📋 Key Information Summary
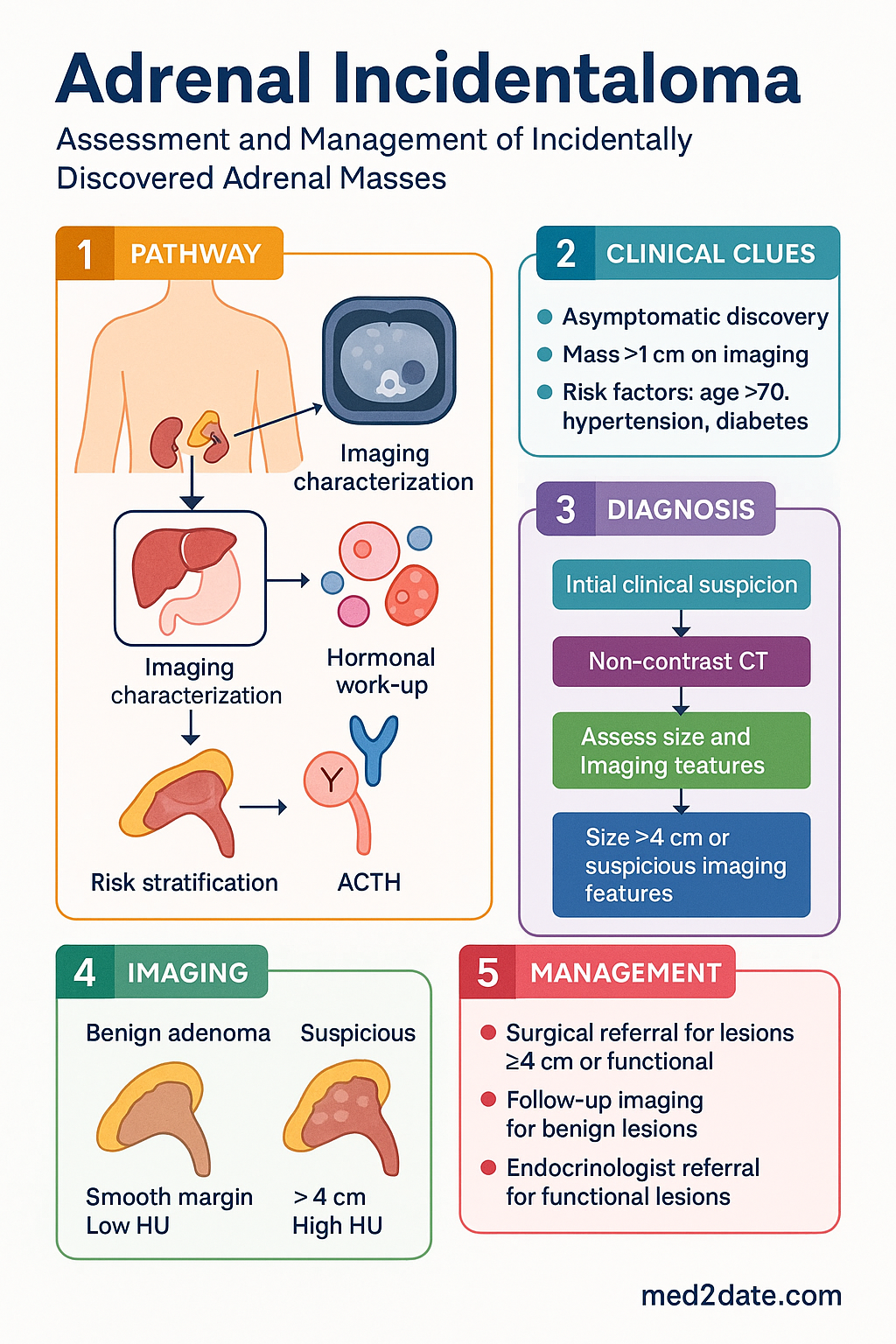
- An adrenal incidentaloma is an adrenal mass ≥1 cm discovered incidentally on imaging performed for unrelated reasons.
- Prevalence is approximately 4–5% on abdominal CT; most (80–85%) are benign, non-functioning adenomas.
- The primary assessment goals are to exclude malignancy and identify hormonally active tumours.
- All patients require a non-contrast CT for characterisation and a basic hormonal work-up.
