📋 Key Information Summary
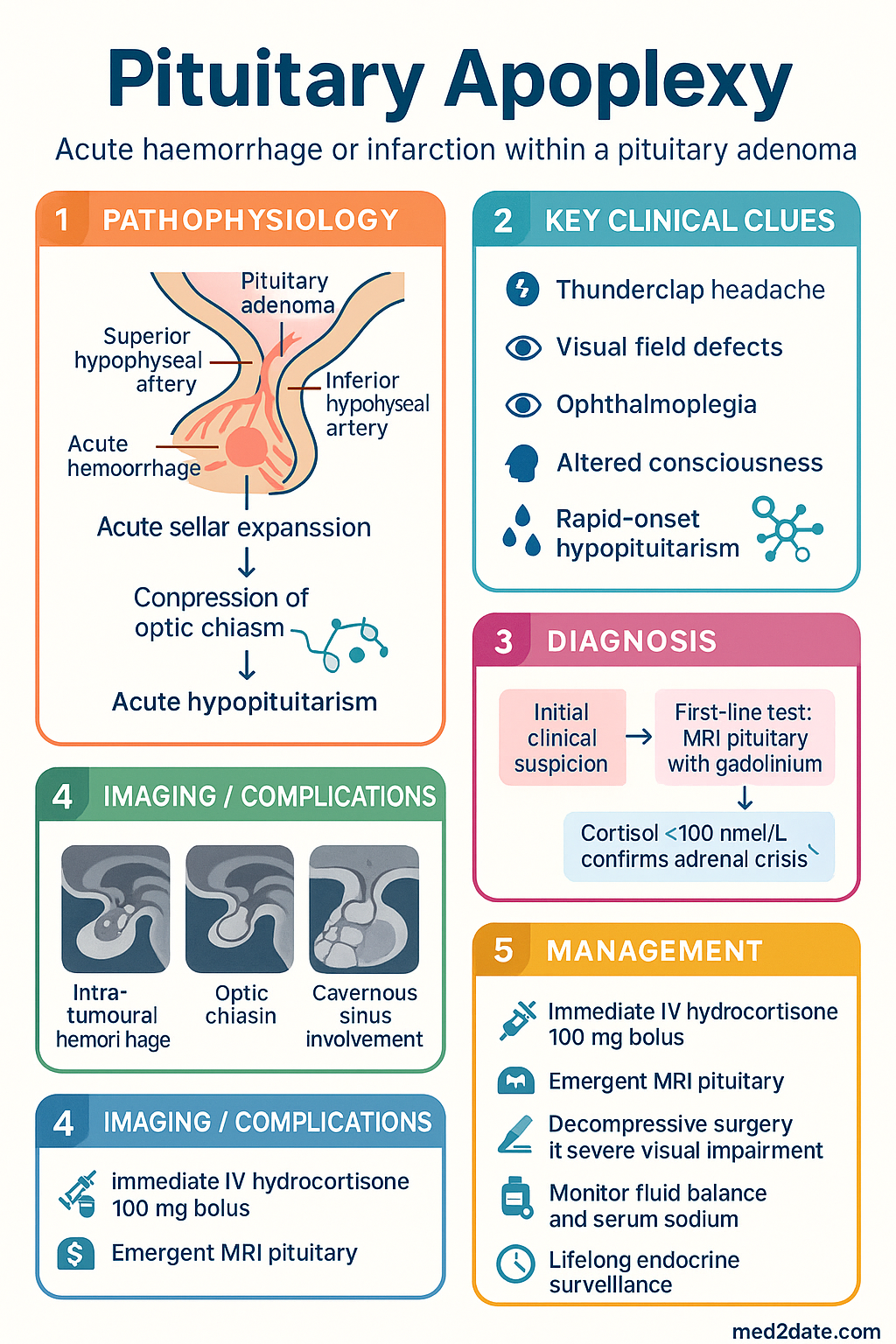
- Pituitary apoplexy is a neuroendocrine emergency caused by acute haemorrhage or infarction within a pre-existing pituitary adenoma, occurring in approximately 0.6–10% of all pituitary adenomas.
- Severe sudden-onset headache ("thunderclap headache") is the cardinal symptom, often accompanied by visual field defects, ophthalmoplegia, altered consciousness, and rapid-onset hypopituitarism.
- Immediate IV hydrocortisone 100 mg bolus is lifesaving and must be administered before diagnostic confirmation — do not delay steroids for MRI.
