📋 Key Information Summary
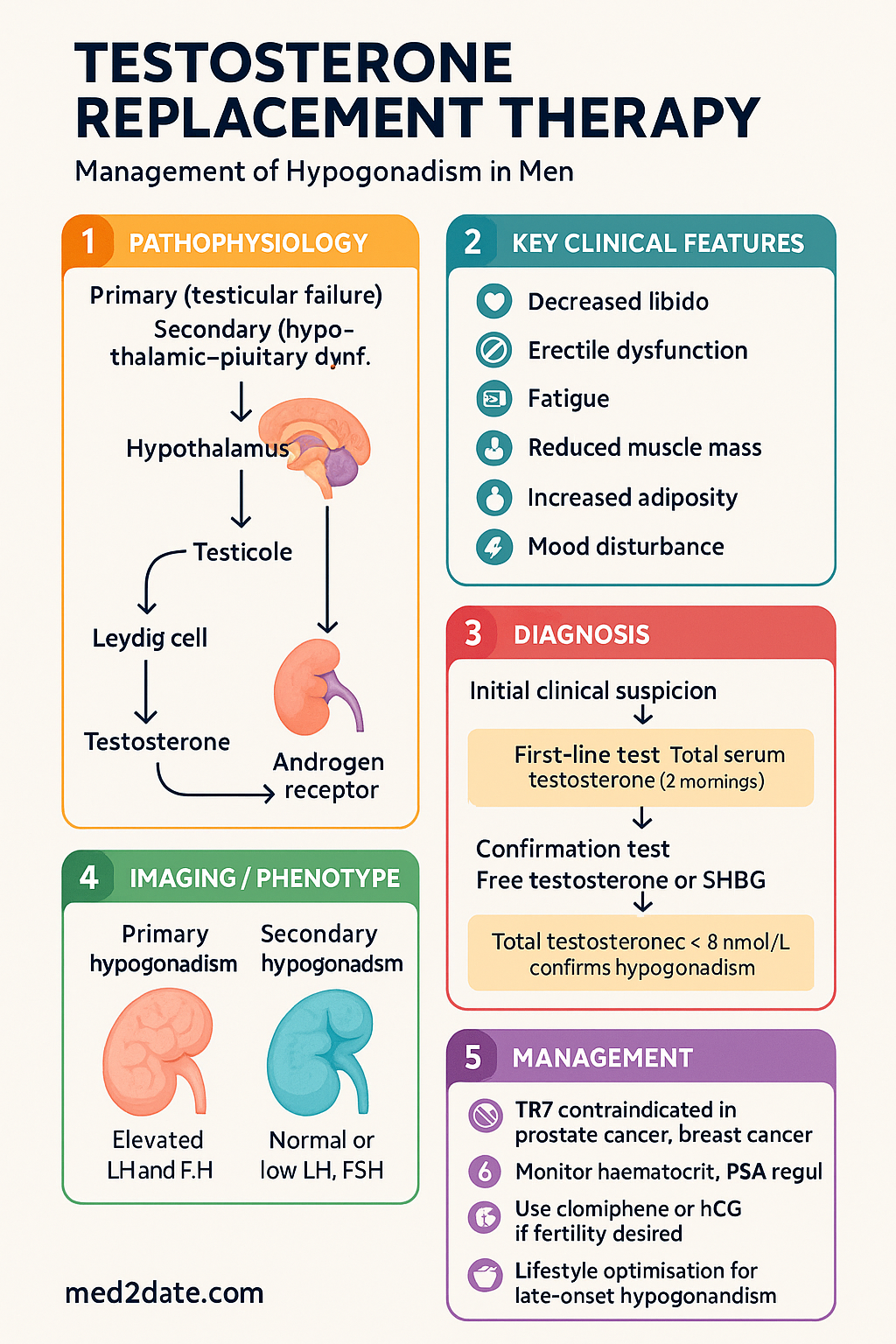
- Testosterone replacement therapy (TRT) is indicated for men with confirmed hypogonadism — consistently low serum testosterone (total T < 8 nmol/L on two morning samples) with associated symptoms.
