📋 Key Information Summary
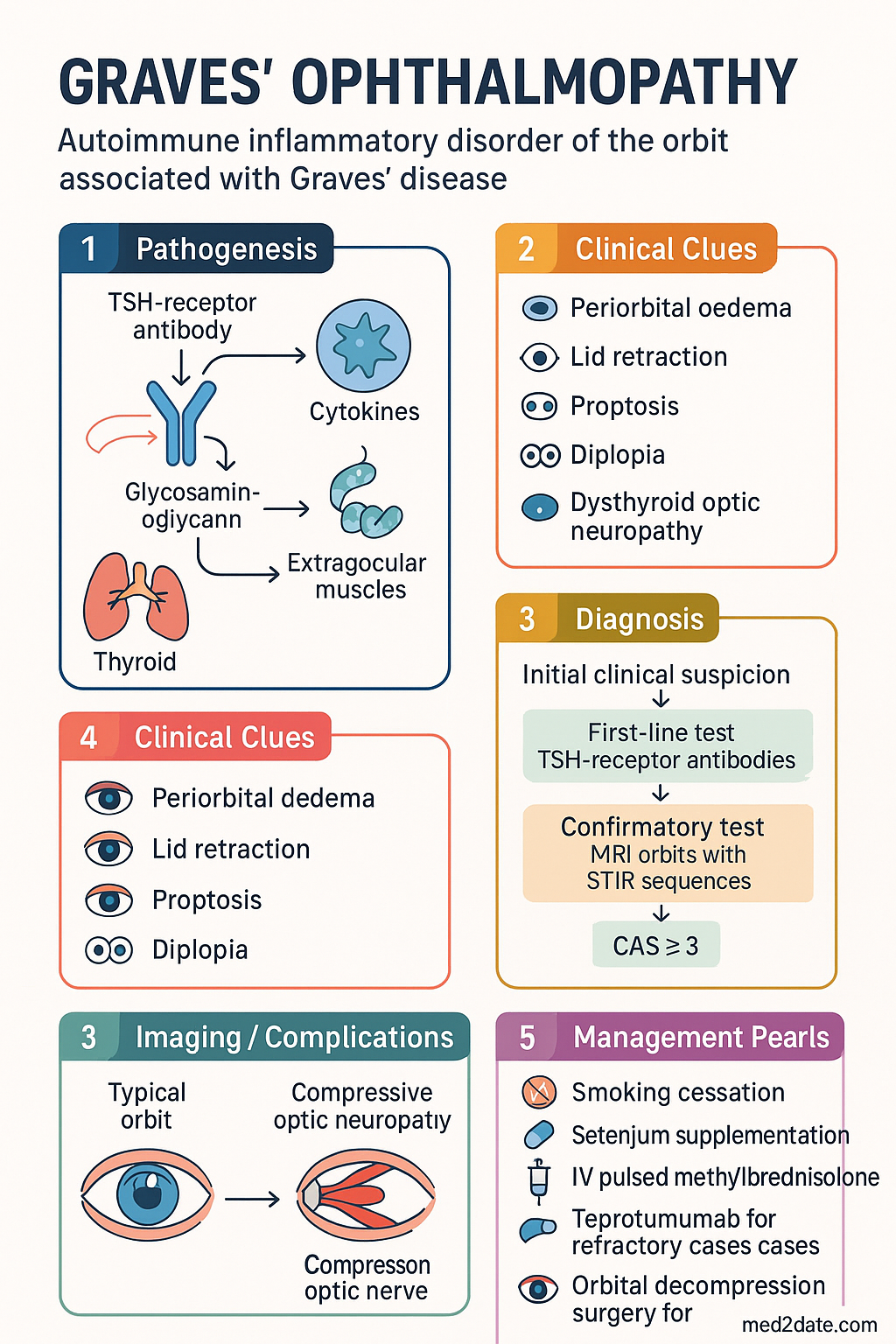
- Graves' ophthalmopathy (GO), also termed thyroid eye disease (TED), is an autoimmune inflammatory disorder of the orbit affecting approximately 25–50% of patients with Graves' disease.