- Cortisol <100 nmol/L in the acute setting confirms adrenal crisis and mandates urgent glucocorticoid replacement.
- Emergent MRI pituitary with gadolinium is the investigation of choice; CT may show haemorrhage but has lower sensitivity for infarction.
- Decompressive transsphenoidal surgery should be performed within 7 days for patients with severe visual impairment, progressive visual deterioration, or declining consciousness.
- Mild cases (no visual compromise, intact consciousness) may be managed conservatively with close monitoring in an HDU setting.
- All patients require complete anterior pituitary hormone panel (TSH/fT4, cortisol, LH/FSH, testosterone/oestradiol, IGF-1, prolactin) and posterior pituitary function assessment post-event.
- Precipitants include dynamic pituitary function testing (GnRH analogue stimulation), anticoagulation, pregnancy, and raised intracranial pressure.
- Diabetes insipidus may develop acutely or 5–10 days post-surgery; monitor strict fluid balance and serum sodium in all patients.
- Aboriginal and Torres Strait Islander patients may have reduced access to specialist neurosurgical and endocrinological care, particularly in remote regions; initiate early retrieval coordination.
- Lifelong endocrine surveillance and hormone replacement therapy are required for most patients following pituitary apoplexy.
🎧 Audio Brief
Introduction & Australian Epidemiology
Pituitary apoplexy is a clinical emergency caused by acute haemorrhage or infarction within a pituitary adenoma, resulting in rapid expansion of the sellar mass, compression of adjacent neural structures, and abrupt pituitary hormone deficiency. The syndrome may also rarely occur in non-adenomatous pituitary tissue, during pregnancy (Sheehan syndrome), or as a consequence of pharmacological or radiological interventions.
The estimated incidence is 6.2 per 100,000 person-years among patients with known pituitary adenomas. Clinically apparent apoplexy occurs in 2–12% of all pituitary adenomas, though histopathological evidence of haemorrhage or infarction is found in up to 25% of surgical specimens. The true incidence in the Australian population is not well established; however, data from the Australian Pituitary Tumour Registries and tertiary referral centres (Royal Melbourne Hospital, Westmead Hospital, St Vincent's Hospital Sydney) suggest approximately 80–120 clinically significant presentations per year nationally.
The condition has a male predominance (M:F ≈ 2:1), likely reflecting the higher prevalence of non-functioning macroadenomas in men. Presentation is most common in the fifth and sixth decades. Non-functioning adenomas account for the majority of cases, though prolactinomas, GH-secreting, and ACTH-secreting adenomas may also undergo apoplexy.
Pathophysiology & Precipitants
Mechanism
Pituitary adenomas are particularly vulnerable to haemorrhage and infarction due to their unique vascular architecture. The pituitary gland is supplied by the superior and inferior hypophyseal arteries, with adenomas relying on a fragile, sinusoidal capillary network. Rapid tumour expansion outstrips blood supply, creating zones of ischaemia that may progress to infarction or haemorrhagic transformation.
Two pathological processes underlie apoplexy:
- Haemorrhagic apoplexy: Intra-tumoural haemorrhage causing rapid sellar expansion, compression of the optic chiasm, cavernous sinus, and hypothalamus. Gross haemorrhage is identified in approximately 50% of cases.
- Ischaemic (infarctive) apoplexy: Thrombosis or vasospasm within the tumour vasculature leading to coagulative necrosis, oedema, and secondary mass effect. This variant may have a more insidious onset.
Recognised Precipitants
| Precipitant | Mechanism | Clinical Context |
|---|---|---|
| Dynamic pituitary function testing | GnRH analogue stimulation (e.g., triptorelin) causes rapid tumour enlargement | Growth hormone stimulation testing in children with pituitary adenoma |
| Anticoagulation | Haemorrhagic transformation of pre-existing ischaemic focus | Heparin, warfarin, DOACs; post-cardiac surgery |
| Pregnancy | Oestrogen-mediated lactotroph hyperplasia; haemodynamic changes | Peripartum period; Sheehan syndrome (postpartum pituitary necrosis) |
| Raised intracranial pressure | Venous congestion of pituitary sinusoidal system | Lumbar puncture, Valsalva, mechanical ventilation with high PEEP |
| Radiotherapy | Vascular endothelial damage; delayed vasculopathy | Months to years after stereotactic or fractionated radiotherapy |
| Dopamine agonist initiation/withdrawal | Rapid tumour shrinkage with infarction, or rebound expansion on withdrawal | Cabergoline initiation in macroprolactinoma |
| Diabetes mellitus | Microvascular disease of pituitary vasculature | Independent risk factor in observational studies |
| Head trauma | Direct vascular injury or shearing of stalk vessels | Road traffic accidents, falls |
Sequence of Pathological Events
The acute expansion of the pituitary fossa contents occurs over minutes to hours, producing a cascade of compressive effects: first on the optic chiasm (bitemporal hemianopia), then the cavernous sinus (cranial nerve III, IV, VI palsies), and finally the hypothalamus and third ventricle (altered consciousness, autonomic instability, hydrocephalus). Concurrently, destruction of functioning pituitary tissue causes acute hypopituitarism, with ACTH/cortisol deficiency being the most immediately life-threatening.