- Hypogonadism may be primary (testicular failure) or secondary (hypothalamic–pituitary dysfunction); aetiology must be identified before initiating therapy.
- TRT is contraindicated in prostate cancer, breast cancer, uncontrolled heart failure, severe untreated obstructive sleep apnoea (OSA), polycythaemia (haematocrit > 0.54), and when fertility is desired.
- Australian PBS-listed options include testosterone undecanoate (Reandron® IM), testosterone enanthate (Primoteston Depot® IM), and testosterone undecanoate oral (Andriol Testocaps®).
- Transdermal testosterone (Testogel® 1% 50 mg sachets) is available but is not PBS-subsidised for most patients — authority required or private script.
- Initial monitoring: haematocrit, PSA, lipids, LFTs at baseline, 3 months, 6 months, then 6–12 monthly.
- Haematocrit > 0.54 requires dose reduction, phlebotomy, or cessation — thromboembolic risk increases significantly.
- PSA monitoring is essential; TRT is contraindicated in existing prostate cancer and a urology referral is required if PSA rises > 4.0 µg/L or increases by > 1.4 µg/L in 12 months.
- For men desiring fertility, TRT suppresses spermatogenesis via negative feedback on gonadotrophins — use clomiphene citrate or hCG instead.
- Late-onset hypogonadism (ageing-related) should be managed cautiously with lifestyle optimisation first; TRT only if sustained low levels with clear symptomatic benefit.
- Aboriginal and Torres Strait Islander men experience higher rates of chronic disease-related hypogonadism; culturally safe care, remote monitoring pathways, and PBS access are important considerations.
- Oral testosterone undecanoate must be taken with food containing at least 19 g of fat for adequate absorption — poor bioavailability with fasting.
🎧 Audio Brief
Introduction & Australian Epidemiology
Testosterone replacement therapy (TRT) is the cornerstone of management for men with confirmed hypogonadism — a clinical syndrome characterised by low circulating testosterone and associated symptoms including decreased libido, erectile dysfunction, fatigue, reduced muscle mass, increased adiposity, and mood disturbance.
The Endocrine Society of Australia and the Australasian Society of Clinical Immunology and Allergy (ASCIA) endorse that diagnosis requires both biochemical confirmation (total serum testosterone < 12 nmol/L on at least two early-morning fasting samples) and clinical symptomatology. Total testosterone between 8 and 12 nmol/L is considered equivocal and should prompt measurement of free testosterone or sex hormone-binding globulin (SHBG).
Australian epidemiology: Community-based studies estimate the prevalence of symptomatic hypogonadism at 5–8% of men aged 40–79 years, rising to 15–20% in men aged > 70 years. In the 2017–18 Australian Bureau of Statistics National Health Survey, testosterone prescribing increased approximately 4-fold over the preceding decade, with Reandron® (testosterone undecanoate 1000 mg IM) being the most commonly PBS-dispensed formulation. Chronic conditions prevalent in Australia — type 2 diabetes mellitus, obesity, opioid use, and obstructive sleep apnoea — are major contributors to functional hypogonadism.
Primary hypogonadism (hypergonadotrophic) accounts for approximately 30% of cases and includes Klinefelter syndrome (affecting ~1 in 600 Australian males), orchitis, testicular trauma, and cryptorchidism. Secondary hypogonadism (hypogonadotrophic) — including Kallmann syndrome, pituitary adenoma, and functional suppression — accounts for the remainder.
