📋 Key Information Summary
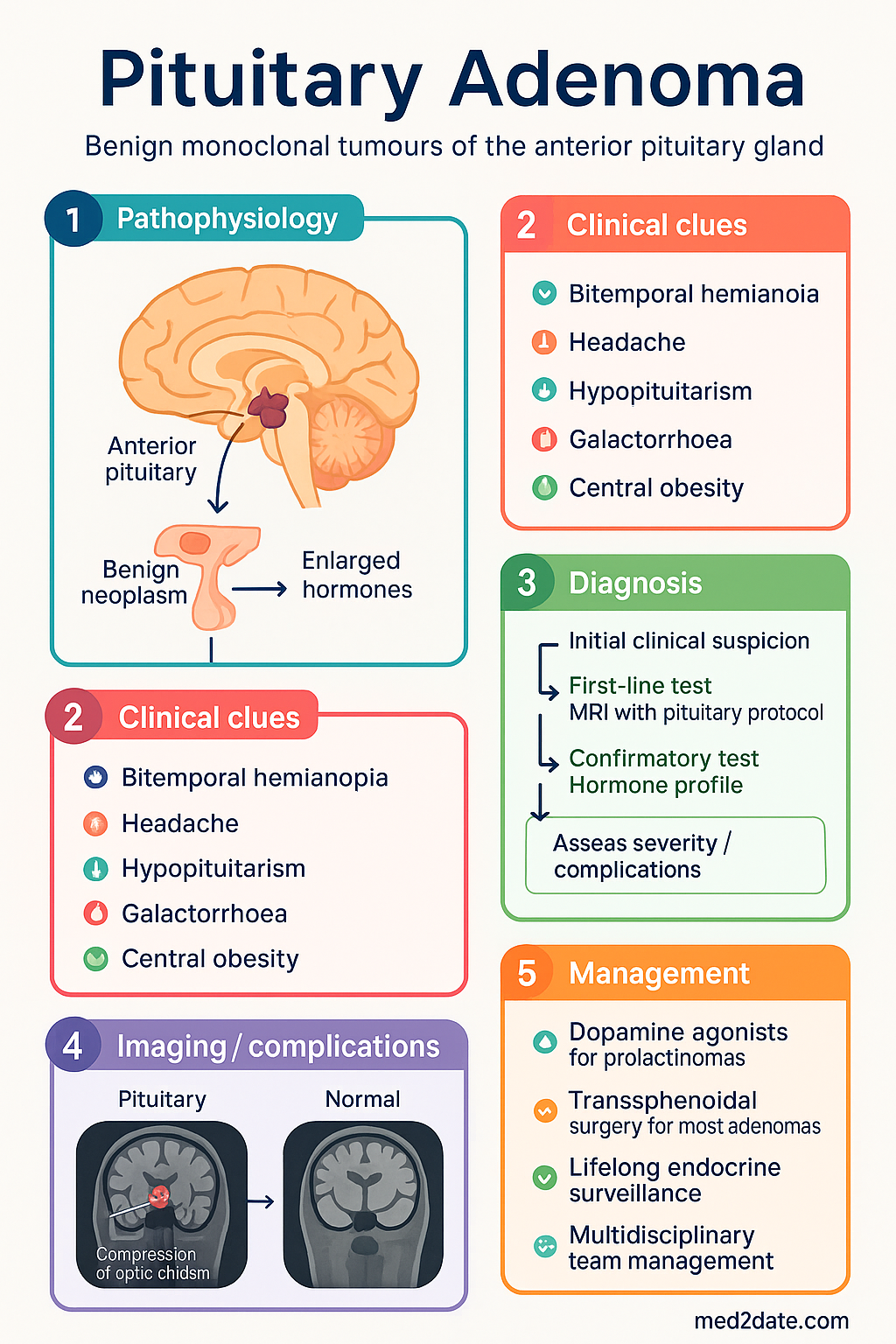
- Pituitary adenomas are benign monoclonal tumours of the anterior pituitary gland, classified by size (microadenoma <10 mm, macroadenoma ≥10 mm) and functional status (secretory vs. non-functioning).
- Prevalence on high-resolution MRI is approximately 10–15%, but clinically significant tumours are less common, accounting for ~15% of intracranial neoplasms.
- Mass effects from macroadenomas include bitemporal hemianopia, headache, and hypopituitarism due to stalk compression.
- Prolactinoma is the most common secretory adenoma (40–60%); first-line medical therapy is a dopamine agonist (cabergoline).
- Acromegaly (GH excess) and Cushing's disease (ACTH excess) require multidisciplinary management, with transsphenoidal surgery as first-line for most.
