📋 Key Information Summary
- Hyperthyroidism management requires aetiological diagnosis; Graves' disease, toxic multinodular goitre, and toxic adenoma are most common in Australia.
- First-line antithyroid drug (ATD) for most non-pregnant adults is carbimazole (Mycril®); propylthiouracil (PTU) reserved for first trimester pregnancy, thyroid storm, or carbimazole intolerance.
- Carbimazole initial dose 15–40 mg/day, titrated to lowest维持 dose maintaining euthyroidism; typical course 12–18 months for Graves' disease.
- Major ATD risk is agranulocytosis (~0.2–0.5%); patients must be counselled to stop drug and seek urgent FBC if febrile illness or sore throat develops.
- Radioiodine (I-131) is definitive therapy for Graves' disease and toxic nodular disease; contraindicated in pregnancy and breastfeeding.
- Post-radioiodine hypothyroidism is expected (≥50% at 10 years); requires lifelong levothyroxine monitoring and replacement.
- Total thyroidectomy indicated for large goitre with compressive symptoms, suspected malignancy, or failed/contraindicated medical/radioiodine therapy.
- Pregnancy: PTU in first trimester, switch to carbimazole in second/third trimester; aim for free T4 at or just above upper normal limit.
- Paediatric Graves': ATDs are first-line; surgery if ATD failure/toxicity; radioiodine generally avoided in children <10 years.
- Thyroid storm is a medical emergency with high mortality; requires ICU admission, beta-blockade, high-dose PTU, iodine, and corticosteroids.
- Monitor thyroid function every 4–6 weeks during ATD titration, then every 3–6 months once stable.
- Aboriginal and Torres Strait Islander peoples have higher prevalence of thyroid disease and may face barriers to specialist access; culturally safe care and long-term follow-up are essential.
🎧 Audio Brief
Introduction & Australian Epidemiology
Hyperthyroidism, or thyrotoxicosis, is a clinical state resulting from excess circulating thyroid hormones. Management is guided by the underlying aetiology, severity, patient age, comorbidities, and reproductive plans. In Australia, the most common causes are Graves' disease (an autoimmune condition), toxic multinodular goitre, and toxic adenoma.
Australian epidemiological data indicate a prevalence of hyperthyroidism of approximately 1–2%, with a female-to-male ratio of 5–10:1. Graves' disease is the predominant cause in younger adults, while toxic nodular disease increases in prevalence with age. Access to care, particularly endocrinology and nuclear medicine services, varies significantly between metropolitan and regional/remote areas.