- Mandatory hormonal screening includes overnight dexamethasone suppression test (cortisol), plasma free metanephrines (phaeochromocytoma), and plasma aldosterone concentration/renin ratio (if hypertensive).
- Imaging features suspicious for malignancy: size >4 cm, irregular margins, high unenhanced Hounsfield units (>10 HU), and delayed washout.
- Functional tumours (Cushing’s, phaeochromocytoma, aldosteronoma) require specific management, often surgery.
- For non-functioning lesions, size and imaging characteristics dictate management: surgery for ≥4 cm or suspicious features; follow-up imaging for smaller, benign-appearing lesions.
- Biochemical follow-up is recommended at 6–12 months for non-functioning adenomas to detect subclinical hormone production.
- Consider referral to an endocrinologist or endocrine surgeon for all functional lesions, lesions ≥4 cm, or those with suspicious imaging.
- Aboriginal and Torres Strait Islander peoples have a higher prevalence of hypertension and diabetes, which may influence the detection and hormonal work-up of incidentalomas.
🎧 Audio Brief
Introduction & Australian Epidemiology
An adrenal incidentaloma is an adrenal mass, typically ≥1 cm in diameter, discovered incidentally during imaging performed for an unrelated clinical indication. The widespread use of high-resolution cross-sectional imaging (CT, MRI) has led to a significant increase in their detection, presenting a common clinical dilemma in endocrinology and general practice.
The fundamental clinical imperative is twofold: to exclude adrenocortical carcinoma and to identify any tumour with autonomous hormone secretion, as these conditions necessitate specific intervention. The vast majority (80–85%) are benign, non-functioning cortical adenomas. However, a systematic approach is required to avoid missing clinically significant pathology.
Australian Epidemiology
Australian data mirrors international trends. Incidentalomas are found in approximately 4–5% of abdominal CT scans. Prevalence increases with age, affecting up to 10% of individuals over 70 years. There is no significant gender predilection, though some studies suggest a slightly higher frequency in women. The increasing utilisation of imaging in Australia's ageing population means these lesions are frequently encountered in primary and secondary care.
Epidemiology & Classification
Aetiological Classification
Adrenal incidentalomas can be classified by histology and functional status.
| Type | Approximate Frequency | Key Features |
|---|---|---|
| Non-functioning adenoma | 70–80% | Benign, lipid-rich, low HU on CT. |
| Subclinical Cushing’s syndrome | 5–10% | Autonomous cortisol secretion without overt Cushing’s syndrome. |
| Phaeochromocytoma | ~5% | Catecholamine-producing tumour from adrenal medulla. |
| Aldosteronoma | ~1–2% | Associated with primary aldosteronism and hypertension. |
| Adrenocortical carcinoma | ~2–5% | Aggressive malignancy; often larger (>4 cm) and functional. |
| Metastasis | ~5% | From lung, breast, melanoma, kidney primaries; often bilateral. |
| Other (cyst, myelolipoma, haemorrhage) | ~5% | Often have characteristic imaging features. |
Hormonal Work-Up
A systematic hormonal evaluation is required for all incidentalomas ≥1 cm, regardless of size or imaging characteristics. The work-up aims to exclude the three major functional syndromes.
1. Cortisol Excess (Cushing's Syndrome)
2. Catecholamine Excess (Phaeochromocytoma)
3. Aldosterone Excess (Primary Aldosteronism)
Screen only if the patient has hypertension or unexplained hypokalaemia. Test using the plasma aldosterone concentration/plasma renin activity (PAC/PRA) ratio. Patients should ideally be on a liberal sodium diet and medications like spironolactone and beta-blockers withheld for weeks prior.
Imaging Characterisation (CT/MRI)
Imaging is critical for assessing the risk of malignancy. A dedicated adrenal protocol CT is the investigation of choice.
Key Imaging Features
MRI Utility
MRI with chemical shift imaging is useful for confirming intracellular lipid in adenomas (signal drop on out-of-phase images). It is superior for characterising cysts, myelolipomas (fat signal), and assessing venous invasion in large tumours. It is the modality of choice in young patients or those requiring avoidance of iodinated contrast.
Management Algorithm
Management is guided by functional status, size, and imaging characteristics.
Clinical Presentation & Diagnostic Criteria
By definition, an incidentaloma is asymptomatic and discovered incidentally. The diagnostic approach focuses on risk stratification.