- Cigarette smoking is the single most significant modifiable risk factor, increasing GO risk 5–8-fold and reducing treatment response.
- The Clinical Activity Score (CAS) ≥ 3/7 on initial assessment defines active disease; CAS ≥ 4/10 at follow-up indicates active disease warranting immunosuppression.
- Sight-threatening complications include dysthyroid optic neuropathy (DON), corneal ulceration, and globe subluxation — these constitute endocrine emergencies requiring urgent intervention.
- MRI orbits with STIR sequences is the preferred imaging modality to assess disease activity (muscle oedema) and differentiate active from fibrotic disease.
- TSH-receptor antibody (TRAb) levels correlate with disease activity and severity; monitoring assists in prognostication and treatment response assessment.
- Selenium 100 micrograms twice daily (PBS-listed) for 6 months is recommended for mild active GO based on European multicentre RCT evidence.
- Moderate-to-severe active GO requires IV pulsed methylprednisolone (cumulative dose ≤4.5 g over 12 weeks) as first-line immunosuppression.
- Teprotumumab (anti-IGF-1R monoclonal antibody) is now PBS Authority Required for moderate-to-severe active GO refractory to or intolerant of glucocorticoids.
- Orbital decompression surgery is reserved for sight-threatening DON, disfiguring proptosis in inactive disease, or failed medical therapy — minimum 6 months of stable euthyroidism recommended before rehabilitative surgery.
- Aboriginal and Torres Strait Islander peoples have higher rates of thyroid autoimmunity and may present with more advanced disease; culturally safe, accessible care pathways are essential.
- All patients with Graves' disease should be screened for GO at diagnosis, and antithyroid drug therapy or radioiodine should be managed with concurrent ophthalmology liaison to minimise GO flares.
🎧 Audio Brief
Introduction & Australian Epidemiology
Graves' ophthalmopathy (GO), increasingly referred to as thyroid eye disease (TED), is an autoimmune inflammatory disorder of the extraocular muscles and orbital connective tissue occurring in the context of Graves' disease. The spectrum of clinical manifestations ranges from mild, self-limiting eyelid retraction and soft-tissue inflammation to severe sight-threatening dysthyroid optic neuropathy (DON) and corneal ulceration.
In Australia, Graves' disease accounts for approximately 80% of all thyrotoxicosis, with an estimated prevalence of 0.5–2% of the population. Clinically apparent GO develops in approximately 25–50% of patients with Graves' disease, with moderate-to-severe disease occurring in 3–5% and sight-threatening GO in fewer than 1%. The female-to-male ratio is approximately 5:1, although male patients tend to present with more severe disease at an older age.
The peak incidence occurs in the 40–60-year age group. Australia's strong outdoor culture and historically high smoking rates, particularly in regional and remote communities, have contributed to a disproportionate burden of GO. The condition imposes significant morbidity through diplopia, visual impairment, facial disfigurement, psychosocial distress, and reduced quality of life. Optimal management requires a coordinated multidisciplinary approach involving endocrinology, ophthalmology, radiology, and allied health services.
Pathophysiology & Risk Factors
The pathogenesis of GO involves a complex interplay of humoral and cell-mediated autoimmune mechanisms directed against shared antigens expressed on both thyroid follicular cells and orbital fibroblasts.
Immunopathogenesis
TSH-receptor (TSHR) antibodies are the principal pathogenic drivers. Activated T lymphocytes infiltrate the orbit and stimulate orbital fibroblasts via CD40–CD40L and cytokine interactions (IL-1, IL-6, TNF-α, IFN-γ, IL-17). Orbital fibroblasts, particularly CD34+ fibrocytes expressing TSHR, respond by:
- Glycosaminoglycan (GAG) overproduction: Hyaluronic acid accumulation causes osmotic oedema and expansion of extraocular muscles and orbital fat.
- Adipogenesis: Differentiation of precursor fibroblasts into mature adipocytes increases orbital fat volume.
- Proinflammatory cytokine release: Sustained local inflammation perpetuates tissue remodelling.