- Pituitary function testing (prolactin, IGF-1, cortisol, thyroid/sex hormones, α-subunit) is essential for all macroadenomas and symptomatic microadenomas.
- MRI with dedicated pituitary protocol (gadolinium-enhanced, 1–1.5T minimum) is the gold-standard imaging investigation.
- Visual field assessment (formal perimetry) is mandatory for any adenoma abutting or compressing the optic chiasm.
- Management is stratified: prolactinomas → medical; most other adenomas → surgery (endoscopic endonasal transsphenoidal); recurrent/residual disease → radiotherapy or medical therapy.
- Lifelong endocrine surveillance is required post-treatment for recurrence, hypopituitarism, and comorbidities (cardiovascular, metabolic).
- Pregnancy planning is critical in fertile women with prolactinomas or Cushing's disease, requiring pre-conception medication adjustment and monitoring.
- Aboriginal and Torres Strait Islander peoples may face delayed diagnosis and barriers to specialist care; culturally safe, accessible services are essential.
🎧 Audio Brief
Introduction & Australian Epidemiology
Pituitary adenomas are benign neoplasms arising from the anterior pituitary gland (adenohypophysis). They represent approximately 10–15% of intracranial neoplasms and are the most common sellar mass. Autopsy and radiological (MRI) studies suggest a prevalence of 10–15%, though the majority are incidental, non-functioning microadenomas without clinical significance.
In Australia, the incidence of clinically relevant pituitary adenomas is estimated at 3–5 per 100,000 population per year. Data from the Australian Institute of Health and Welfare (AIHW) and specialist centres (e.g., Royal Melbourne Hospital, Westmead Hospital) indicate that prolactinomas account for 40–60% of all secretory adenomas, followed by non-functioning adenomas (15–30%), GH-secreting adenomas (acromegaly, 10–15%), and ACTH-secreting adenomas (Cushing's disease, 5–10%). Thyroid-stimulating hormone (TSH)-secreting adenomas are rare (<1%).
Management requires a multidisciplinary pituitary team including an endocrinologist, neurosurgeon, neuroradiologist, ophthalmologist, and radiation oncologist. Early recognition and appropriate referral are crucial to prevent irreversible complications such as hypopituitarism, visual loss, and the metabolic and cardiovascular consequences of hormonal hypersecretion.
Classification & Pathophysiology
Classification by Size
- Microadenoma: <10 mm in diameter. Typically confined to the sella turcica; rarely cause mass effects.
- Macroadenoma: ≥10 mm in diameter. May extend suprasellarly, laterally into cavernous sinuses, or inferiorly into sphenoid sinus. Responsible for most mass-effect symptoms.
- Giant adenoma: >40 mm; rare but associated with higher surgical morbidity.
Classification by Function
| Type | Hormone Excess | Proportion | Key Pathophysiology |
|---|---|---|---|
| Prolactinoma | Prolactin | 40–60% | Direct dopamine inhibition by tumour; galactorrhoea, hypogonadism. |
| Somatotrophinoma | Growth Hormone (GH) | 10–15% | GH → hepatic IGF-1 excess; acral enlargement, metabolic dysfunction. |
| Corticotrophinoma | ACTH | 5–10% | ACTH drives adrenal cortisol hypersecretion; central obesity, hypertension. |
| Non-functioning adenoma | None (or subclinical α-subunit) | 15–30% | Mass effect; often macroadenoma at presentation. |
| Thyrotrophinoma | TSH | <1% | Inappropriate TSH secretion causing central hyperthyroidism. |
Histopathological Classification (WHO 2022)
The modern WHO classification emphasises immunohistochemistry for pituitary transcription factors (PIT-1, T-PIT, SF-1) and hormone production, moving away from the term "adenoma" to "pituitary neuroendocrine tumour (PitNET)" in some contexts. Prognostic markers include mitotic count, Ki-67 proliferation index (>3% suggests potential for more aggressive behaviour), and p53 expression.
Clinical Features (Mass Effect, Hormonal)
Mass Effect Symptoms (Macroadenomas)
- Visual field defects: Classically bitemporal hemianopia due to chiasmal compression. May progress to blindness. Formal perimetry is essential.
- Headache: Often frontal or retro-orbital due to dural stretching. Not always correlated with tumour size.
- Cranial nerve palsies: Diplopia from III, IV, VI nerve involvement if lateral extension into cavernous sinus.
- Apoplexy: Sudden haemorrhage or infarction within the adenoma. Presents with acute headache, visual loss, ophthalmoplegia, and potential cardiovascular collapse (adrenal crisis). Requires emergency high-dose glucocorticoids and neurosurgical assessment.
