📋 Key Information Summary
- Vitamin D deficiency (25-OH vitamin D <50 nmol/L) is extremely common in Australia, affecting approximately 23–31% of adults, with higher prevalence in southern states, veiled populations, the elderly, and Aboriginal and Torres Strait Islander peoples.
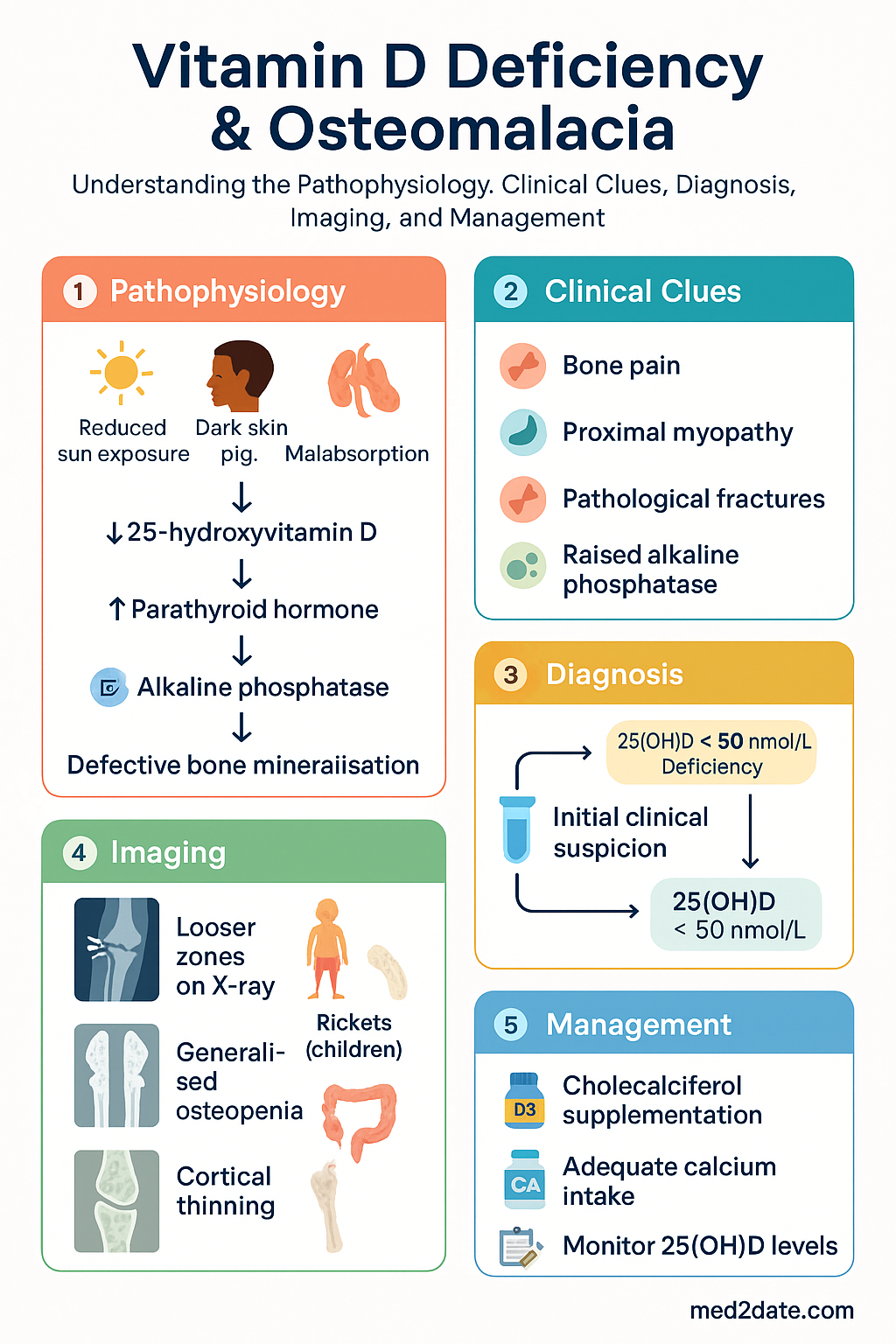
- Osteomalacia results from severe, prolonged vitamin D deficiency causing defective bone mineralisation — characterised by bone pain, proximal myopathy, pathological fractures, and raised alkaline phosphatase (ALP).
- Rickets is the paediatric equivalent, with growth-plate involvement, skeletal deformities (bowed legs, rachitic rosary, frontal bossing), and delayed milestones.
- 25-hydroxyvitamin D [25(OH)D] is the recommended screening test; levels <50 nmol/L define deficiency, 50–74 nmol/L insufficiency, and ≥75 nmol/L adequacy.
- Causes include reduced sun exposure (indoor lifestyle, veiling), dark skin pigmentation, malabsorption (coeliac disease, bariatric surgery), chronic kidney/hepatic disease, anticonvulsants, and obesity.
- Dietary sources alone are insufficient; most Australians require sunlight exposure and/or supplementation to maintain adequate levels.
- First-line supplementation: cholecalciferol (vitamin D₃) — loading dose followed by maintenance; ergocalciferol (D₂) is a less effective alternative.
