📋 Key Information Summary
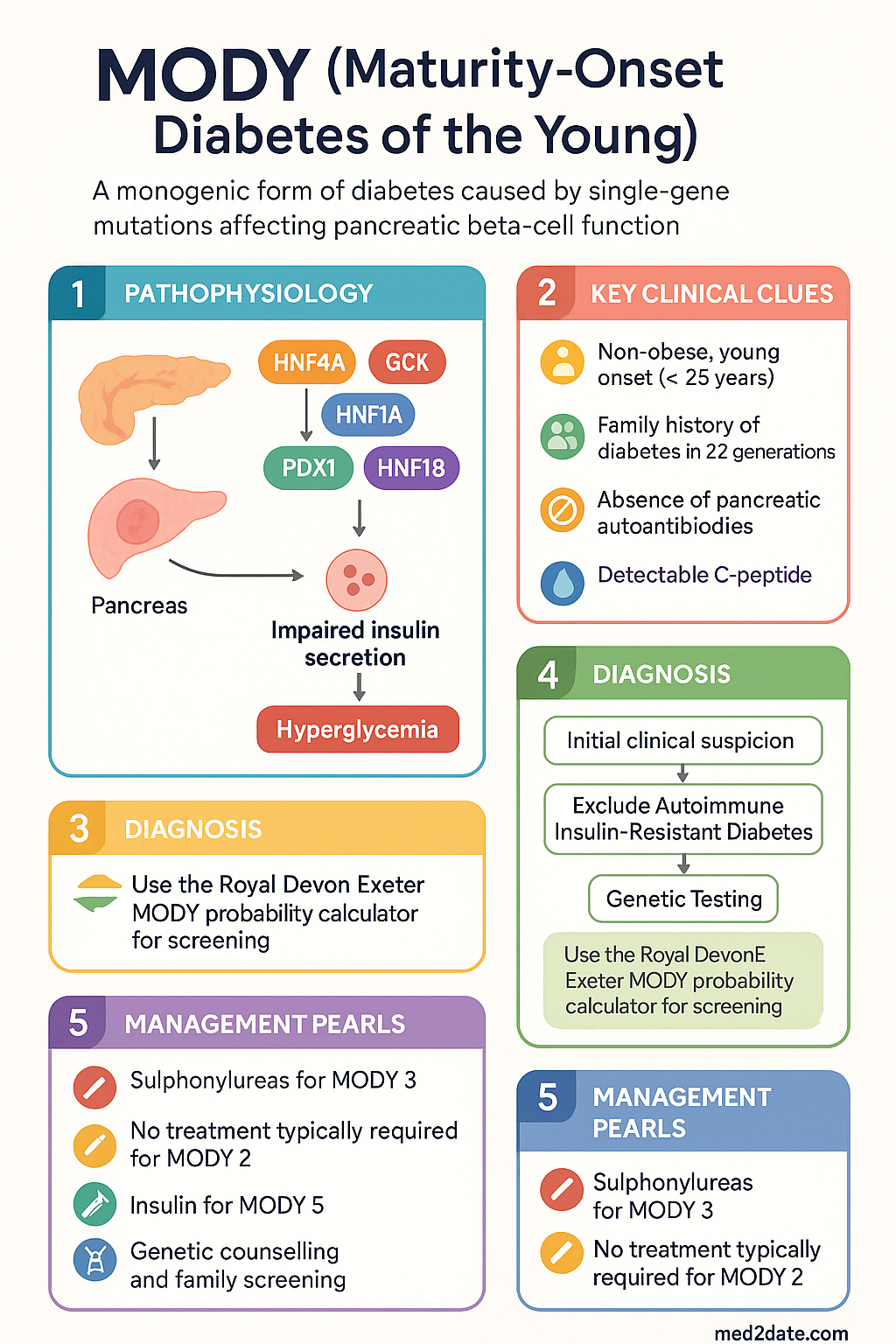
- MODY (Maturity-Onset Diabetes of the Young) is a monogenic form of diabetes caused by single-gene mutations affecting pancreatic beta-cell function; it accounts for 1–5 % of all paediatric and young-adult diabetes.
