📋 Key Information Summary
- Non-thyroidal illness syndrome (NTIS), also termed sick euthyroid syndrome or euthyroid sick syndrome, is the most common cause of abnormal thyroid function tests in hospitalised patients.
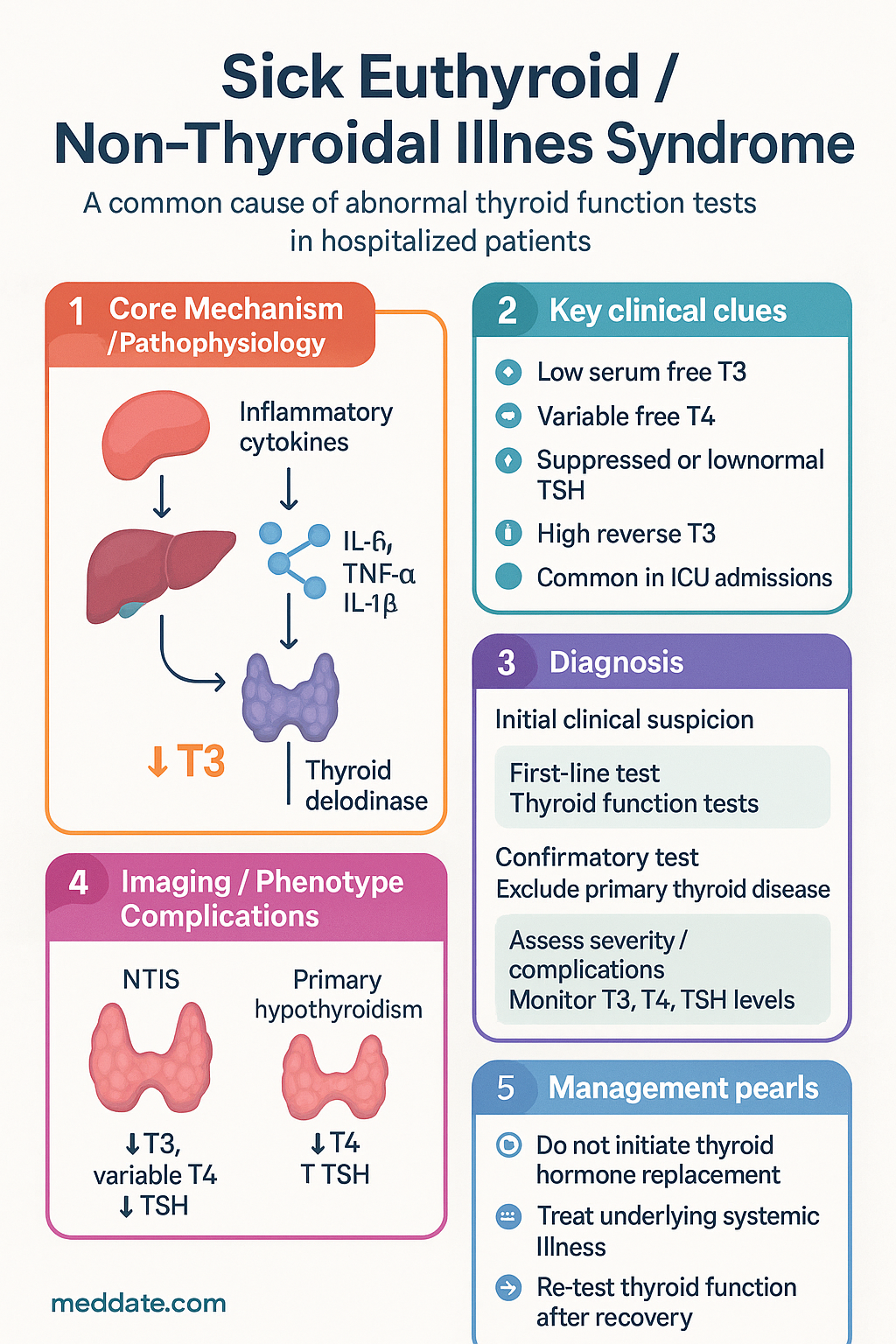
- NTIS is a neuroendocrine adaptive response — not primary thyroid disease — and does not require thyroid hormone replacement in the vast majority of cases.
- The hallmark biochemical pattern is low serum free T3 (triiodothyronine), with variable free T4 (thyroxine) and suppressed or low-normal TSH.
- Type 3 deiodinase upregulation in peripheral tissues converts T4 to reverse T3 (rT3), driving the characteristic low-T3 / high-rT3 pattern.
- Low-T3 syndrome is present in up to 70 % of intensive care unit admissions and correlates with illness severity and mortality.
- Free T4 below 10 pmol/L in critically ill patients is independently associated with increased mortality; TSH < 0.1 mIU/L with low T4 raises concern for secondary hypothyroidism or drug effect.