Indications & Contraindications
Indications for Testosterone Replacement Therapy
TRT is indicated when both biochemical and clinical criteria are met:
| Indication | Details |
|---|---|
| Primary hypogonadism | Klinefelter syndrome, bilateral anorchia, testicular torsion, orchidectomy, mumps orchitis, chemotherapy/radiation-induced gonadal failure |
| Secondary hypogonadism | Kallmann syndrome, idiopathic hypogonadotrophic hypogonadism, pituitary tumour/adenoma, hyperprolactinaemia (after treatment), haemochromatosis |
| Late-onset hypogonadism (LOH) | Age-related decline with total T consistently < 8 nmol/L and symptoms — use cautiously; lifestyle measures first |
| Functional hypogonadism | Obesity, type 2 DM, chronic opioid therapy, glucocorticoid use, HIV-related wasting — treat underlying cause first where possible |
Diagnostic Criteria
- Total serum testosterone < 8 nmol/L on two separate morning (8–10 am) fasting samples — confirms hypogonadism
- Total testosterone 8–12 nmol/L — equivocal zone: calculate free testosterone (using Vermeulen equation) or measure bioavailable testosterone
- Elevated LH and FSH → primary hypogonadism
- Normal or low LH and FSH → secondary hypogonadism → investigate pituitary (MRI pituitary, prolactin, iron studies)
- Prolactin > 1000 mIU/L → exclude prolactinoma before starting TRT
Absolute Contraindications
- Prostate cancer (known or suspected) — testosterone may stimulate growth
- Male breast cancer
- Polycythaemia with haematocrit > 0.54
- Uncontrolled or severe congestive heart failure (NYHA class III–IV)
- Desire for fertility in the next 6–12 months
- Hypersensitivity to testosterone or formulation excipients
Relative Contraindications / Cautions
- Severe untreated obstructive sleep apnoea — may worsen OSA; treat CPAP first
- Lower urinary tract symptoms (IPSS > 19) — monitor closely
- PSA > 4.0 µg/L without urological work-up
- Thrombophilia or history of venous thromboembolism (VTE)
- Epilepsy — testosterone may lower seizure threshold
- Severe hepatic impairment
Formulations & Dosing
The choice of formulation depends on patient preference, PBS availability, injection tolerance, and clinical context. The following formulations are available in Australia:
Target Serum Levels
The therapeutic target is a mid-range total testosterone of 15–20 nmol/L measured at trough (just before next injection) for injectable formulations. Avoid supraphysiological levels (> 30 nmol/L) which increase adverse effects without additional benefit.
Monitoring & Side Effects
Recommended Monitoring Schedule
Key Side Effects & Management
| Side Effect | Mechanism | Management |
|---|---|---|
| Polycythaemia (haematocrit > 0.54) | Erythropoietin stimulation | Dose reduction, therapeutic phlebotomy, or stop TRT |
| Acne / oily skin | Sebaceous gland stimulation | Topical agents; dose reduction if severe |
| Gynaecomastia | Peripheral aromatisation to oestradiol | Dose reduction; consider tamoxifen if symptomatic |
| Peripheral oedema | Fluid retention via mineralocorticoid effect | Reduce dose; diuretics if needed |
| Sleep apnoea worsening | Upper airway effects | Optimise CPAP; consider dose reduction |
| Infertility | GnRH suppression → ↓ LH/FSH | Stop TRT; use hCG or clomiphene if fertility desired |
| Mood / behavioural changes | CNS androgen receptor effects | Dose titration; psychiatric review if significant |
| Injection site pain / reaction | Oil-based depot formulation | Rotate sites; switch formulation if persistent |
Prostate Monitoring Detail
- Digital rectal examination (DRE) at baseline and annually
- PSA at baseline, 3 months, 6 months, then annually
- Refer to urology if PSA > 4.0 µg/L or velocity > 0.4 µg/L/year on two occasions
- TRT does not cause prostate cancer but may accelerate pre-existing occult disease
- Men on active surveillance for prostate cancer — TRT generally contraindicated; specialist decision only
Special Situations (Fertility, Ageing)
Fertility Preservation
Alternatives for hypogonadal men desiring fertility:
Recovery of spermatogenesis after discontinuing TRT may take 6–24 months and is unpredictable. Semen analysis should be performed before restarting TRT if fertility was previously desired. Pre-treatment sperm banking should be discussed with all men of reproductive age.