- MODY is often misdiagnosed as type 1 diabetes mellitus (T1DM) or type 2 diabetes mellitus (T2DM); correct diagnosis changes management in the majority of cases.
- At least 14 subtypes are recognised; MODY 1–6 are the best characterised (HNF4A, GCK, HNF1A, PDX1, HNF1B, NEUROD1).
- MODY 2 (GCK mutations) causes mild, stable fasting hyperglycaemia (5.5–8.0 mmol/L) and usually requires no pharmacological treatment.
- MODY 3 (HNF1A mutations) is the most common subtype in Australia; patients are exquisitely sensitive to low-dose sulphonylureas and this is the preferred therapy.
- MODY 1 (HNF4A) responds similarly to sulphonylureas; MODY 5 (HNF1B) is associated with renal cysts and often requires insulin.
- Genetic testing (targeted gene panel or whole-exome sequencing) is the gold standard for diagnosis; available through Australian public genetics services.
- MODY follows autosomal dominant inheritance — each child of an affected parent has a 50 % chance of inheriting the mutation.
- Key diagnostic clues: non-obese, young onset (<25 years), family history of diabetes in ≥2 generations, absence of pancreatic autoantibodies, detectable C-peptide.
- Correct diagnosis of MODY 3 allows transition from insulin to low-dose sulphonylurea, improving glycaemic control and quality of life.
- HbA1c targets: 6.5 % (48 mmol/mol) or individualised; MODY 2 patients typically have HbA1c < 7.0 % without treatment.
- Cascade genetic testing of first-degree relatives is recommended to identify undiagnosed family members.
🎧 Audio Brief
Introduction & Australian Epidemiology
MODY (Maturity-Onset Diabetes of the Young) is a monogenic form of diabetes mellitus caused by single-gene mutations that impair pancreatic beta-cell development, insulin secretion, or both. Unlike type 1 diabetes mellitus (T1DM), MODY is not autoimmune; unlike type 2 diabetes mellitus (T2DM), it is not primarily driven by insulin resistance. MODY typically presents in adolescents or young adults who are often non-obese and have a strong family history of diabetes spanning multiple generations in an autosomal dominant pattern.
MODY accounts for approximately 1–5 % of all cases of diabetes diagnosed before the age of 25 years. In Australia, MODY is likely underdiagnosed due to its clinical overlap with T1DM and T2DM. A 2018 study from the Royal Melbourne Hospital genetics service estimated that fewer than 10 % of eligible patients are referred for genetic testing. Prevalence estimates from European and North American registries suggest roughly 68–100 cases per million population; Australian data are limited but the condition is recognised at major tertiary centres and through the Australian Genomics Health Alliance.
Accurate diagnosis of MODY is clinically important because it determines prognosis, guides therapy (particularly the use of sulphonylureas in MODY 3), informs family screening, and may allow cessation of unnecessary insulin therapy. The three most common subtypes — MODY 3 (HNF1A), MODY 2 (GCK), and MODY 1 (HNF4A) — together account for over 80 % of genetically confirmed cases worldwide.
Genetics & Types (MODY 1–6)
MODY follows autosomal dominant inheritance with high penetrance. Each child of an affected parent carries a 50 % risk of inheriting the pathogenic variant. The condition is caused by heterozygous loss-of-function mutations in genes critical for beta-cell development, glucose sensing, or insulin transcription and secretion. At least 14 subtypes are now recognised; the first six are the best characterised and most clinically relevant.
