📋 Key Information Summary
- Hypocalcaemia is defined as a serum albumin-corrected calcium <2.10 mmol/L or ionised calcium <1.10 mmol/L. It requires urgent assessment for acute symptoms and underlying cause.
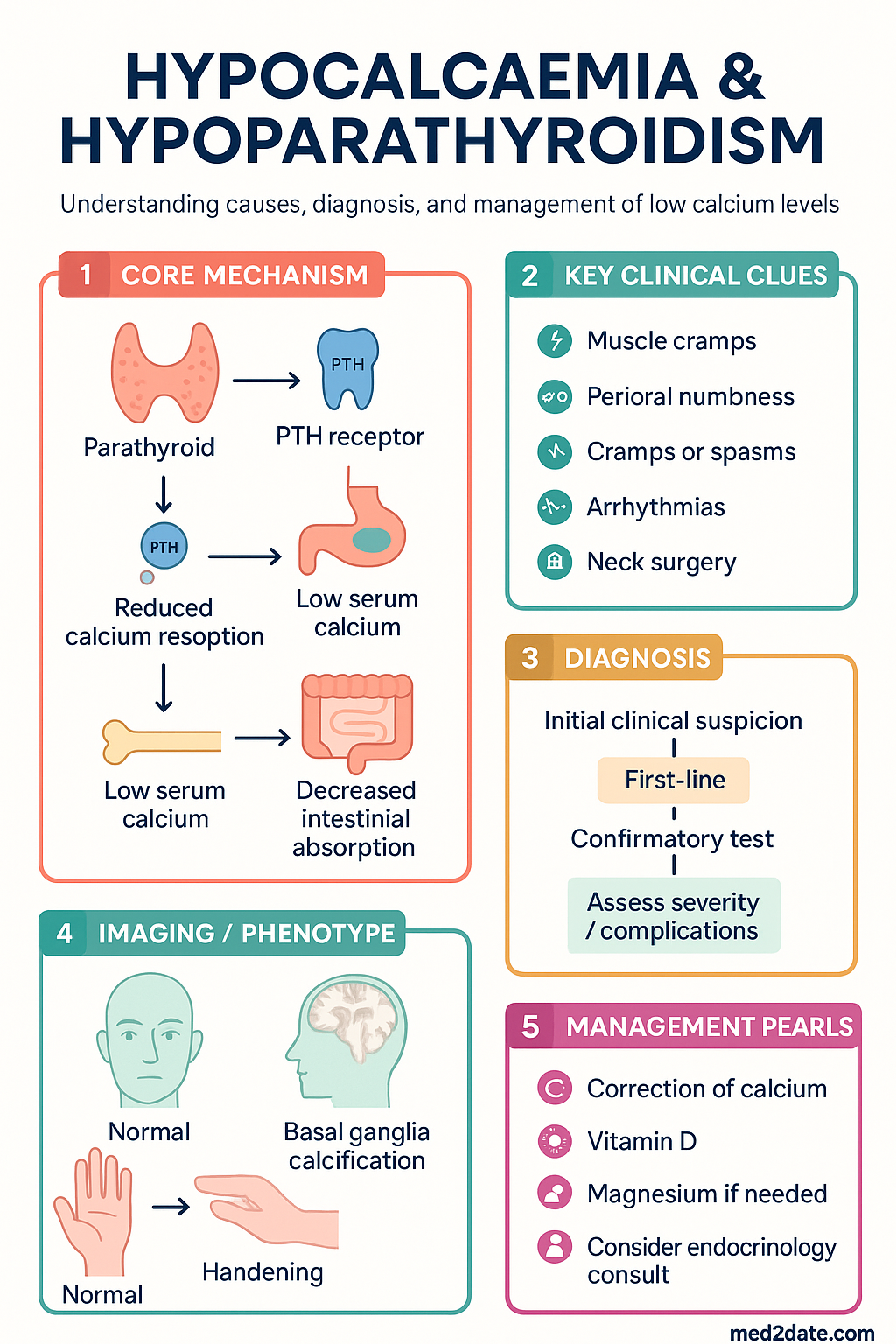
- Hypoparathyroidism is the most common cause of chronic hypocalcaemia, usually iatrogenic following anterior neck surgery. Autoimmune and genetic causes are less common.
- Acute symptomatic hypocalcaemia is a medical emergency. Intravenous calcium gluconate is first-line to rapidly correct levels and prevent laryngospasm or seizures.
- Classic signs include perioral/acral paraesthesia, muscle cramps, tetany, and characteristic findings like Trousseau's sign (carpopedal spasm) and Chvostek's sign (facial muscle twitching).
- Investigations must include corrected calcium, phosphate, magnesium, PTH, 25-hydroxyvitamin D, and renal function to determine the aetiology.
- First-line oral therapy for chronic hypoparathyroidism involves calcium carbonate/citrate supplements combined with calcitriol (active vitamin D).
- Recombinant human parathyroid hormone (1-84) (Natpara®) is available via the PBS as an adjunct for patients with refractory hypocalcaemia despite standard therapy.
- Magnesium deficiency must be corrected concurrently, as it causes PTH resistance and impairs secretion.
- Monitoring is essential to avoid overtreatment (hypercalcaemia, hypercalciuria) and long-term complications like nephrocalcinosis and renal impairment.
- Aboriginal and Torres Strait Islander peoples may have higher rates of postsurgical hypoparathyroidism and require tailored, accessible chronic disease management.
