📋 Key Information Summary
- Thyroid nodules are detected in up to 68% of adults on high-resolution ultrasound; the overwhelming majority (>95%) are benign.
- Thyroid cancer incidence in Australia is rising (≈16 per 100,000 in 2024); papillary carcinoma accounts for ≈85% of cases.
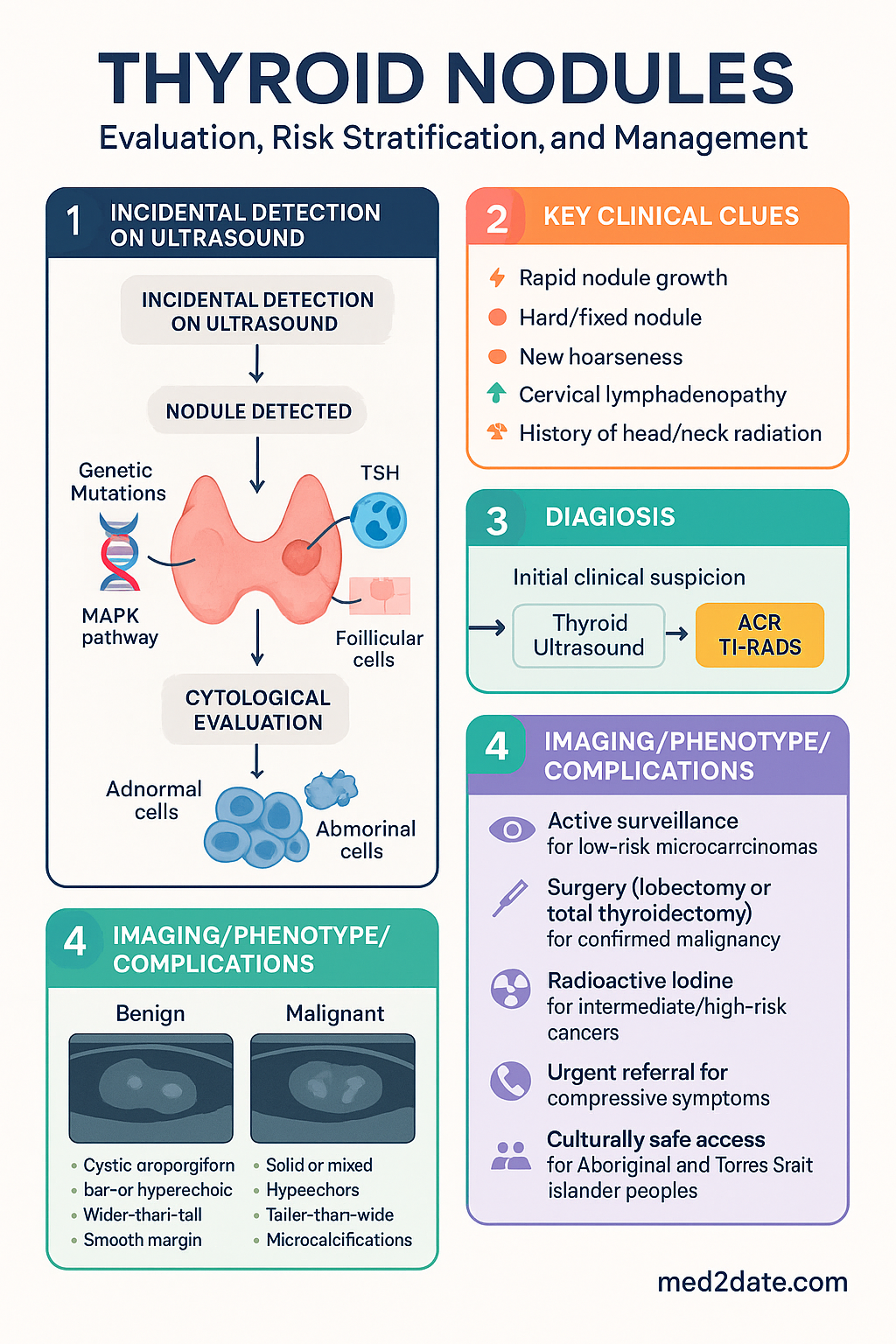
- Ultrasound risk stratification using the ACR TI-RADS system guides the decision to biopsy or surveil.