- Key differential diagnoses that must be excluded include central hypothyroidism, drug-induced thyroid dysfunction (amiodarone, dopamine, glucocorticoids, checkpoint inhibitors), and pre-existing but undiagnosed primary hypothyroidism.
- Thyroid function tests should generally not be ordered in acutely unwell patients unless there are specific clinical features of thyroid disease (goitre, exophthalmos, pretibial myxoedema, tremor with tachycardia disproportionate to the clinical picture).
- Re-testing 2–3 months after acute illness recovery is the most reliable strategy to confirm or exclude true thyroid disease.
- Levothyroxine therapy is not recommended for NTIS; the two major randomised controlled trials (TRH-analogue in critical illness and T4 replacement) showed no survival benefit and potential harm.
- Identify and treat the underlying systemic illness aggressively — this is the only proven management that normalises thyroid function.
- In Australian Aboriginal and Torres Strait Islander populations, higher rates of chronic disease and delayed presentation may increase NTIS prevalence; culturally safe communication about "not needing thyroid tablets" is essential.
- Medicare item 66712 (thyroid function tests) is rebatable; however, testing in the setting of acute illness often generates confounding results — consider clinical justification.
🎧 Audio Brief
Introduction & Australian Epidemiology
Non-thyroidal illness syndrome (NTIS) — historically termed "sick euthyroid syndrome" or "euthyroid sick syndrome" — refers to a spectrum of changes in circulating thyroid hormone concentrations that occur in the context of significant systemic illness, critical illness, starvation, or major surgery, in the absence of intrinsic hypothalamic–pituitary–thyroid (HPT) axis pathology. It represents an adaptive neuroendocrine response rather than a disease process per se.
NTIS is the most frequently encountered cause of abnormal thyroid function tests (TFTs) in hospitalised patients worldwide, and this is no different in the Australian context. The prevalence depends on the clinical setting and the severity of illness:
- General medical wards: approximately 15–20 % of patients with significant illness demonstrate at least one abnormal TFT consistent with NTIS.
- Intensive care units (ICUs): prevalence rises to 50–70 %, with low free T3 seen in up to 80 % of mechanically ventilated patients.
- Post-cardiac surgery: NTIS is nearly universal in the first 48 hours following cardiopulmonary bypass.
- Chronic kidney disease: low T3 is found in approximately 50 % of patients on maintenance haemodialysis.
- Major burns: a nadir T3 at 3–5 days post-burn is an expected finding, with recovery correlating to wound healing.
In Australia, NTIS carries particular relevance in several high-burden disease populations: sepsis (approximately 18 000 new cases per year nationally), decompensated heart failure (where low T3 is independently predictive of mortality), cirrhosis, and severe COVID-19 infection. The 2020–2022 pandemic reinforced the prognostic significance of low T3 in COVID-19, with Australian ICU data mirroring international findings of an association between low free T3 and ICU mortality.
A critical clinical pitfall — and the central reason for this guideline — is the misidentification of NTIS as primary hypothyroidism, leading to inappropriate initiation of levothyroxine. Australian data from the Pharmaceutical Benefits Scheme (PBS) indicate that levothyroxine dispensing has increased steadily over the past decade; the extent to which NTIS contributes to unnecessary prescribing is not quantified but is widely acknowledged by endocrinologists as a significant clinical concern.
Pathophysiology (Deiodinase Changes)
Understanding NTIS requires appreciation of the three iodothyronine deiodinase enzymes (DIO1, DIO2, DIO3) and their tissue-specific regulation during systemic illness.
Normal Thyroid Hormone Metabolism
The thyroid gland secretes predominantly T4 (thyroxine), a relatively inactive prohormone. Conversion to the biologically active T3 (triiodothyronine) occurs peripherally through the removal of a single iodine atom from the outer ring of T4. Approximately 80 % of circulating T3 is derived from peripheral conversion, with the remainder secreted directly by the thyroid.
| Deiodinase | Primary Function | Key Tissues | Change in NTIS |
|---|---|---|---|
| DIO1 (Type 1) | Outer-ring deiodination: T4 → T3; also clears rT3 | Liver, kidney, thyroid | ↓ Downregulated by IL-6, TNF-α; reduced T3 production and rT3 clearance |
| DIO2 (Type 2) | Outer-ring deiodination: T4 → T3 (local tissue supply) | Brain, pituitary, BAT, skeletal muscle | Variable — ↑ in pituitary (driving TSH suppression), ↓ in hypothalamus |
| DIO3 (Type 3) | Inner-ring deiodination: T4 → rT3; T3 → T2 (inactivation) | Placenta, brain, skin, many tissues during inflammation | ↑ Upregulated — central driver of low T3 and elevated rT3 |
The Cascade of Changes
During systemic illness, a coordinated neuroendocrine response unfolds:
- Peripheral deiodinase shift (hours to days): Pro-inflammatory cytokines — interleukin-6 (IL-6), tumour necrosis factor-alpha (TNF-α), and interleukin-1-beta (IL-1β) — suppress hepatic DIO1 activity while simultaneously upregulating DIO3 expression in peripheral tissues. This results in decreased conversion of T4 to T3 and increased conversion of T4 to the metabolically inactive reverse T3 (rT3). Serum T3 falls; rT3 rises.