Clinical Features
Classic Triad
- Severe sudden-onset headache (85–97%)
- Visual impairment (60–80%)
- Ophthalmoplegia / cranial nerve palsy (40–70%)
Severe Headache
The headache of pituitary apoplexy is typically retro-orbital or frontal, of sudden onset ("thunderclap"), severe, and unremitting. It may be bilateral or unilateral and is often described as the "worst headache of my life." Nausea and vomiting occur in approximately 70% of cases due to meningeal irritation from subarachnoid haemorrhage or raised intracranial pressure. Neck stiffness may be present, mimicking meningitis or subarachnoid haemorrhage.
Visual Loss & Field Defects
Visual impairment results from compression of the optic chiasm and/or optic nerves. Classical findings include:
- Bitemporal hemianopia: The hallmark visual field defect, occurring in approximately 50–60% of cases
- Unilateral or bilateral visual acuity loss: Ranging from mild blurring to complete blindness
- Afferent pupillary defect (RAPD): Indicates significant unilateral optic nerve compression
- Papilloedema: May be present with raised intracranial pressure
Patients with pre-existing bitemporal hemianopia from a known macroadenoma may not report new visual symptoms; therefore, formal bedside confrontation testing and pupillary reflex assessment are essential in all presentations.
Ophthalmoplegia & Cranial Nerve Palsies
Lateral extension of haemorrhage or oedema into the cavernous sinus compresses cranial nerves traversing this structure:
- CN III (oculomotor): Ptosis, dilated pupil, "down and out" eye — most common
- CN IV (trochlear): Diplopia on downward and inward gaze
- CN VI (abducens): Lateral rectus palsy, horizontal diplopia
- CN V₁ (ophthalmic): Reduced corneal sensation, forehead numbness
Hypopituitarism
Acute anterior pituitary failure develops rapidly, with the following deficiency pattern and approximate frequency:
| Hormone Deficient | Frequency | Acute Consequences |
|---|---|---|
| ACTH → Cortisol | ~70% | Adrenal crisis: hypotension, shock, hyponatraemia, hypoglycaemia — potentially fatal |
| TSH → Thyroid | ~55% | Secondary hypothyroidism (rarely acute; do not replace until cortisol replaced) |
| LH/FSH → Gonadal | ~75% | Hypogonadism: rarely acutely life-threatening |
| GH | ~80% | Hypoglycaemia (especially in children); rarely acute concern in adults |
| ADH (posterior pituitary) | ~3–5% acutely | Diabetes insipidus: polyuria, polydipsia, hypernatraemia |
| Prolactin | ~50% (or ↑ from stalk effect) | Lactation failure in postpartum women |
Investigations
Immediate Bedside & Laboratory
Neuroimaging
Formal Visual Assessment
Urgent ophthalmological assessment with formal visual field testing (Humphrey or Goldmann perimetry) should be arranged, though bedside confrontation testing and pupillary assessment must not be delayed. Documentation of baseline visual function is critical for surgical decision-making.
Lumbar Puncture
Management
Immediate Management (First 0–2 Hours)
The following steps should be initiated simultaneously in the emergency department:
Steroid Therapy — Detailed Regimen
Surgical Management
Transsphenoidal decompression (TSS) is the standard surgical approach. Surgical timing and indications remain debated, but the following evidence-based thresholds are used in Australian neurosurgical centres:
Key surgical considerations in Australia:
- Surgery is performed at designated pituitary neurosurgical centres (Royal Melbourne, Westmead, St Vincent's Sydney, Royal Adelaide, Royal Brisbane & Women's, Sir Charles Gairdner Perth)
- Endoscopic endonasal transsphenoidal approach is standard; craniotomy reserved for unusual anatomy or lateral extension
- Pre-operative steroid therapy must be optimised — hydrocortisone 100 mg IV at induction
- Intra-operative CSF leak may require lumbar drain placement
- Inter-hospital retrieval via RFDS or state retrieval services for rural/remote patients
Management of Diabetes Insipidus
Diabetes insipidus occurs in approximately 3–5% acutely but may develop 5–10 days post-surgery in up to 20% of cases. Monitor strict fluid balance and serum sodium daily.