Late-Onset Hypogonadism (Ageing)
Testosterone levels decline approximately 1–2% per year after age 30. Late-onset hypogonadism (LOH) is characterised by total testosterone < 11 nmol/L (or free testosterone < 225 pmol/L) in conjunction with at least three sexual symptoms (decreased libido, erectile dysfunction, reduced morning erections).
Management approach for older men:
- Step 1 — Lifestyle optimisation: Weight loss (5–10% body weight can increase testosterone by 2–3 nmol/L), resistance exercise, sleep hygiene, alcohol reduction, opioid weaning if applicable
- Step 2 — Re-evaluate at 3–6 months: If persistent symptomatic low testosterone (total T < 8 nmol/L on repeat testing), consider TRT
- Step 3 — Cardiovascular risk assessment: The TRAVERSE trial (2023) demonstrated no significant increase in major adverse cardiovascular events (MACE) with TRT in men aged 45–80 years with cardiovascular risk factors — but polycythaemia management remains critical
- Avoid routine TRT for age-related decline without clear biochemical and symptomatic criteria — "well man" testosterone use is not evidence-based
Opioid-Induced Hypogonadism
Chronic opioid use suppresses GnRH pulsatility, causing secondary hypogonadism in up to 75% of men on long-term opioid therapy. Management priorities:
- Opioid dose reduction or rotation where possible
- TRT if symptomatic hypogonadism persists after opioid optimisation
- Monitor closely — polypharmacy interactions and fall risk in older patients
Investigations
The following investigations are recommended before initiating TRT:
Special Populations
Aboriginal and Torres Strait Islander Health Considerations
📚 References
- 1. Yeap BB, Grossmann M, McLachlan RI, et al. Endocrine Society of Australia position statement on male hypogonadism (part 1): assessment and indications for testosterone therapy. Medical Journal of Australia. 2016;205(4):173-178.
- 2. Grossmann M, Ng Tang Fui M, Cheung AS. Late-onset hypogonadism — testosterone therapy in older men. Medical Journal of Australia. 2020;212(8):367-372.
- 3. Lincoff AM, Bhasin S, Flevaris P, et al. Cardiovascular safety of testosterone-replacement therapy. New England Journal of Medicine. 2023;389(2):107-117. (TRAVERSE trial)
- 4. Bhasin S, Brito JP, Cunningham GR, et al. Testosterone therapy in men with hypogonadism: an Endocrine Society clinical practice guideline. Journal of Clinical Endocrinology & Metabolism. 2018;103(5):1715-1744.
- 5. Grossmann M, Matsumoto AM. A perspective on middle-aged and older men with functional hypogonadism: focus on holistic management. Journal of Clinical Endocrinology & Metabolism. 2017;102(3):1067-1075.
- 6. Australian Institute of Health and Welfare (AIHW). The health of Aboriginal and Torres Strait Islander peoples 2023. AIHW, Canberra. 2023.
- 7. Australian Government Department of Health. Pharmaceutical Benefits Scheme — Testosterone. Available at: pbs.gov.au. Accessed 2024.
- 8. Dohle GR, Arver S, Bettocchi C, Jones TH, Kliesch S, Punab M. Guidelines on male hypogonadism. European Association of Urology. 2023.
- 9. Tajar A, Forti G, O'Neill TW, et al. Characteristics of secondary, primary, and compensated hypogonadism in aging men: evidence from the European Male Ageing Study. Journal of Clinical Endocrinology & Metabolism. 2010;95(4):1810-1818.
- 10. Royal Australian College of General Practitioners (RACGP). RACGP aged care clinical guide (Silver Book) — Endocrinology. 6th edition. 2023.
- 11. Corona G, Rastrelli G, Maggi M. Diagnosis and treatment of late-onset hypogonadism: systematic review and meta-analysis of TRT outcomes. Best Practice & Research Clinical Endocrinology & Metabolism. 2017;31(4):377-396.
- 12. Cheung AS, de Rooij M, Vlot MC, et al. Opioid-induced hypogonadism in men and women: a systematic review. The Lancet Diabetes & Endocrinology. 2022;10(8):587-598.