- Altered thyroid hormone binding (acute phase): Inflammatory cytokines reduce the synthesis of thyroid-binding globulin (TBG), transthyretin (prealbumin), and albumin. They also modify binding affinity through desialylation and oxidation of binding proteins. This contributes to the fall in total T4 and T3, though free hormone levels may initially be preserved.
- Hypothalamic–pituitary changes (days to weeks): In prolonged critical illness, sustained elevation of cytokines and cortisol, together with dopaminergic and somatostatinergic tone, suppresses hypothalamic TRH secretion. Pituitary TSH secretion consequently falls. Additionally, increased DIO2 activity in the pituitary locally amplifies T3 signalling, further suppressing TSH despite low circulating T3 — a form of central feedback override.
- Tissue-level thyroid hormone transport: Expression of monocarboxylate transporter 8 (MCT8) and other thyroid hormone transporters in the brain is altered during illness, potentially contributing to intracellular thyroid hormone depletion in neural tissue despite changing circulating levels.
- Cortisol and NTIS: Elevated cortisol (via the parallel HPA axis activation) independently suppresses TSH and DIO1. This mechanism is distinct from, and additive to, cytokine-mediated changes.
Clinical Patterns (Low T3, Low T4, TSH Changes)
NTIS follows a predictable temporal progression that varies with illness severity. Three broad phases have been described:
Characteristic Biochemical Profile
| Parameter | NTIS Pattern | Australian Reference Range (Adult) |
|---|---|---|
| Free T3 | ↓ Low (hallmark finding) | 3.5–6.5 pmol/L |
| Free T4 | Normal → Low as severity increases | 10–20 pmol/L |
| TSH | Normal → Low / Suppressed | 0.4–4.0 mIU/L |
| Reverse T3 | ↑ Elevated | 0.10–0.45 nmol/L (not routinely measured in Australia) |
| Thyroglobulin | Normal | Not routinely measured |
| TPO Antibodies | Negative (unless coincidental autoimmune thyroiditis) | Negative |
Conditions Associated with NTIS
- Sepsis and septic shock
- Acute myocardial infarction
- Decompensated heart failure
- Liver cirrhosis
- Chronic kidney disease (especially stage 4–5, dialysis)
- Major trauma and burns
- Post-cardiopulmonary bypass
- Malignancy (especially advanced solid organ tumours)
- Starvation, anorexia nervosa, protein-calorie malnutrition
- Severe COVID-19 and other critical viral infections
- Diabetic ketoacidosis
- Bone marrow transplantation
Differentiation from True Thyroid Disease
Differentiating NTIS from genuine thyroid disease is one of the most clinically important — and frequently encountered — challenges in hospital medicine. Misdiagnosis leads to unnecessary treatment, missed diagnoses, or both.
Key Diagnostic Approach
Differentiating NTIS from Thyroid Disease — Comparison Table
| Feature | NTIS | Primary Hypothyroidism | Central Hypothyroidism |
|---|---|---|---|
| TSH | Normal → Low (but usually > 0.1) | ↑ Elevated (> 10 mIU/L typical) | ↓ Low or inappropriately normal |
| Free T4 | Normal → Low | ↓ Low | ↓ Low |
| Free T3 | ↓ Low | ↓ Low | ↓ Low |
| Reverse T3 | ↑ Elevated | Normal or Low | Normal or Low |
| TPO Abs | Negative (unless co-existing) | Often positive (Hashimoto's) | Negative |
| TSH response to TRH | Delayed but present | Exaggerated | Absent or blunted |
| Clinical context | Acute/severe systemic illness | Often insidious, may predate illness | Pituitary/hypothalamic pathology |
| On recovery | Normalises | Persists | Persists |
Drugs That Alter Thyroid Function Tests
| Drug | Effect on TFTs | Mechanism |
|---|---|---|
| Amiodarone | ↑ T4, variable TSH; can cause amiodarone-induced thyrotoxicosis (AIT) type 1 or 2, or hypothyroidism | Iodine excess (37 % iodine by weight); DIO1/DIO2 inhibition; direct thyroid toxicity |
| Glucocorticoids (high dose) | ↓ TSH (suppressed); ↓ T3; ↓ TBG | Direct TSH suppression; hepatic DIO1 inhibition |
| Dopamine (IV infusion) | ↓ TSH; ↓ T4; ↓ T3 | Dopaminergic suppression of TRH/TSH |
| Checkpoint inhibitors (IO) | ↓ or ↑ TSH; destructive thyroiditis | Immune-mediated thyroid destruction |
| Tyrosine kinase inhibitors | ↓ T3, ↓ T4, variable TSH | DIO1/DIO3 alteration; possible direct thyroid toxicity |
| Heparin (in vitro effect) | Spuriously ↑ free T4 on certain assays | Heparin-activated lipase releases free fatty acids that displace T4 from TBG in vitro |
Management
The management of NTIS is fundamentally different from the management of thyroid disease. The guiding principle is: NTIS is not a thyroid problem — it is the consequence of a systemic illness.