- Hypopituitarism: Compression of normal pituitary tissue and stalk. Sequence of loss typically: GH > FSH/LH > TSH > ACTH. Presents with fatigue, amenorrhoea, erectile dysfunction, cold intolerance.
Syndromes of Hormonal Excess
Investigations (MRI Pituitary, Hormone Profile)
Biochemical / Hormonal Profile
Essential for all macroadenomas and symptomatic microadenomas. Perform in a specialised endocrine laboratory.
Radiology
Ophthalmology
Management (Surgery, Radiotherapy, Medical)
General Principles
Management is determined by adenoma type, size, invasiveness, and patient factors. All patients should be discussed at a multidisciplinary pituitary tumour board (neuroendocrinology, neurosurgery, neuroradiology, radiation oncology, ophthalmology).
Medical Therapy
Surgical Therapy
Endoscopic Endonasal Transsphenoidal Surgery (EETS) is the gold-standard approach for most pituitary adenomas. Performed by a specialised skull-base neurosurgeon.
- Indications: All non-prolactinoma secretory adenomas (first-line), non-functioning adenomas causing mass effect, prolactinomas resistant/intolerant to dopamine agonists, pituitary apoplexy with visual compromise.
- Remission rates: Microadenomas 70–90%, Macroadenomas 40–70% (higher for experienced surgeons). Higher for invasive tumours.
- Complications: CSF leak (2–5%), new hypopituitarism (5–15%), diabetes insipidus (transient 10–20%, permanent 1–2%), meningitis, vascular injury (<1%).
- Peri-operative management: Stress-dose hydrocortisone (100 mg IV at induction) if ACTH deficient. Monitor sodium closely for DI (first 5–10 days).
Radiotherapy
Used for residual or recurrent tumour not controlled by surgery/medical therapy. Goal is tumour control, not rapid hormone normalisation (may take years).
| Modality | Indication | Key Details |
|---|---|---|
| Stereotactic Radiosurgery (SRS) (Gamma Knife, CyberKnife) |
Focal residual/recurrent adenoma <3 cm, ≥3–5 mm from optic chiasm. | Single high-dose fraction. 5-year tumour control >90%. Hypopituitarism risk 20–40% at 10 years. |
| Fractionated Radiotherapy (EBRT) | Larger, invasive, or recurrent tumours close to optic apparatus. | Typically 45–50 Gy in 25 fractions. Slower biochemical response. Higher long-term hypopituitarism risk (~50–80%). |
Monitoring & Follow-up
Post-operative / Post-treatment
Special Populations
Aboriginal and Torres Strait Islander peoples may experience pituitary adenomas but face significant barriers to timely diagnosis and specialist care. These include geographical remoteness, reduced access to endocrinology and neurosurgery services, and culturally unsafe healthcare environments.
📚 References
- 1. Melmed S, et al. Diagnosis and Treatment of Hyperprolactinemia: An Endocrine Society Clinical Practice Guideline. J Clin Endocrinol Metab. 2011;96(2):273-88.
- 2. Katznelson L, et al. Acromegaly: An Endocrine Society Clinical Practice Guideline. J Clin Endocrinol Metab. 2014;99(11):3933-51.
- 3. Nieman LK, et al. Treatment of Cushing's Syndrome: An Endocrine Society Clinical Practice Guideline. J Clin Endocrinol Metab. 2015;100(8):2807-31.
- 4. Freda PU, et al. Pituitary Incidentaloma: An Endocrine Society Clinical Practice Guideline. J Clin Endocrinol Metab. 2011;96(4):894-904.
- 5. Australian Institute of Health and Welfare (AIHW). Brain and other central nervous system cancer. Cancer Series. 2023.
- 6. The Royal Australian and New Zealand College of Ophthalmologists (RANZCO). Guidelines for the management of visual field defects due to pituitary adenomas. 2020.
- 7. Chanson P, et al. European Society of Endocrinology (ESE) Clinical Practice Guideline on the management of aggressive pituitary tumours and carcinomas. Eur J Endocrinol. 2018;178(1):G1-G24.
- 8. Fleseriu M, et al. Consensus on diagnosis and management of Cushing's disease: a guideline update. Lancet Diabetes Endocrinol. 2021;9(12):847-875.
- 9. Australian Government Department of Health. PBS Schedule: Cabergoline, Octreotide. Accessed 2024.
- 10. Asa SL, et al. Overview of the 2022 WHO Classification of Pituitary Tumors. Endocr Pathol. 2022;33(1):6-26.