- Fine needle aspiration (FNA) cytology is the gold standard for evaluating suspicious nodules; results are reported using the Bethesda System (six categories).
- Bethesda III–VI nodules carry a 10–95% risk of malignancy; molecular testing (where available) can help avoid diagnostic surgery.
- Most thyroid cancers are indolent; active surveillance is appropriate for selected low-risk papillary microcarcinomas ≤10 mm.
- Surgery (lobectomy or total thyroidectomy) remains the primary treatment for confirmed or high-suspicion malignancy.
- Radioactive iodine (I-131) ablation is reserved for intermediate- to high-risk differentiated thyroid cancers post-surgery.
- Thyroid function tests (TSH, free T4) should be performed in every patient with a thyroid nodule.
- Compressive symptoms (dysphagia, dyspnoea, voice change) or rapid growth mandate urgent surgical referral.
- Aboriginal and Torres Strait Islander peoples have lower thyroid cancer incidence but present at more advanced stages; culturally safe access to ultrasound and FNA is critical.
- MBS items exist for thyroid ultrasound (Item 55047) and ultrasound-guided FNA (Item 30074); PET-CT for thyroid cancer staging is available on Medicare (Item 61506) under specific criteria.
🎧 Audio Brief
Introduction & Australian Epidemiology
Thyroid nodules are discrete lesions within the thyroid parenchyma that are radiologically and clinically distinct from the surrounding tissue. With the widespread use of high-resolution neck ultrasound and cross-sectional imaging (CT, MRI, PET), incidental thyroid nodules have become an increasingly common clinical finding. Autopsy and ultrasound studies suggest that up to 50–68% of adults harbour at least one thyroid nodule, though the vast majority remain clinically silent.
The primary concern when a thyroid nodule is identified is the exclusion of malignancy. Approximately 5–7% of palpable nodules harbour thyroid cancer, while the cancer rate among incidentally discovered nodules is lower (≈1–2%). Thyroid cancer is now the twelfth most common cancer diagnosed in Australia, with age-standardised incidence rates of approximately 16 per 100,000 persons per year (AIHW Cancer Data, 2024). Over the past two decades, incidence has roughly doubled, driven largely by increased detection of small papillary carcinomas.
Despite this rising incidence, mortality from thyroid cancer remains low (≈0.5 per 100,000), reflecting the indolent nature of most differentiated thyroid cancers. Papillary thyroid carcinoma (PTC) accounts for approximately 85% of all thyroid malignancies, followed by follicular carcinoma (≈10%), medullary carcinoma (≈3–5%), and anaplastic carcinoma (<2%).
This guideline provides an evidence-based, Australian-context approach to the evaluation, risk stratification, and management of thyroid nodules in adult patients presenting to primary care, endocrinology, and surgical services.
Epidemiology & Risk Factors for Malignancy
Prevalence
Thyroid nodule prevalence varies with detection method, age, sex, and iodine status:
- Palpation studies: 4–7% of women, 1–2% of men
- Ultrasound studies: 20–68% of adults (higher in older women)
- Autopsy series: 36–65% harbour occult nodules
- Female predominance: 4:1 female-to-male ratio for benign nodules; 3:1 for thyroid cancer
- Age: Prevalence increases with age; peak cancer incidence at 40–60 years
Australia has maintained iodine sufficiency since the mandatory iodisation of bread salt in 2009 (FSANZ Standard 2.1.1), reducing the prevalence of iodine-deficiency-related goitre. However, mild iodine insufficiency persists in some regions, notably Tasmania and parts of Victoria.
