📋 Key Information Summary
- Thyroiditis is inflammation of the thyroid gland, classified by aetiology and clinical course (painful vs painless, duration).
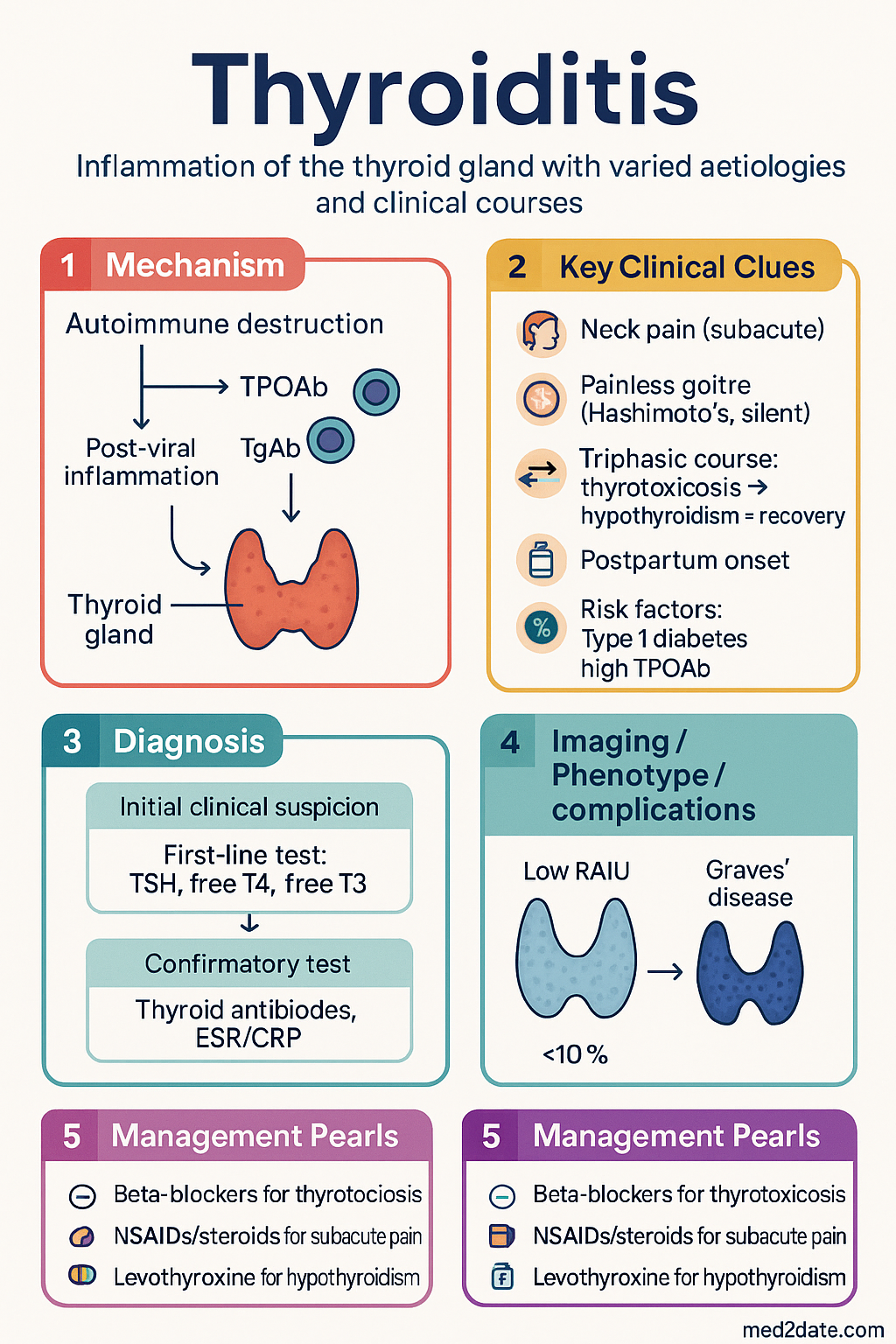
- Key types in Australia: Hashimoto's (chronic autoimmune), subacute (de Quervain's, painful), silent (painless autoimmune), and postpartum thyroiditis.