- Calcitriol is reserved for patients with severe renal impairment or hepatic failure who cannot hydroxylate cholecalciferol.
- Concurrent calcium intake must be assessed and corrected (aim ≥1000–1200 mg/day in adults with osteomalacia).
- Monitoring: repeat 25(OH)D at 3–6 months after initiation; ALP normalises over 6–12 months with adequate treatment.
- Aboriginal and Torres Strait Islander populations have significantly higher prevalence of deficiency; culturally safe supplementation programmes and dietary education are essential.
- Hypervitaminosis D (>250 nmol/L) can cause hypercalcaemia — avoid empiric mega-dosing without monitoring.
🎧 Audio Brief
Introduction & Australian Epidemiology
Vitamin D deficiency is one of the most prevalent nutritional deficiencies worldwide and is remarkably common in sun-rich Australia. It causes defective bone mineralisation — osteomalacia in adults and rickets in children — and is independently associated with musculoskeletal weakness, falls, fractures, and impaired quality of life. Emerging evidence also links low vitamin D status to adverse cardiovascular, immune, and metabolic outcomes, though causality remains under investigation.
Australia's paradoxically high prevalence is driven by sun-safe messaging (slip, slop, slap), indoor working environments, multicultural demographics with darker skin pigmentation and cultural veiling, an ageing population, and high rates of obesity. The Australian Bureau of Statistics National Health Measures Survey (2011–12) found that 23% of adults were vitamin D-deficient (25-OH D <50 nmol/L), rising to 31% during winter–spring. Prevalence is highest in Victoria, Tasmania, and the ACT, and among Aboriginal and Torres Strait Islander peoples, where rates exceed 50–60% in some remote communities.
Despite increasing public and clinical awareness, osteomalacia remains underdiagnosed in Australian primary care, often presenting late with non-specific musculoskeletal symptoms, pathological fractures, or incidental biochemical findings. Early recognition and appropriate supplementation can reverse the condition in most patients.
Vitamin D Metabolism & Causes of Deficiency
Physiology
Vitamin D₃ (cholecalciferol) is synthesised in the skin from 7-dehydrocholesterol upon exposure to ultraviolet B radiation (wavelength 290–315 nm). It can also be obtained from dietary sources (oily fish, fortified foods, egg yolks, liver). Vitamin D₂ (ergocalciferol) is derived from plant sterols and fungi. Both forms undergo hepatic 25-hydroxylation (CYP2R1, CYP27A1) to produce 25-hydroxyvitamin D [25(OH)D], the major circulating form measured clinically. Subsequent renal 1α-hydroxylation (CYP27B1), regulated by parathyroid hormone (PTH), calcium, and phosphate, produces the active hormone 1,25-dihydroxyvitamin D [1,25(OH)₂D or calcitriol]. Calcitriol promotes intestinal calcium and phosphate absorption, bone mineralisation, and modulates immune function.
Causes of Deficiency
| Category | Examples | Mechanism |
|---|---|---|
| Reduced synthesis | Indoor lifestyle, institutionalised elderly, cultural veiling/burqa, high-latitude residence (southern Australia/Tasmania), winter season | Inadequate UVB exposure |
| Skin pigmentation | Darkly pigmented skin (Aboriginal, African, South Asian, Middle Eastern backgrounds) | Melanin absorbs UVB, reducing synthesis by up to 90% |
| Malabsorption | Coeliac disease, inflammatory bowel disease, bariatric surgery, cholestatic liver disease, cystic fibrosis, pancreatic insufficiency | Fat-soluble vitamin malabsorption; reduced bile salts |
| Impaired metabolism | Chronic kidney disease (CKD stages 3–5), hepatic failure | Reduced 1α-hydroxylation |
| Increased catabolism | Anticonvulsants (phenytoin, carbamazepine, phenobarbitone), rifampicin, glucocorticoids | Induction of CYP enzymes (CYP3A4) accelerating 25(OH)D degradation |
| Obesity | BMI ≥30 kg/m² | Vitamin D sequestration in adipose tissue; volumetric dilution |
| Inadequate intake | Strict veganism, exclusive breastfeeding (without supplementation), anorexia nervosa | Low dietary vitamin D; breast milk contains only ~25 IU/L |
Clinical Features
Osteomalacia (Adults)
Osteomalacia results from failure of osteoid mineralisation. Onset is typically insidious.
- Bone pain: Diffuse, deep, aching — most commonly affecting the pelvis, lumbar spine, ribs, and lower limbs. Often worse with weight-bearing and palpation of bone (tibial tenderness is a classic sign).
- Proximal myopathy: Difficulty rising from a chair, climbing stairs, or walking. Waddling gait pattern. Reflects both vitamin D receptor effects on skeletal muscle and hypophosphataemia.
- Fatigue and weakness: Non-specific but common; may be the presenting complaint.
- Pathological fractures: Insufficiency fractures, particularly of the femoral neck, pubic rami, and vertebrae (pseudofractures/Looser zones on X-ray are pathognomonic).
- Tetany and paraesthesiae: In severe cases with hypocalcaemia — Chvostek's and Trousseau's signs may be positive.