Insulin-like growth factor-1 receptor (IGF-1R), expressed on orbital fibroblasts, forms a physical and functional complex with TSHR, amplifying the autoimmune response. This interaction is the target of teprotumumab therapy.
Natural History
GO follows a characteristic biphasic course:
- Active (inflammatory) phase: Duration typically 12–24 months, characterised by dynamic inflammatory signs. This is the window for immunomodulatory therapy.
- Inactive (fibrotic/static) phase: Progressive fibrosis with fixed lid retraction, stable proptosis, and restrictive myopathy. Surgery is generally deferred until this phase.
Risk Factors
| Risk Factor | Effect on GO Risk | Notes |
|---|---|---|
| Cigarette smoking | ↑ 5–8-fold | Most significant modifiable risk factor; dose-dependent; reduces treatment efficacy |
| Radioiodine therapy | ↑ 1.5–4-fold | Risk greatest in smokers with pre-existing GO; prophylactic steroids recommended |
| High TRAb titre | ↑↑ | Strongest biochemical predictor of GO onset, severity, and relapse |
| Female sex | 5:1 ratio | Males more likely to have severe disease when affected |
| Age > 50 years | ↑ | Associated with more severe presentation |
| Uncontrolled hypothyroidism post-treatment | ↑ | Rapid TSH fluctuation is a risk; maintain euthyroidism |
| TSH receptor polymorphisms | ↑ (genetic) | HLA-DRB1, CTLA-4, PTPN22 loci implicated |
Clinical Features & CAS Score
Clinical Manifestations
The clinical presentation of GO encompasses soft-tissue, muscular, and corneal/optic nerve involvement:
- Soft-tissue signs: Periorbital oedema, conjunctival injection, chemosis, caruncular oedema, lid erythema.
- Lid retraction: Upper lid retraction (Dalrymple sign) is the most common early sign, contributing to lid lag, stare, and exposure keratopathy.
- Proptosis: Exophthalmos measured by Hertel exophthalmometry; upper limit of normal approximately 20 mm in Caucasian Australians (adjust for ethnicity).
- Restrictive myopathy: Diplopia and restricted eye movements, particularly in upgaze and abduction (inferior rectus > medial rectus most commonly involved).
- Corneal exposure: Punctate keratopathy, ulceration in severe cases.
- Dysthyroid optic neuropathy (DON): Reduced visual acuity, impaired colour vision (red desaturation), visual field defects, relative afferent pupillary defect, disc oedema or pallor.
Werner Classification (NOSPECS — historical but still used)
| Class | Description |
|---|---|
| 0 | No signs or symptoms |
| 1 | Only signs (lid retraction, stare) — no symptoms |
| 2 | Soft-tissue involvement (oedema, chemosis) |
| 3 | Proptosis (≥ upper limit of normal for ethnicity) |
| 4 | Extraocular muscle involvement (diplopia) |
| 5 | Corneal involvement (ulceration) |
| 6 | Sight loss (DON, optic atrophy) |
Clinical Activity Score (CAS)
The CAS, developed by the European Group on Graves' Orbitopathy (EUGOGO), is the standard tool for assessing disease activity and guiding treatment decisions:
| CAS Parameter (one point each) | Assessment |
|---|---|
| Spontaneous retrobulbar pain | Patient-reported |
| Pain on attempted up- or downgaze | Clinical examination |
| Redness of the eyelids | Clinical examination |
| Redness of the conjunctiva (diffuse injection) | Clinical examination |
| Swelling of the eyelids | Clinical examination |
| Inflammation of the caruncle and/or plica | Clinical examination |
| Conjunctival oedema (chemosis) | Clinical examination |
Investigations
Investigation of GO serves three purposes: confirming the diagnosis, assessing disease activity and severity, and monitoring treatment response.
Thyroid Function & Autoantibodies
Orbital Imaging
Ophthalmological Assessment
Orbital Doppler Ultrasound
B-scan and A-scan orbital ultrasound can assess extraocular muscle thickness and reflectivity. Available at specialist ophthalmology practices. Less operator-dependent than CT/MRI for measuring muscle enlargement, though limited in assessing the orbital apex (critical for DON evaluation).