| Subtype | Gene | Prevalence | Mechanism | Key Features |
|---|---|---|---|---|
| MODY 1 | HNF4A | ~5 % | Impaired insulin transcription & secretion | Progressive hyperglycaemia; neonatal macrosomia and transient neonatal hypoglycaemia; responds to sulphonylureas |
| MODY 2 | GCK | ~30–50 % | Defective glucose sensing (glucokinase) | Mild stable fasting hyperglycaemia (5.5–8.0 mmol/L); HbA1c typically 5.8–7.6 %; usually no treatment required |
| MODY 3 | HNF1A | ~30–50 % | Reduced beta-cell transcription factor function | Most common subtype; progressive hyperglycaemia; renal glycosuria (low renal threshold); exquisitely sensitive to sulphonylureas |
| MODY 4 | PDX1 (IPF1) | <1 % | Impaired pancreas development & insulin gene expression | Rare; may cause pancreatic agenesis in homozygotes; heterozygotes develop late-onset diabetes |
| MODY 5 | HNF1B | ~5–7 % | Renal cysts and diabetes syndrome (RCAD) | Renal cystic disease, renal malformations, pancreatic hypoplasia; often requires insulin; renal function monitoring essential |
| MODY 6 | NEUROD1 | <1 % | Impaired insulin gene transcription & neuronal development | Very rare; may have neurological features; responds to sulphonylureas or insulin |
Clinical Features & Diagnosis
When to Suspect MODY
MODY should be considered in any patient with diabetes who does not clearly fit the typical T1DM or T2DM profile. The following clinical features raise the probability of MODY:
- Diagnosis before age 25 years (though MODY 1 and 3 may present later)
- Non-obese (BMI < 25 kg/m²) with no features of metabolic syndrome
- Family history of diabetes in ≥ 2 consecutive generations (autosomal dominant pattern)
- Negative pancreatic autoantibodies (GAD65, IA-2, ZnT8)
- Preserved C-peptide secretion (fasting C-peptide > 200 pmol/L, or stimulated > 600 pmol/L)
- No history of diabetic ketoacidosis (DKA)
- Mild, stable hyperglycaemia without significant glycaemic variability (particularly MODY 2)
- Renal glycosuria with normal blood glucose (suggestive of MODY 3/HNF1A)
- Neonatal macrosomia followed by childhood-onset diabetes (suggestive of MODY 1/HNF4A)
- Renal cysts or urogenital malformations with diabetes (suggestive of MODY 5/HNF1B)
Diagnostic Pathway
The diagnostic workup for suspected MODY follows a stepwise approach:
Differentiation from T1DM and T2DM
Distinguishing MODY from T1DM and T2DM is essential for appropriate management. The table below summarises key distinguishing features.
| Feature | T1DM | T2DM | MODY |
|---|---|---|---|
| Age of onset | Any age; peaks in childhood/adolescence | Usually > 40 years (increasingly younger) | Typically < 25 years (some subtypes later) |
| BMI | Usually normal | Usually overweight/obese | Usually normal |
| Family history pattern | Polygenic; ~10 % have FHx | Polygenic; strong FHx common | Autosomal dominant; ≥ 2 generations affected |
| Autoantibodies (GAD, IA-2) | Positive (85–90 %) | Negative | Negative |
| C-peptide | Low/undetectable | Normal or elevated | Preserved (detectable, often normal) |
| DKA risk | High | Low (unless severe illness) | Very low (except MODY 5 with pancreatic atrophy) |
| Insulin resistance | Absent initially | Central feature | Absent |
| Metabolic syndrome | No | Common | No |
| HbA1c at diagnosis | Often markedly elevated (> 8.5 %) | Variable (6.5–10 %) | MODY 2: 5.8–7.6 %; MODY 3: variable, progressive |
| Treatment response | Insulin essential | Lifestyle + metformin ± other agents | MODY 2: usually none; MODY 3: sulphonylureas first-line |
Management — Sulphonylureas for MODY 2 & 3
Management of MODY depends on the subtype. Accurate genetic diagnosis directly informs pharmacotherapy.