- Waddling gait: Due to combined proximal myopathy and pelvic bone pain.
Rickets (Children)
- Skeletal deformities: Bowed legs (genu varum) or knock knees (genu valgum), frontal bossing, craniotabes (soft occipital skull), rachitic rosary (costochondral beading).
- Delayed milestones: Late walking, fontanelle closure delay.
- Growth retardation: Short stature, widened wrists and ankles.
- Dental abnormalities: Enamel hypoplasia, delayed eruption.
- Hypocalcaemic seizures: May be the presenting feature, especially in infants of dark-skinned mothers with low vitamin D status.
Investigations
Biochemical Investigations
Imaging
| Modality | Findings in Osteomalacia/Rickets | MBS Item |
|---|---|---|
| X-ray (long bones) | Looser zones (pseudofractures) — radiolucent lines perpendicular to cortex, typically at pubic rami, femoral neck, scapula, ribs. Generalised osteopenia, cortical thinning. In rickets: widened, frayed metaphyses, cupped growth plates. | 57508 (limb), 57708 (pelvis) |
| DXA scan | Low bone mineral density (T-score ≤ −1.0) — often significantly reduced. Repeat after 12–24 months of treatment to document recovery. Not diagnostic of osteomalacia per se. | 12320 |
| Bone biopsy (gold standard) | Increased osteoid volume, wide osteoid seams (>12.5 µm), reduced mineralisation rate on tetracycline labelling. Rarely performed — diagnosis is usually clinical + biochemical. | Specialist only |
Management (Supplementation)
Treatment Principles
- Correct vitamin D deficiency with a loading (repletion) dose followed by a long-term maintenance dose.
- Ensure adequate concurrent calcium intake (diet ± supplements).
- Treat the underlying cause where possible (e.g., coeliac disease, medication review).
- Monitor response biochemically (25-OH D, ALP, calcium, PTH) and clinically.
Cholecalciferol (Vitamin D₃) — First-Line
Ergocalciferol (Vitamin D₂) — Alternative
Calcitriol (1,25-Dihydroxyvitamin D₃) — Specialist Use
Calcium Supplementation
Monitoring Schedule
Special Populations
Aboriginal and Torres Strait Islander Health Considerations
📚 References
- 1. Nowson CA, McGrath JJ, Ebeling PR, et al. Vitamin D and health in adults in Australia and New Zealand: a position statement. Med J Aust. 2012;196(11):686–687.
- 2. Daly RM, Gagnon C, Lu ZX, et al. Prevalence of vitamin D deficiency and its determinants in Australian adults aged 25 years and older: a national, population-based study. Clin Endocrinol (Oxf). 2012;77(1):26–35.
- 3. Australian Institute of Health and Welfare (AIHW). Australia's health 2022: data insights. Canberra: AIHW; 2022.
- 4. Munns CF, Shaw N, Kiely M, et al. Global consensus recommendations on prevention and management of nutritional rickets. J Clin Endocrinol Metab. 2016;101(2):394–415.
- 5. Royal Australian College of General Practitioners (RACGP). RACGP position statement: Vitamin D and adult bone health in Australia. Melbourne: RACGP; 2012.
- 6. Bischoff-Ferrari HA, Willett WC, Orav EJ, et al. A pooled analysis of vitamin D dose requirements for fracture prevention. N Engl J Med. 2012;367(1):40–49.
- 7. Sanders KM, Stuart AL, Williamson EJ, et al. Annual high-dose oral vitamin D and falls and fractures in older women: a randomized controlled trial. JAMA. 2010;303(18):1815–1822.
- 8. Holick MF, Binkley NC, Bischoff-Ferrari HA, et al. Evaluation, treatment, and prevention of vitamin D deficiency: an Endocrine Society clinical practice guideline. J Clin Endocrinol Metab. 2011;96(7):1911–1930.
- 9. National Health and Medical Research Council (NHMRC). Nutrient reference values for Australia and New Zealand including recommended dietary intakes. Canberra: NHMRC; 2006.
- 10. Royal Australasian College of Physicians (RACP). Position statement: Vitamin D and health in pregnancy, infancy and childhood. Sydney: RACP; 2013.
- 11. KDIGO 2017 Clinical Practice Guideline Update for the Diagnosis, Evaluation, Prevention, and Treatment of Chronic Kidney Disease–Mineral and Bone Disorder (CKD-MBD). Kidney Int Suppl. 2017;7(1):1–59.
- 12. Gutiérrez OM, Farwell WR, Kermah D, Taylor EN. Racial differences in the relationship between vitamin D, bone mineral density, and parathyroid hormone in the National Health and Nutrition Examination Survey. Osteoporos Int. 2011;22(6):1745–1753.
- 13. Maple-Brown LJ, Hughes JT, Lu ZX, et al. Vitamin D in Aboriginal and Torres Strait Islander peoples of the Northern Territory. Aust N Z J Public Health. 2019;43(2):180–184.
- 14. Winzenberg T, Jones G. Vitamin D and bone health in childhood and adolescence. Calcif Tissue Int. 2013;92(2):140–150.