- Clinical course typically follows a triphasic pattern: thyrotoxicosis → hypothyroidism → recovery (may not occur in all types).
- Subacute thyroiditis often follows a viral infection, presents with neck pain, fever, and elevated ESR/CRP.
- Investigations: TSH, free T4, free T3, ESR/CRP (for subacute), thyroid antibodies (TPOAb, TgAb), and ultrasound.
- Management is primarily symptomatic: beta-blockers for thyrotoxicosis, NSAIDs/steroids for pain in subacute, and levothyroxine for persistent hypothyroidism.
- Distinguish thyrotoxicosis in thyroiditis (low radioactive iodine uptake) from Graves' disease (high uptake) for appropriate therapy.
- Monitor for progression to hypothyroidism, especially in postpartum and silent thyroiditis.
- Consider amiodarone-induced thyroiditis (AIT) type 1 (excess synthesis) and type 2 (destructive) in patients on amiodarone.
- ATSI populations have higher prevalence of thyroid autoimmunity; ensure culturally safe care and monitoring.
🎧 Audio Brief
Introduction & Australian Epidemiology
Thyroiditis refers to a group of inflammatory conditions affecting the thyroid gland. Inflammation may be acute, subacute, or chronic, and can lead to transient thyrotoxicosis, hypothyroidism, or a biphasic disturbance of thyroid function. The most common forms encountered in Australian clinical practice are Hashimoto's thyroiditis (chronic autoimmune), subacute thyroiditis (de Quervain's), silent thyroiditis (painless autoimmune), and postpartum thyroiditis.
In Australia, Hashimoto's thyroiditis is the most common cause of hypothyroidism, with a prevalence of autoimmune thyroid disease estimated at 5-10% of the general population. Subacute thyroiditis is less common but frequently presents to primary care and emergency departments. Postpartum thyroiditis affects approximately 5-10% of women within the first year after delivery. Aboriginal and Torres Strait Islander populations may have a different spectrum and prevalence of thyroid disorders, requiring tailored clinical awareness.
Classification & Pathophysiology
Thyroiditis is classified based on aetiology, clinical presentation (painful vs painless), and duration of illness.
| Type | Aetiology/Pathogenesis | Typical Course |
|---|---|---|
| Hashimoto's (Chronic Lymphocytic) | Autoimmune destruction mediated by T-lymphocytes and thyroid autoantibodies (TPOAb, TgAb). Genetic predisposition with environmental triggers. | Chronic, progressive to permanent hypothyroidism. |
| Subacute (de Quervain's) | Post-viral inflammatory response. Often follows upper respiratory tract infections. Not autoimmune. | Self-limiting, triphasic: thyrotoxicosis (1-3 months) → hypothyroidism (1-3 months) → recovery. |
| Silent (Painless) | Autoimmune (often TPOAb positive), similar to Hashimoto's but with a destructive, transient course. | Triphasic like subacute, but painless. May recur. |
| Postpartum | Exacerbation of underlying silent thyroiditis in the postpartum period (immune rebound). | Thyrotoxicosis (1-4 months postpartum) → hypothyroidism (4-8 months) → recovery (majority). |
| Drug-Induced (e.g., Amiodarone, Immune Checkpoint Inhibitors) | Amiodarone: Type 1 (excess synthesis due to iodine load) or Type 2 (destructive). Checkpoint inhibitors: autoimmune. | Variable; may be permanent or transient. |
The pathophysiology of thyrotoxicosis in thyroiditis is due to glandular inflammation and destruction, releasing preformed thyroid hormones (colloid leak), not increased synthesis. This results in a low radioactive iodine uptake (RAIU) on nuclear imaging, distinguishing it from Graves' disease.
Clinical Features & Natural History
Presentation varies by type but often follows a predictable pattern.
Subacute (de Quervain's) Thyroiditis
- Prodrome: Recent viral-like illness (fever, malaise, myalgia).