Management & Orbital Decompression
Management of GO is stratified by disease severity and activity. All patients require optimisation of thyroid function, smoking cessation, and multidisciplinary coordination.
Supportive & General Measures (All Severities)
- Smoking cessation: Structured programme with pharmacotherapy (nicotine replacement, varenicline [Champix® — PBS], or bupropion [Zyban® — PBS]).
- Thyroid function control: Aim for stable euthyroidism. Avoid rapid correction of hypothyroidism. Liaise with endocrinology for optimal antithyroid drug dosing.
- Lubricants: Preservative-free artificial tears (e.g., Systane® Ultra — PBS) four to six times daily and ophthalmic ointment (polyvinyl alcohol [Liquifilm® — PBS]) at bedtime for exposure keratopathy.
- Sunglasses and prisms: Wraparound sunglasses for photophobia; temporary press-on Fresnel prisms for diplopia.
- Head-of-bed elevation: 15–30° to reduce periorbital oedema.
- Selenium supplementation: See mild disease management below.
Mild Active GO — CAS < 3
Evidence from the EUGOGO multicentre RCT (Lancet Diabetes Endocrinol 2016) demonstrated that selenium 100 µg twice daily for 6 months significantly improved quality of life, reduced CAS, and prevented GO progression compared with placebo. Benefit was observed even in selenium-replete populations such as Australia. Pentoxifylline 400 mg PO TDS may be considered as an alternative (limited evidence).
Moderate-to-Severe Active GO — CAS ≥ 3
First-Line: IV Pulsed Glucocorticoids
Second-Line / Adjunctive: Teprotumumab
Teprotumumab is indicated for moderate-to-severe active GO that is refractory to or intolerant of systemic glucocorticoids, or where glucocorticoids are contraindicated. The landmark OPTIC trials (NEJM 2020, Lancet 2021) demonstrated significant proptosis reduction (≥2 mm) in 71% of patients compared with 20% placebo, and improvement in CAS, diplopia, and quality of life. PBS Authority approval requires prior specialist assessment and documentation of inadequate response to first-line therapy.
Other Immunosuppressive Options
- Oral prednisone: 0.5–1 mg/kg/day, taper over 3–6 months. Less effective than IV pulsed therapy and greater systemic side effects. PBS General Benefit.
- Rituximab: 1000 mg IV × 2 doses (2 weeks apart). Emerging evidence for GO refractory to glucocorticoids. Off-label use; requires specialist initiation. PBS Authority Required for other indications.
- Mycophenolate mofetil: 500–1000 mg PO twice daily. Used as steroid-sparing agent. Limited GO-specific RCT data. PBS Authority Required.
- Orbital radiotherapy: 20 Gy in 10 fractions over 2 weeks. Effective as adjunct to glucocorticoids. Avoid in diabetic retinopathy. Available at major radiotherapy centres (Peter MacCallum, Royal Adelaide, Westmead).
Sight-Threatening GO (DON / Corneal Ulceration)
Orbital Decompression — Indications & Techniques
Orbital decompression surgery is performed for two principal indications:
- Sight-threatening DON: Emergency decompression when medical therapy fails or is insufficient (apical decompression prioritised).
- Rehabilitative (cosmetic/functional): Correction of disfiguring proptosis in patients with inactive GO (CAS 0/7 for ≥6 months).
| Technique | Walls Decompressed | Proptosis Reduction | Key Considerations |
|---|---|---|---|
| Endoscopic medial wall + medial floor | Medial, inferomedial | 3–5 mm | Lower diplopia rate; preferred for DON; ENT co-surgery |
| Lateral wall (Docker technique) | Lateral | 2–4 mm | Lower diplopia risk; used in combination for balanced decompression |
| Three-wall (medial, floor, lateral) | Medial, floor, lateral | 6–10 mm | Maximum proptosis reduction; higher new-onset diplopia rate (~30%) |
| Fat decompression | Orbital fat removal | 2–4 mm | Often combined with bony decompression; suitable for high fat fraction GO |
Rehabilitative surgery follows a sequential approach once the patient has been euthyroid and GO has been inactive for ≥6 months: (1) orbital decompression → (2) strabismus surgery (if diplopia persists) → (3) eyelid surgery (levator recession, blepharoplasty). Interval between stages is typically 3–6 months.