MODY 2 (GCK) — Management
- Monitoring: Annual HbA1c; fasting glucose self-monitoring not routinely required
- During pregnancy: Insulin may be required if foetal growth is affected (foetal MODY 2 genotype determines foetal hyperglycaemia risk)
- Patient education: Reassurance that the condition is benign; avoid unnecessary dietary restriction or medication
MODY 3 (HNF1A) — Management
MODY 3 patients are exquisitely sensitive to sulphonylureas — they require doses approximately 25–50 % of those used in T2DM. Sulphonylureas are first-line therapy and remain effective long-term.
MODY 1 (HNF4A) — Management
Similar to MODY 3, MODY 1 patients respond well to sulphonylureas. Therapy typically starts at low doses and is titrated to glycaemic targets. Insulin may be required in later life as beta-cell function declines.
MODY 5 (HNF1B) — Management
MODY 5 is frequently associated with pancreatic atrophy or hypoplasia, resulting in significant insulin deficiency. Most patients require insulin therapy from diagnosis. Sulphonylureas are generally ineffective due to inadequate beta-cell mass. Renal function monitoring is essential given the association with renal cystic disease.
Glycaemic Targets
| Parameter | Target | Notes |
|---|---|---|
| HbA1c | ≤ 6.5 % (48 mmol/mol) | Individualise; MODY 2 patients typically < 7.0 % without treatment |
| Fasting glucose | 4.0–7.0 mmol/L | MODY 2 patients may run 5.5–8.0 mmol/L — this is acceptable |
| Postprandial glucose | < 10.0 mmol/L | Particularly relevant for MODY 3 on sulphonylureas |
Special Populations
Aboriginal and Torres Strait Islander Health Considerations
📚 References
- 1. Shields BM, Hicks S, Shepherd MH, et al. Maturity-onset diabetes of the young (MODY): how many cases are we missing? Diabetologia. 2010;53(12):2504–2508.
- 2. Hattersley AT, Patel KA. Precision diabetes: learning from monogenic diabetes. Diabetologia. 2017;60(5):769–777.
- 3. Naylor RN, Greeley SAW, Bell GI, Philipson LH. Genetics and pathophysiology of neonatal diabetes mellitus. J Clin Invest. 2011;121(12):4513–4521.
- 4. McDonald TJ, Ellard S. Maturity onset diabetes of the young: identification and diagnosis. Ann Clin Biochem. 2013;50(Pt 5):403–415.
- 5. Pearson ER, Flechtner I, Njølstad PR, et al. Switching from insulin to oral sulfonylureas in patients with diabetes due to Kir6.2 mutations. N Engl J Med. 2006;355(5):467–477.
- 6. Bacon S, Kyithar MP, Rizvi SR, et al. Successful maintenance on sulphonylurea therapy and low diabetes complication rates in a HNF1A-MODY cohort. Diabet Med. 2016;33(7):976–984.
- 7. Australian Institute of Health and Welfare (AIHW). Diabetes: Australian Facts. Canberra: AIHW; 2023.
- 8. Royal Australian and New Zealand College of Obstetricians and Gynaecologists (RANZCOG). Management of Pre-existing Diabetes in Pregnancy (C-Obs 60). Melbourne: RANZCOG; 2021.
- 9. The Royal Australian College of General Practitioners (RACGP). General Practice Management of Type 2 Diabetes: 2016–2018. East Melbourne: RACGP; 2016.
- 10. National Health and Medical Research Council (NHMRC). National Evidence-Based Guideline: Diagnosis, Prevention and Management of Chronic Kidney Disease in Type 2 Diabetes. Canberra: NHMRC; 2015.
- 11. Johansson BB, Irgens HU, Molnes J, et al. Targeted next-generation sequencing reveals MODY in up to 6.5% of antibody-negative diabetes cases listed in the Norwegian Childhood Diabetes Registry. Diabetologia. 2017;60(4):625–635.
- 12. Royal Devon and Exeter NHS Foundation Trust. MODY Probability Calculator. Available from: https://www.diabetesgenes.org/exeter-mody-probability-calculator.