Risk Factors for Malignancy
| Risk Factor | Category | Association |
|---|---|---|
| Age <20 or >60 years | Patient factor | Higher malignancy risk at extremes of age |
| Male sex | Patient factor | Higher malignancy risk per nodule (fewer benign nodules) |
| History of head/neck radiation | Radiation exposure | Strong association, especially childhood radiation therapy |
| Family history of thyroid cancer | Genetic | Papillary and medullary (MEN2A/2B, familial MTC) |
| MEN2A / MEN2B / FAP / Cowden syndrome | Genetic | Medullary (RET proto-oncogene), follicular (PTEN) |
| Rapid nodule growth | Clinical feature | Suspicious; but also seen in benign haemorrhagic cysts |
| Firm/hard, fixed nodule | Clinical feature | Higher malignancy probability |
| New cervical lymphadenopathy | Clinical feature | Highly suspicious for papillary or medullary carcinoma |
| Vocal cord paralysis / hoarseness | Clinical feature | Suggests local invasion; high specificity for malignancy |
| History of familial adenomatous polyposis (FAP) | Genetic | Papillary thyroid cancer (cribriform-morular variant) |
Clinical Assessment & Ultrasound Classification
Clinical History
A targeted history should address:
- Duration and rate of nodule growth (self-noticed or incidentally found)
- Compressive symptoms: dysphagia, dyspnoea, odynophagia, choking sensation
- Voice changes or hoarseness (recurrent laryngeal nerve involvement)
- Symptoms of thyroid dysfunction: weight change, tremor, heat/cold intolerance, palpitations, constipation
- Risk factors: family history of thyroid cancer or MEN syndromes, prior head/neck irradiation, recent rapid growth
- Jod-Basedow phenomenon: prior iodinated contrast exposure (CT angiography) may unmask autonomous nodules
Physical Examination
Examine the thyroid with the patient seated, neck slightly extended. Assess:
- Nodule size, consistency (soft, firm, hard), mobility, and tenderness
- Fixation to adjacent structures (trachea, strap muscles)
- Ipsilateral or bilateral cervical lymph node stations (II, III, IV, VI)
- Signs of thyrotoxicosis (tachycardia, tremor, lid lag) or hypothyroidism
- Pemberton's sign: facial plethora on arm elevation suggesting substernal goitre
Baseline Investigations
- TSH (MBS Item 66719) — perform in all patients with a thyroid nodule; if suppressed, order free T4 and free T3
- Free T4 / Free T3 — if TSH suppressed (possible autonomous or toxic nodule)
- Calcitonin — consider if medullary thyroid carcinoma (MTC) is suspected (elevated calcitonin is sensitive for MTC); available at major reference laboratories (Sullivan Nicolaides, Douglass Hanly Moir)
- Thyroglobulin — generally not useful in the diagnostic workup of a new nodule; used post-thyroidectomy for surveillance
- FBC, UEC, LFTs — baseline pre-operative workup if surgery is planned
Thyroid Ultrasound
High-resolution grey-scale ultrasound is the single most important imaging modality for thyroid nodule evaluation. It should be performed by an experienced sonographer or radiologist with thyroid ultrasound expertise.
ACR TI-RADS Classification
The American College of Radiology (ACR) Thyroid Imaging Reporting and Data System (TI-RADS) is the recommended classification system. Five ultrasound features are scored:
| Feature | Points |
|---|---|
| Composition | Cystic/almost completely cystic = 0; Spongiform = 0; Mixed = 1; Solid = 2 |
| Echogenicity | Anechoic = 0; Hyperechoic = 1; Isoechoic = 2; Hypoechoic = 3; Very hypoechoic = 3 |
| Shape | Wider-than-tall = 0; Taller-than-wide = 3 |
| Margin | Smooth/ill-defined = 0; Lobulated/irregular = 2; Extrathyroidal extension = 3 |
| Echogenic foci | None/large comet-tail = 0; Macrocalcification = 1; Peripheral calcification = 2; Punctate echogenic foci = 3 |
TI-RADS Categories & Management
Fine Needle Aspiration (FNA) & Bethesda System
Fine Needle Aspiration Biopsy
Ultrasound-guided FNA is the gold standard for cytological evaluation of thyroid nodules. It has a sensitivity of 90–97% and specificity of 50–75% for thyroid malignancy.