Graves' Thyrotoxicosis Treatment — Impact on GO
Radioiodine: Can worsen or precipitate GO in 15–20% of patients. Risk is highest in smokers and those with pre-existing GO. Prophylactic prednisone 0.3–0.5 mg/kg/day for 3 months (starting 1 day after radioiodine, taper over 3 months) is recommended for patients with active GO or significant risk factors. Coordinate with endocrinology and ophthalmology before radioiodine administration.
Antithyroid drugs (carbimazole, propylthiouracil): Do not exacerbate GO. Preferred initial therapy when GO is active or at high risk.
Total thyroidectomy: May be considered to eliminate the thyroid antigenic source, particularly in severe GO with high TRAb. Some evidence suggests improved GO outcomes post-total thyroidectomy combined with radioiodine ablation.
Special Populations
Graves' disease may improve or flare in the post-partum period. Monitor closely for GO exacerbation in the first 6 months after delivery. Breastfeeding is not a contraindication to selenium or glucocorticoid therapy.
Juvenile Graves' ophthalmopathy is uncommon (5–10% of paediatric Graves' disease) and usually mild. Severe disease should prompt evaluation for alternative diagnoses. Management at a tertiary paediatric centre with experienced multidisciplinary team is recommended.
Aboriginal and Torres Strait Islander Health Considerations
📚 References
- 1. Bartalena L, Kahaly GJ, Baldeschi L, et al. The 2021 European Group on Graves' Orbitopathy (EUGOGO) clinical practice guidelines for the medical management of Graves' orbitopathy. Eur J Endocrinol. 2021;185(4):G43–G67.
- 2. Smith TJ, Kahaly GJ, Ezra DG, et al. Teprotumumab for thyroid-associated ophthalmopathy. N Engl J Med. 2020;382(19):1789–1799.
- 3. Douglas RS, Kahaly GJ, Patel A, et al. Teprotumumab for the treatment of active thyroid eye disease. N Engl J Med. 2020;382(4):341–352.
- 4. Marcocci C, Kahaly GJ, Krassas GE, et al. Selenium and the course of mild Graves' orbitopathy. N Engl J Med. 2011;364(20):1920–1931.
- 5. Kahaly GJ, Riedl M, König J, et al. Mycophenolate plus methylprednisolone versus methylprednisolone alone in active, moderate-to-severe Graves' orbitopathy (MINGO): a randomised, observer-masked, multicentre trial. Lancet Diabetes Endocrinol. 2018;6(4):287–298.
- 6. Mourits MP, Koornneef L, Wiersinga WM, et al. Clinical criteria for the assessment of disease activity in Graves' ophthalmopathy: a novel approach. Br J Ophthalmol. 1989;73(8):639–644.
- 7. Australian Institute of Health and Welfare (AIHW). Thyroid disease in Australia. Cat. no. AUS 235. Canberra: AIHW; 2023.
- 8. Bartalena L, Marcocci C, Bogazzi F, et al. Relation between therapy for hyperthyroidism and the course of Graves' ophthalmopathy. N Engl J Med. 1998;338(2):73–78.
- 9. Royal Australian College of General Practitioners (RACGP). Smoking cessation — a guide for health professionals. 3rd ed. East Melbourne: RACGP; 2021.
- 10. Aboriginal and Torres Strait Islander Health Practice Board of Australia. Guidelines for culturally safe health care. 2020.
- 11. Bahn RS. Graves' ophthalmopathy. N Engl J Med. 2010;362(8):726–738.
- 12. Dolman PJ. Dysthyroid optic neuropathy: evaluation and management. J Endocrinol Invest. 2021;44(3):421–429.
- 13. Pharmaceuticals Benefits Scheme (PBS). Teprotumumab (Tepezza®) — Authority Required listing. Australian Government Department of Health and Aged Care; 2024.