Diagnostic Criteria
- Imaging finding of an adrenal mass ≥1 cm in diameter on a study not performed for suspected adrenal disease.
- Exclusion of patients with known extra-adrenal malignancy (where the mass is likely a metastasis) or a history of adrenal cancer.
Clinical Evaluation
A thorough history and physical examination should be performed to look for subtle signs of hormone excess (e.g., easy bruising, proximal muscle weakness, new hypertension, paroxysmal symptoms) or malignancy (weight loss, cachexia).
Investigations
The initial work-up combines imaging and targeted biochemistry. Australian MBS item numbers are provided for commonly requested tests.
Risk Stratification / Severity Scoring
Risk is determined by the composite of size, imaging phenotype, and functional status.
Directed Therapy
Surgery is the definitive treatment for functioning tumours and suspected malignancy. Pre-operative optimisation is critical.
Management by Tumour Type
| Diagnosis | Primary Treatment | Key Pre-operative Step |
|---|---|---|
| Phaeochromocytoma | Laparoscopic adrenalectomy | Alpha-blockade (doxazosin) for ≥10–14 days, then beta-blockade if tachyarrhythmic. Volume expansion. |
| Aldosteronoma | Laparoscopic adrenalectomy | Correct hypokalaemia, control BP with spironolactone. |
| Cushing’s / Subclinical Cushing’s | Laparoscopic adrenalectomy (if biochemical cure desired) | Peri-operative stress-dose hydrocortisone (HPA axis suppression likely). |
| Adrenocortical carcinoma | Open en-bloc resection (by specialist surgeon) | Staging, multidisciplinary team discussion. |
Monitoring
For Non-Functioning, Benign-Appearing Adenomas
- Imaging: Repeat non-contrast CT at 6–12 months. If stable (no growth, no change in character), further imaging is typically unnecessary unless new clinical concerns arise.
- Hormonal: Repeat 1 mg ONDST and plasma metanephrines at 12 months. Up to 10% of initially non-functioning adenomas may develop autonomous cortisol secretion over time.
For Post-Surgical Patients
- Phaeochromocytoma: Annual plasma metanephrines for life (risk of recurrence or malignancy).
- Aldosteronoma: Monitor BP and potassium. Assess for resolution of primary aldosteronism.
- Cushing’s: Monitor for adrenal insufficiency and need for glucocorticoid replacement.
Special Populations
Aboriginal and Torres Strait Islander Health Considerations
📚 References
- 1. Fassnacht M, Arlt W, Bancos I, et al. Management of adrenal incidentalomas: European Society of Endocrinology Clinical Practice Guideline in collaboration with the European Network for the Study of Adrenal Tumors. Eur J Endocrinol. 2016;175(2):G1-G34.
- 2. National Institute for Health and Care Excellence (NICE). Adrenal incidentalomas (NG154). 2019.
- 3. Young WF Jr. Clinical practice. The incidentally discovered adrenal mass. N Engl J Med. 2007;356(6):601-610.
- 4. Australian Institute of Health and Welfare (AIHW). Adrenal gland and related conditions. In: Australian Cancer Incidence and Mortality (ACIM) books. 2023.
- 5. Lenders JWM, Duh QY, Eisenhofer G, et al. Pheochromocytoma and paraganglioma: an Endocrine Society clinical practice guideline. J Clin Endocrinol Metab. 2014;99(6):1915-1942.
- 6. Funder JW, Carey RM, Mantero F, et al. The Management of Primary Aldosteronism: Case Detection, Diagnosis, and Treatment: An Endocrine Society Clinical Practice Guideline. J Clin Endocrinol Metab. 2016;101(5):1889-1916.
- 7. Royal Australian College of General Practitioners (RACGP). Management of type 2 diabetes: A handbook for general practice. 2020. (Relevant for comorbidity management).
- 8. The Royal Australian and New Zealand College of Radiologists (RANZCR). Guidelines for the use of imaging in the investigation of adrenal lesions. 2021.
- 9. Australian Government Department of Health. Medicare Benefits Schedule (MBS) Item 66680 - Metanephrines. Accessed 2024.
- 10. Australian Institute of Health and Welfare (AIHW). Aboriginal and Torres Strait Islander health performance framework 2020 summary report. 2020.