Procedural Details
- Performed under real-time ultrasound guidance using a 25–27 gauge needle
- Minimum 6 passes recommended for adequacy (or 2–4 passes with rapid on-site evaluation [ROSE], where available)
- Aspirate smears are air-dried or alcohol-fixed; needle washings in liquid-based medium for cell block
- Cystic nodules: aspirate fluid first; re-biopsy any residual solid component
- Local anaesthesia (1% lidocaine) is optional but improves patient comfort
- Post-procedure: apply gentle pressure for 5 minutes; patient can resume normal activities
MBS & Access
- MBS Item 30074: Ultrasound-guided fine needle aspiration of thyroid — covers the procedure when performed by a specialist or credentialed practitioner
- Available at most public hospital radiology departments and private radiology practices across metropolitan and major regional centres
- Wait times: typically 2–4 weeks in the public system; 1–2 weeks in private
- Remote/rural access: mobile ultrasound services and telehealth review of imaging can facilitate triage; patients in remote areas may require travel to regional centres for FNA
Bethesda System for Reporting Thyroid Cytopathology
The Bethesda System (2017 revision) standardises thyroid FNA cytology reporting into six diagnostic categories, each with an associated risk of malignancy (ROM) and recommended management.
| Bethesda Category | Diagnosis | ROM (Nodule ≥1 cm) | Recommended Action |
|---|---|---|---|
| I | Non-diagnostic / Unsatisfactory | 5–10% | Repeat FNA with ultrasound guidance (≥12 weeks); if persistently non-diagnostic, consider diagnostic lobectomy or surveillance |
| II | Benign | 0–3% | Clinical and ultrasound surveillance; repeat US at 12–24 months then at intervals per TI-RADS category |
| III | Atypia of Undetermined Significance (AUS) / Follicular Lesion of Undetermined Significance (FLUS) | 10–30% | Repeat FNA (preferred), molecular testing (where available), or diagnostic lobectomy |
| IV | Follicular Neoplasm / Suspicious for Follicular Neoplasm | 25–40% | Molecular testing (Afirma, ThyroSeq) or diagnostic lobectomy. MTC excluded if calcitonin normal. |
| V | Suspicious for Malignancy | 50–75% | Near-total thyroidectomy or lobectomy (depending on nodule size, extent, and patient factors); multidisciplinary team (MDT) discussion |
| VI | Malignant | 97–99% | Total thyroidectomy or lobectomy ± central compartment dissection; MDT discussion; referral to endocrine surgeon and endocrinologist |
Molecular Testing
Molecular testing of FNA samples can refine malignancy risk assessment for Bethesda III and IV nodules, potentially avoiding diagnostic surgery. Available platforms include:
- Afirma Genomic Sequencing Classifier (GSC): Classifies nodules as "benign" or "suspicious." A benign result can support observation for Bethesda III/IV nodules.
- ThyGenX / ThyroSeq v3: Next-generation sequencing panel testing for point mutations (BRAF, RAS, TERT promoter) and gene fusions (RET/PTC, PAX8/PPARγ).
- BRAF V600E testing: Available at major Australian pathology laboratories (e.g., Sonic Healthcare, Laverty). High specificity for papillary thyroid carcinoma. If positive, the nodule is almost certainly malignant.
Management Algorithm
Stepwise Approach to Thyroid Nodule Management
Surgical Management
| Procedure | Indications | Considerations |
|---|---|---|
| Diagnostic lobectomy | Bethesda III or IV (if molecular testing unavailable or equivocal) | Allows histological assessment of capsule invasion (follicular carcinoma diagnosis requires invasion); completion thyroidectomy if malignancy confirmed |
| Total thyroidectomy | Confirmed thyroid cancer >4 cm; bilateral nodularity; extrathyroidal extension; known distant metastases; prior head/neck radiation + cancer | Lifelong levothyroxine replacement required; risk of bilateral recurrent laryngeal nerve injury and hypoparathyroidism |
| Lobectomy | Unilateral papillary microcarcinoma ≤1 cm (low-risk); benign dominant nodule causing symptoms; follicular neoplasm on cytology | May avoid lifelong thyroxine; contralateral lobe may maintain euthyroid state |
| Central compartment dissection | Clinical or US-detected level VI lymph node metastases in PTC/MTC | Prophylactic central dissection for MTC (all cases) and PTC with cN1 disease |
Post-Surgical Management
Levothyroxine Replacement & TSH Suppression
Radioactive Iodine (I-131) Therapy
Active Surveillance for Low-Risk Papillary Microcarcinoma
Active surveillance (AS) is an accepted alternative to immediate surgery for papillary microcarcinomas (≤1 cm) without evidence of extrathyroidal extension, lymph node metastases, or aggressive histology. This approach is supported by data from Kuma Hospital (Korea) and Memorial Sloan Kettering Cancer Center (USA).