🎧 Audio Brief
Introduction & Australian Epidemiology
Hypocalcaemia is a common electrolyte disturbance characterised by a low concentration of calcium in the blood. Calcium is critical for neuromuscular excitability, cardiac function, coagulation, and bone health. A reduction in serum calcium leads to increased neuronal membrane permeability to sodium ions, resulting in neuromuscular irritability.
Hypoparathyroidism, the most common cause of chronic hypocalcaemia, results from deficient or absent parathyroid hormone (PTH). PTH is the principal regulator of calcium homeostasis, acting on bone (resorption), kidneys (reabsorption and activation of vitamin D), and intestine (indirectly via vitamin D). In Australia, post-surgical hypoparathyroidism accounts for approximately 75% of cases, occurring in 1–7% of patients following total thyroidectomy, parathyroidectomy, or radical neck dissection for malignancy.
Other significant causes include autoimmune hypoparathyroidism (isolated or part of autoimmune polyendocrine syndrome type 1), functional hypoparathyroidism due to severe hypomagnesaemia, and vitamin D deficiency, which remains prevalent in the Australian population. Acute hypocalcaemia can be life-threatening, necessitating rapid diagnosis and management.
Pathophysiology & Causes
Calcium homeostasis is maintained by a balance between intestinal absorption, renal reabsorption, and skeletal turnover, tightly regulated by PTH and vitamin D. Hypocalcaemia results from either increased calcium loss or inadequate calcium supply/uptake, most often due to impaired PTH action or vitamin D deficiency.
Major Causes by Mechanism
| Mechanism | Common Causes | Key Pathophysiological Defect |
|---|---|---|
| PTH Deficiency/Resistance |
|
Reduced PTH secretion or action → decreased bone resorption, renal calcium reabsorption, and 1,25-dihydroxyvitamin D production. |
| Vitamin D Deficiency |
|
Reduced intestinal calcium absorption. PTH may be elevated (secondary hyperparathyroidism) but cannot fully compensate. |
| Increased Calcium Loss |
|
Calcium sequestration by fatty acids (pancreatitis) or increased renal excretion. |
Clinical Features (Trousseau's, Chvostek's, Tetany)
Clinical manifestations correlate with the degree and rapidity of fall in serum calcium. Chronic, mild hypocalcaemia may be asymptomatic, while acute or severe hypocalcaemia can present with life-threatening neuromuscular and cardiac complications.
Symptoms and Signs
- Neuromuscular: Perioral numbness, tingling in fingers and toes, muscle cramps, carpopedal spasm, laryngospasm, bronchospasm, and seizures.
- Central Nervous System: Anxiety, irritability, depression, confusion, and raised intracranial pressure (papilloedema).
- Cardiac: Prolongation of the QTc interval on ECG, predisposing to torsades de pointes and heart failure.
- Chronic: Dry skin, brittle nails, coarse hair, cataracts, dental enamel hypoplasia, and basal ganglia calcification.
Classic Bedside Signs
Investigations
Investigation should confirm hypocalcaemia, determine its severity and chronicity, and identify the underlying cause. A systematic approach is essential.
First-Line Investigations
Second-Line / Aetiological Investigations
Management (Calcium, Vitamin D, PTH Analogue)
Management goals are to: 1) Acutely correct symptomatic hypocalcaemia; 2) Maintain serum calcium in the low-normal range (target 2.00–2.12 mmol/L) to avoid symptoms and complications; and 3) Minimise urinary calcium excretion to protect renal function.
Acute Symptomatic Hypocalcaemia
Chronic Management (Hypoparathyroidism)
First-line therapy combines oral calcium supplements with active vitamin D analogue.
Adjunctive / Refractory Therapy
Monitoring Plan
Special Populations
📚 References
- 1. Shoback D. Hypocalcemia: Definition, Etiology, Pathogenesis, Diagnosis, and Management. In: Rosen CJ, ed. Primer on the Metabolic Bone Diseases and Disorders of Mineral Metabolism. 9th ed. Wiley; 2019:575-586.
- 2. Australian Institute of Health and Welfare (AIHW). Chronic kidney disease prevalence among Aboriginal and Torres Strait Islander people. AIHW; 2023.
- 3. Brandi ML, Bilezikian JP, Shoback D, et al. Management of Hypoparathyroidism: Summary Statement and Guidelines. J Clin Endocrinol Metab. 2016;101(6):2273-2283.
- 4. The Royal Australian College of General Practitioners (RACGP). Management of hypothyroidism in primary care. RACGP; 2023.
- 5. Mannstadt M, Clarke BL, Vokes T, et al. Efficacy and safety of recombinant human parathyroid hormone (1-84) in hypoparathyroidism (REPLACE): a double-blind, placebo-controlled, randomised, phase 3 study. Lancet Diabetes Endocrinol. 2013;1(4):275-283.
- 6. Department of Health (Australia). Pharmaceutical Benefits Schedule (PBS). Parathyroid hormone (1-84). Published 2024. Accessed [Current Date].
- 7. Society for Endocrinology (UK). Endocrine emergencies: hypocalcaemia. Clinical Guidance. 2021.
- 8. Nowak A, Loeffler J, Schacht C, et al. Calcification of cerebral arteries and basal ganglia in patients with postsurgical hypoparathyroidism. J Clin Endocrinol Metab. 2021;106(12):e5013-e5022.
- 9. Australian Commission on Safety and Quality in Health Care (ACSQHC). National Safety and Quality Health Service Standards. 2nd ed. ACSQHC; 2021.
- 10. Aboriginal and Torres Strait Islander Health Practice Board of Australia. Cultural safety framework. 2022.