemic), immune-mediated processes, or treatment toxicity.
Perivalvular Abscess
- Occurs in 10–40% of native valve IE and up to 60% of prosthetic valve IE.
- Most common in the aortic annulus (mitro-aortic intervalvular fibrosa region).
- Clinical clue: New AV conduction abnormalities (first-degree AV block, bundle branch block, complete heart block), persistent fever on appropriate antibiotics, or persistent bacteraemia.
- Diagnosis: TEE is the investigation of choice (sensitivity >85%). CT cardiac (ECG-gated) is a valuable adjunct. TTE has limited sensitivity for abscess.
- Management: Almost always requires surgical drainage and debridement. Antibiotics alone rarely sufficient. New heart block in the setting of IE should be treated as perivalvular abscess until proven otherwise.
Conduction Abnormalities
- New PR prolongation, bundle branch block, or complete heart block occurs in 5–15% of cases.
- Strongly associated with perivalvular abscess (aortic valve IE > mitral valve IE).
- Any new conduction abnormality mandates urgent TEE and cardiothoracic surgical review.
- Temporary pacing may be required; permanent pacemaker implantation may be needed if conduction does not recover after surgical debridement.
Embolic Events
| Embolic Site | Frequency | Clinical Features | Management |
|---|---|---|---|
| Cerebral (ischaemic stroke) | 15–25% | Focal neurological deficit; may be clinically silent on imaging in up to 50% of S. aureus IE | CT brain ± MRI; anticoagulation generally NOT recommended for ischaemic stroke in IE; discuss neurology; surgery timing may be delayed 2–4 weeks if large infarct |
| Cerebral (haemorrhagic) | 3–5% | Headache, altered consciousness, focal deficit; may occur as complication of anticoagulation or mycotic aneurysm rupture | CT brain urgently; hold anticoagulation; neurosurgical review; contraindication to cardiopulmonary bypass |
| Splenic infarction/abscess | 10–40% (subclinical) | Left upper quadrant pain, fever; CT shows peripheral wedge defects or abscess | Most resolve with antibiotics; splenic abscess may require percutaneous drainage or splenectomy |
| Renal infarction | 10–30% | Flank pain, haematuria, rising creatinine | Supportive care; also consider immune-complex glomerulonephritis and drug-induced nephrotoxicity |
| Septic pulmonary emboli | Common in right-sided IE (PWID) | Dyspnoea, pleuritic chest pain, haemoptysis; CT chest shows peripheral nodular infiltrates with cavitation | Antibiotics; rarely requires surgical intervention |
| Spondylodiscitis / Vertebral osteomyelitis | 3–15% | Back pain, fever; MRI spine is the investigation of choice | Prolonged antibiotic course (≥6 weeks total from IE start); may require surgical debridement |
| Peripheral arterial emboli | 5–15% | Acute limb ischaemia (pain, pallor, pulselessness); may present with Osler nodes, Janeway lesions | Vascular surgery review; embolectomy if critical ischaemia |
Mycotic Aneurysm
- Result from septic emboli lodging in the vasa vasorum or direct arterial wall infection.
- Most common sites: intracranial (especially middle cerebral artery bifurcation), aorta, visceral arteries, and peripheral arteries.
- Diagnosis: CT angiography or MR angiography. Conventional angiography if endovascular intervention planned.
- Management: Prolonged IV antibiotics; surgical or endovascular intervention for rupture, expansion, or failure to respond to medical therapy. Neurosurgical intervention for intracranial mycotic aneurysms (clipping or coiling).
- Aneurysm surveillance: Repeat imaging at intervals to assess for expansion or new aneurysm formation.
Other Complications
- Heart failure: May be acute (valvular regurgitation) or chronic; echocardiographic monitoring is essential.
- Renal failure: Multifactorial — embolic, immune-complex glomerulonephritis, drug toxicity (vancomycin, gentamicin). Monitor renal function closely.
- Drug fever / hypersensitivity: Diagnosis of exclusion; do not prematurely discontinue antibiotics without infectious diseases input.
Prophylaxis & Prevention
Australian guidelines (aligned with the American Heart Association 2007 update and endorsed by the Cardiac Society of Australia and New Zealand) recommend antibiotic prophylaxis before dental and certain invasive procedures in patients at highest risk of adverse outcomes from IE.
High-Risk Conditions Requiring Prophylaxis
- Prosthetic heart valve or prosthetic material used for valve repair
- Previous infective endocarditis
- Congenital heart disease: unrepaired cyanotic CHD, completely repaired CHD with prosthetic material within the first 6 months, repaired CHD with residual defects at or near the site of a prosthetic patch
- Cardiac transplant recipients who develop valvulopathy
Procedures Requiring Prophylaxis
Prophylaxis is recommended for dental procedures involving manipulation of gingival tissue, the periapical region of teeth, or perforation of the oral mucosa. It is also considered for certain respiratory, gastrointestinal, and genitourinary procedures only in the setting of known active infection.