Long-Term Hormone Replacement
Following acute stabilisation, formal pituitary function reassessment at 6–12 weeks determines long-term replacement needs. Approximately 80% of patients require lifelong glucocorticoid replacement; 60–70% require thyroid hormone replacement; 50–60% require gonadal hormone replacement; and GH replacement may be indicated in confirmed severe GH deficiency.
Supportive & Adjunctive Measures
- VTE prophylaxis: Mechanical prophylaxis (TED stockings, intermittent pneumatic compression) immediately; pharmacological prophylaxis (enoxaparin 40 mg SC daily) once haemostasis confirmed — usually 24–48 hours post-surgery
- Analgesia: Paracetamol 1 g QDS PO/IV; avoid NSAIDs if coagulopathy or recent haemorrhage
- Anti-emetics: Ondansetron 4 mg IV PRN
- Glucose monitoring: BSL 4–6 hourly during acute phase — hypoglycaemia is a feature of cortisol deficiency
- Steroid emergency card: Issue MedicAlert bracelet and adrenal crisis information card prior to discharge
Monitoring
Acute Phase (0–7 Days)
Subacute & Long-Term Follow-Up
- 6 weeks: Formal pituitary function reassessment (full anterior panel + cortisol day curve). Repeat MRI pituitary to assess residual tumour.
- 3 months: Ophthalmological review with formal perimetry. GH stimulation testing (insulin tolerance test or glucagon stimulation test) if other axes deficient.
- 6–12 months: Annual MRI surveillance for residual/recurrent adenoma. Annual pituitary blood panel. Bone density (DEXA) if hypogonadal or on long-term steroids.
- Ongoing: Lifelong annual endocrine review. MedicAlert registration. Sick-day steroid education reinforcement at each visit.
Special Populations
Aboriginal and Torres Strait Islander Health Considerations
📚 References
- 1. Briet C, Salenave S, Bonneville JF, Laws ER, Chanson P. Pituitary apoplexy. Endocrine Reviews. 2015;36(6):622–645.
- 2. Rajasekaran S, Vanderpump M, Baldeweg S, et al. UK guidelines for the management of pituitary apoplexy. Clinical Endocrinology. 2011;74(1):9–20.
- 3. Glezer A, Bronstein MD. Pituitary apoplexy: pathophysiology, diagnosis and management. Archives of Endocrinology and Metabolism. 2015;59(3):259–264.
- 4. Singh TD, Bydon JB, Mandrekar JN, et al. Pituitary apoplexy: a nationwide study of 90-day readmissions. Pituitary. 2017;20(3):324–330.
- 5. Ayuk J, McGregor EJ, Mitchell RD, Gittoes NJL. Acute management of pituitary apoplexy — surgery or conservative management? Clinical Endocrinology. 2004;61(6):747–752.
- 6. Randeva HS, Schoebel J, Byrne J, Esiri M, Adams CBT, Wass JAH. Classical pituitary apoplexy: clinical features, management and outcome. Clinical Endocrinology. 1999;51(2):181–188.
- 7. Australian Institute of Health and Welfare (AIHW). Aboriginal and Torres Strait Islander health performance framework 2020 summary report. Canberra: AIHW; 2020.
- 8. Grossman A, Besser GM. Anterior pituitary failure. In: De Groot LJ, Chrousos G, Dungan K, et al., eds. Endotext. South Dartmouth, MA: MDText.com, Inc.; 2023.
- 9. Royal Australasian College of Physicians. Endocrinology advanced training curriculum. Sydney: RACP; 2022.
- 10. Moller-Goede DL, Brandle M, Landau K, Bernays RL, Schmid C. Pituitary apoplexy: re-evaluation of treatment. Journal of Neurosurgery. 2011;114(1):154–160.
- 11. Semple PL, Webb MK, de Villiers JC, Laws ER Jr. Pituitary apoplexy. Neurosurgery. 2005;56(1):65–73.
- 12. National Health and Medical Research Council (NHMRC). National statement on ethical conduct in human research. Canberra: NHMRC; 2023 (updated).