- Ultrasound surveillance every 6 months for 2 years, then annually
- Conversion to surgery if: nodule grows ≥3 mm, new lymph node metastases detected, patient preference changes
- Rate of disease progression requiring conversion: approximately 5–10% over 10 years
- Requires experienced thyroid ultrasound operator and patient adherence
- Appropriate patient selection is critical; not suitable for high-risk features (TERT mutation, BRAF + TERT co-mutation, aggressive subtypes)
Thyroid Surveillance (Bethesda II Benign Nodules)
- Repeat ultrasound at 12–24 months
- If stable, further surveillance at 3–5 year intervals
- Repeat FNA if: ≥50% increase in volume, new suspicious US features, new lymphadenopathy
- Consider stopping surveillance after 2 stable examinations in low-risk patients
Special Populations
Aboriginal and Torres Strait Islander Health Considerations
Thyroid cancer incidence among Aboriginal and Torres Strait Islander peoples is lower than in the non-Indigenous population, though data are limited by under-identification in cancer registries. When thyroid cancer is diagnosed in Indigenous Australians, it tends to present at a more advanced stage, with poorer outcomes.
📚 References
- 1. Haugen BR, Alexander EK, Bible KC, et al. 2015 American Thyroid Association Management Guidelines for Adult Patients with Thyroid Nodules and Differentiated Thyroid Cancer. Thyroid. 2016;26(1):1-133.
- 2. Tessler FN, Middleton WD, Grant EG, et al. ACR Thyroid Imaging, Reporting and Data System (TI-RADS): White Paper of the ACR TI-RADS Committee. J Am Coll Radiol. 2017;14(5):587-595.
- 3. Cibas ES, Ali SZ. The 2017 Bethesda System for Reporting Thyroid Cytopathology. Thyroid. 2017;27(11):1341-1346.
- 4. Australian Institute of Health and Welfare (AIHW). Cancer Data in Australia. Canberra: AIHW; 2024. Available from: https://www.aihw.gov.au/reports/cancer/cancer-data-in-australia
- 5. Cancer Council Australia. Thyroid Cancer Guidelines Wiki. Sydney: Cancer Council Australia; 2023.
- 6. Patel KN, Yip L, Lubitz CC, et al. The American Association of Endocrine Surgeons Guidelines for the Definitive Surgical Management of Thyroid Disease in Adults. Ann Surg. 2020;271(3):e21-e93.
- 7. Ito Y, Miyauchi A, Kihara M, et al. Patient age is significantly related to the progression of papillary microcarcinoma during active surveillance. Thyroid. 2014;24(1):27-34.
- 8. Tuttle RM, Haugen B, Perrier ND. Updated American Joint Committee on Cancer/Tumor-Node-Metastasis Staging System for Differentiated and Anaplastic Thyroid Cancer (Eighth Edition). Thyroid. 2017;27(10):1260-1270.
- 9. Ross DS, Burch HB, Cooper DS, et al. 2016 American Thyroid Association Guidelines for Diagnosis and Management of Hyperthyroidism and Other Causes of Thyrotoxicosis. Thyroid. 2016;26(10):1343-1421.
- 10. Royal Australasian College of Surgeons (RACS). Position Statement: Thyroid and Parathyroid Surgery. Melbourne: RACS; 2022.
- 11. Australian Government Department of Health. Medicare Benefits Schedule (MBS) — Items 55047, 30074, 61506. Available from: http://www.mbsonline.gov.au
- 12. Conron M, Finlayson M, Cullen R. Primary thyroid lymphoma: a review of clinical presentation, diagnosis, and management. ANZ J Surg. 2020;90(4):498-503.
- 13. ARPANSA. Recommendations for Radiation Protection in Nuclear Medicine — Iodine-131 Therapy. Sydney: Australian Radiation Protection and Nuclear Safety Agency; 2021.
- 14. National Health and Medical Research Council (NHMRC). National Statement on Ethical Conduct in Human Research. Canberra: NHMRC; 2023 (updated).
- 15. Australian Government, Food Standards Australia New Zealand (FSANZ). Mandatory Iodine Fortification of Bread: Standard 2.1.1. Canberra: FSANZ; 2009.