- Pain: Anterior neck pain, often radiating to the jaw or ears. Pain worsens with neck movement or palpation.
- Thyrotoxic Phase (Weeks 1-6): Symptoms of thyrotoxicosis (anxiety, palpitations, weight loss, tremor) due to hormone release. Gland is tender, firm, and enlarged.
- Hypothyroid Phase (Weeks 8-16): Fatigue, cold intolerance, constipation as stored hormone depletes.
- Recovery: Majority return to euthyroidism within 6-12 months. A small percentage develop permanent hypothyroidism.
Hashimoto's Thyroiditis
- Often presents with gradual, painless enlargement of the thyroid (goitre) and symptoms of hypothyroidism.
- May initially present with a transient thyrotoxic phase ("Hashitoxicosis") due to glandular destruction.
- High risk of progression to permanent hypothyroidism.
Silent & Postpartum Thyroiditis
- Painless goitre may be present. Thyrotoxic phase is often mild and overlooked.
- Postpartum thyroiditis typically presents with thyrotoxicosis 1-4 months after delivery, followed by hypothyroidism 4-8 months postpartum.
- Risk factors: Type 1 diabetes, personal/family history of autoimmunity, high TPOAb titre in early pregnancy.
Investigations
A stepwise approach differentiates thyroiditis from other causes of thyrotoxicosis or hypothyroidism.
Management
Treatment is largely supportive and based on the clinical phase. Patient education on the natural history is crucial.
Thyrotoxic Phase Management
Pain Management (Subacute Thyroiditis)
- First-line: NSAIDs (e.g., Ibuprofen 400 mg PO TDS with food, or Naproxen 500 mg PO BD). PBS General Benefit.
- Second-line: Oral corticosteroids (see above) for refractory pain.
Hypothyroid Phase Management
Monitoring
- Check TSH and free T4 every 4-8 weeks during active phases.
- Once stable on levothyroxine, annual TSH monitoring is sufficient.
- Educate patients on symptoms of both hyperthyroidism and hypothyroidism to report.
Special Populations
Aboriginal and Torres Strait Islander Health Considerations
Thyroid disease, particularly autoimmune thyroiditis, may be underdiagnosed in Aboriginal and Torres Strait Islander populations. A culturally safe approach is essential for optimal care.
📚 References
- 1. Royal Australian College of General Practitioners (RACGP). Management of thyroid disorders in primary care. RACGP White Book. 2020.
- 2. Australian Institute of Health and Welfare (AIHW). Aboriginal and Torres Strait Islander health performance framework. AIHW; 2023.
- 3. Pearce EN, Farwell AP, Braverman LE. Thyroiditis. N Engl J Med. 2003;348(26):2646-55.
- 4. Stasiak M, Lewiński A. New aspects in the pathogenesis and management of subacute thyroiditis. Rev Endocr Metab Disord. 2021;22(4):1027-39.
- 5. Ross DS, Burch HB, Cooper DS, et al. 2016 American Thyroid Association Guidelines for Diagnosis and Management of Hyperthyroidism and Other Causes of Thyrotoxicosis. Thyroid. 2016;26(10):1343-1421.
- 6. Alexander EK, Pearce EN, Brent GA, et al. 2017 Guidelines of the American Thyroid Association for the Diagnosis and Management of Thyroid Disease During Pregnancy and the Postpartum. Thyroid. 2017;27(3):315-389.
- 7. The Pharmaceutical Benefits Scheme (PBS). Australian Government Department of Health. Available at: https://www.pbs.gov.au.
- 8. NHMRC. Australian guidelines to reduce health risks from drinking alcohol. NHMRC; 2020.
- 9. RHDAustralia (RACP). 2022 Australasian Society for HIV, Viral Hepatitis and Sexual Health Medicine (ASHM) HIV/hepatitis C guidelines.
- 10. Fatourechi V, Aniszewski JP, Fatourechi GZ, Atkinson EJ, Jacobsen SJ. Clinical features and outcome of subacute thyroiditis in an incidence cohort: Olmsted County, Minnesota, study. J Clin Endocrinol Metab. 2003;88(5):2100-5.