Core Management Principles
Scenarios Requiring Thyroid Treatment Despite NTIS Overlap
In a small number of situations, genuine thyroid disease may co-exist with NTIS or be unmasked by it. Consider treatment when:
- Known hypothyroidism on levothyroxine: Continue usual dose; do not increase.
- New presentation of myxoedema coma: Extremely rare but life-threatening. Suspect when there is hypothermia (< 35 °C), bradycardia, altered consciousness, and periorbital/oedematous features in the absence of other explanations. Manage in ICU with IV levothyroxine (loading dose 200–500 micrograms IV, then 50–100 micrograms IV daily) and IV hydrocortisone 100 mg stat then 50 mg 8-hourly (given before or with T4 to avoid adrenal crisis). Specialist endocrinology consultation is mandatory.
- Thyroid storm: Differentiated from NTIS by high T3/T4, suppressed TSH, and features of thyrotoxic crisis (fever, tachycardia, delirium). Treated with carbimazole 20–40 mg PO/NG (or propylthiouracil if thyroid storm — 500 mg loading then 250 mg 4-hourly), propranolol, and ICU support. Not confused with NTIS if the clinical picture is carefully assessed.
Investigations — What to Order and When
Pharmacotherapy Summary — Medications Referenced
Special Populations
Aboriginal and Torres Strait Islander Health Considerations
📚 References
- 1. Van den Berghe G. Non-thyroidal illness in the ICU: a syndrome with different faces. Thyroid. 2014;24(10):1456–1465.
- 2. Warner MH, Breslow MJ, Lubomski PJ, et al. Thyroid hormone replacement in critically ill patients with non-thyroidal illness: a randomised, double-blind, placebo-controlled trial. Lancet. 1996;348(9032):405–408.
- 3. Van den Berghe G, de Zegher F, Baxter RC, et al. Neuroendocrinology of prolonged critical illness: effects of exogenous thyrotropin-releasing hormone and its combination with growth hormone secretagogues. J Clin Endocrinol Metab. 1998;83(2):309–319.
- 4. Chaker L, Bianco AC, Jonklaas J, Peeters RP. Hypothyroidism. Lancet. 2017;390(10101):1550–1562.
- 5. Fliers E, Bianco AC, Langouche L, Boelen A. Thyroid function in critically ill patients. Lancet Diabetes Endocrinol. 2015;3(10):816–825.
- 6. Australian Institute of Health and Welfare (AIHW). Cardiovascular disease, diabetes and chronic kidney disease — Australian facts: Aboriginal and Torres Strait Islander people. Cat. no. CDK 5. Canberra: AIHW; 2015.
- 7. Bello G, Pennisi MA, Montini L, et al. Nonthyroidal illness syndrome and prolonged mechanical ventilation in patients admitted to the ICU. Chest. 2009;135(6):1448–1454.
- 8. Economidou F, Douka E, Tzanela M, Nanas S, Kotanidou A. Thyroid function during critical illness. Hormones (Athens). 2011;10(2):117–124.
- 9. RACGP. Thyroid disease — a guide to diagnosis and management in general practice. East Melbourne: The Royal Australian College of General Practitioners; 2023.
- 10. Wiersinga WM, de Graeff PA, Völzke H, et al. Nonthyroidal illness syndrome. In: Feingold KR, Anawalt B, Blackman MR, et al., eds. Endotext. South Dartmouth (MA): MDText.com, Inc.; 2000–2024.
- 11. Andersen S, Bruun NH, Pedersen KM, Laurberg P. Biologic variation is important for interpretation of thyroid function tests. Thyroid. 2003;13(11):1069–1078.
- 12. Suárez-Ortegón MF, Beltrán-Anaya FO, Mosquera M, et al. Association of low T3 with mortality in COVID-19: a systematic review and meta-analysis. Eur J Endocrinol. 2022;187(4):557–566.
- 13. Services Australia. MBS Online — Medicare Benefits Schedule. Australian Government. Available at: www.mbsonline.gov.au. Accessed 2024.