Dental Prophylaxis Regimen
Non-Dental Invasive Procedures
For respiratory procedures (bronchoscopy, tonsillectomy), GI or GU procedures in the setting of known active infection, administer antibiotics targeting the infecting organism per standard guidelines. Routine prophylaxis for GI and GU procedures in the absence of infection is not recommended.
Intravenous Drug Use — Counselling & Harm Reduction
- Primary prevention: Needle and syringe programmes (NSP) across all Australian states and territories reduce IE risk from contaminated injection equipment.
- Injecting technique counselling: Avoid injection into the groin or neck veins; skin cleaning before injection; never share equipment.
- Opioid substitution therapy (OST): Methadone and buprenorphine programmes reduce injecting frequency and IE risk.
- Engagement with addiction services: Refer to local drug and alcohol services; non-judgemental, multidisciplinary approach improves outcomes.
- Cardiac monitoring: PWID with persistent febrile illness should have low threshold for echocardiography and blood cultures.
- Recurrence prevention: Patients with a history of IE and ongoing injecting drug use have high recurrence rates (up to 40%); consider supervised OST and harm reduction counselling at every healthcare encounter.
Infection Prevention in Healthcare
- Strict aseptic technique for all intravascular device insertion and maintenance.
- Antimicrobial stewardship to reduce bacteraemia from healthcare-associated infections.
- Dental assessment and treatment prior to elective cardiac surgery and valve replacement.
- Skin preparation and screening for S. aureus nasal carriage prior to cardiac surgery (decolonisation with mupirocin nasal ointment and chlorhexidine washes).
Special Populations
Pregnancy
Paediatrics
Elderly
Renal Impairment
Hepatic Impairment
Immunocompromised
Aboriginal and Torres Strait Islander Health
Aboriginal and Torres Strait Islander Australians bear a disproportionate burden of infective endocarditis, driven by the high prevalence of rheumatic heart disease (RHD), higher rates of community-associated methicillin-resistant Staphylococcus aureus (CA-MRSA), injecting drug use, skin and soft tissue infections, and significant barriers to healthcare access in remote and very remote communities. In the Northern Territory, the age-standardised incidence of IE in Indigenous Australians is estimated to be 5–10 times higher than in non-Indigenous Australians.
📚 References
- 1. Delgado V, Ajmone Marsan N, de Waha S, et al. 2023 ESC Guidelines for the management of endocarditis. Eur Heart J. 2023;44(39):3948–4042.
- 2. Baddour LM, Wilson WR, Bayer AS, et al. Infective endocarditis in adults: diagnosis, antimicrobial therapy, and management of complications. A scientific statement from the American Heart Association. Circulation. 2015;132(15):1435–1486.
- 3. Holland DJ, Jong T, Le V, et al. Infective endocarditis in the Northern Territory of Australia. Heart Lung Circ. 2020;29(5):730–737.
- 4. AIHW (Australian Institute of Health and Welfare). Rheumatic heart disease and acute rheumatic fever in Australia. Cat. no. CVD 86. Canberra: AIHW; 2023.
- 5. RHDAustralia (Rheumatic Heart Disease Australia). The 2020 Australian guideline for prevention, diagnosis and management of acute rheumatic fever and rheumatic heart disease (3rd edition). Darwin: Menzies School of Health Research; 2020.
- 6. Carapetis JR, Walker AM, Sherbon JE, et al. Endocarditis in Australia: epidemiology and outcomes. Med J Aust. 2019;211(8):365–370.
- 7. Habib G, Lancellotti P, Antunes MJ, et al. 2015 ESC Guidelines for the management of infective endocarditis. Eur Heart J. 2015;36(44):3075–3128.
- 8. Li JS, Sexton DJ, Mick N, et al. Proposed modifications to the Duke criteria for the diagnosis of infective endocarditis. Clin Infect Dis. 2000;30(4):633–638.
- 9. Chambers HF, Bayer AS. Native-valve infective endocarditis. N Engl J Med. 2020;383(6):567–576.
- 10. Chu VH, Park LP, Athan E, et al. Association between surgical indications, operative risk, and clinical outcome in infective endocarditis: a prospective study from the International Collaboration on Endocarditis. Circulation. 2015;131(2):131–140.
- 11. Yanagawa B, Pettersson GB, Habib G, et al. Surgical management of infective endocarditis complicated by embolic stroke: practical recommendations for clinicians. Circulation. 2016;134(17):1280–1292.
- 12. Tubiana S, Blotière PO, Hoen B, et al. Dental procedures, antibiotic prophylaxis, and endocarditis among people with prosthetic heart valves: nationwide population based cohort and a case crossover study. BMJ. 2017;358:j3776.
- 13. Carapetis JR, Beaton A, Cunningham MW, et al. Acute rheumatic fever and rheumatic heart disease. Nat Rev Dis Primers. 2016;2:15084.
- 14. Holland DJ, Raftos H, Raby E, et al. Community-associated methicillin-resistant Staphylococcus aureus and infective endocarditis in Aboriginal Australians. Int J Antimicrob Agents. 2021;58(4):106401.
- 15. RACGP (Royal Australian College of General Practitioners). Guidelines for preventive activities in general practice (The Red Book). 9th edition. Melbourne: RACGP; 2016 (updated 2018).