The three definitive treatment modalities are antithyroid drugs (ATDs), radioactive iodine (RAI) therapy, and thyroidectomy. The choice is individualised, considering efficacy, side-effect profiles, patient preference, and long-term outcomes.
Pathophysiology
Thyroid hormone synthesis and release are regulated by the hypothalamic-pituitary-thyroid (HPT) axis. Hyperthyroidism arises from autonomous thyroid hormone production, independent of TSH stimulation.
Key Aetiologies:
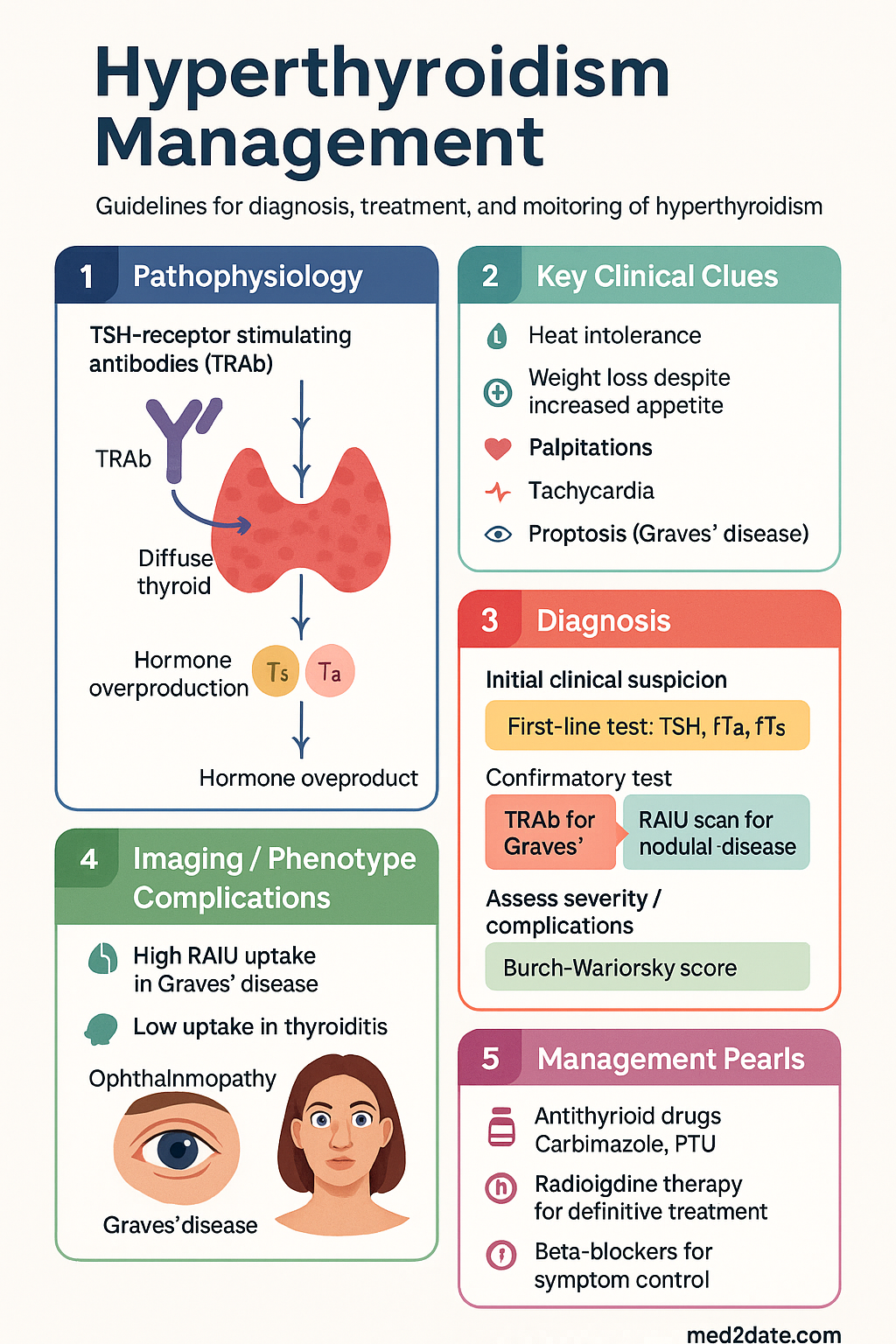
- Graves' disease: TSH-receptor stimulating antibodies (TRAb) cause diffuse thyroid stimulation and hormone overproduction. It is associated with extrathyroidal manifestations like ophthalmopathy.
- Toxic multinodular goitre: Somatic mutations lead to autonomously functioning nodules, more common in iodine-deficient regions and the elderly.
- Toxic adenoma: A single autonomously functioning benign adenoma.
- Thyroiditis: Destructive processes (e.g., subacute, postpartum) cause release of preformed hormone, typically resulting in transient thyrotoxicosis.
- Drug-induced: Amiodarone-induced thyrotoxicosis (AIT) has two types: Type 1 (excess synthesis) and Type 2 (destructive thyroiditis).
Clinical Presentation & Diagnostic Criteria
Presentation ranges from asymptomatic biochemical abnormality to life-threatening thyroid storm.
Typical Symptoms & Signs:
| System | Symptoms | Signs |
|---|---|---|
| Constitutional | Heat intolerance, weight loss despite increased appetite, fatigue | Warm moist skin, fine tremor |
| Cardiovascular | Palpitations, dyspnoea on exertion | Tachycardia, atrial fibrillation, systolic hypertension, high-output cardiac failure |
| Neuropsychiatric | Anxiety, irritability, insomnia | Hyperreflexia, lid lag |
| Musculoskeletal | Proximal myopathy | Muscle weakness |
| Reproductive | Oligomenorrhoea, gynaecomastia | |
| Graves'-specific | Eye irritation, diplopia | Proptosis, lid retraction, pretibial myxoedema, thyroid acropachy |
Diagnostic Criteria:
Diagnosis is biochemical:
- Primary hyperthyroidism: Suppressed TSH (<0.1 mIU/L) with elevated free T4 (fT4) and/or free T3 (fT3).
- Subclinical hyperthyroidism: Suppressed TSH with normal fT4 and fT3.
- Aetiological diagnosis: TSH-receptor antibodies (TRAb) for Graves', uptake scan (RAIU) for nodular disease vs. thyroiditis.
Investigations
Initial and aetiological investigations are essential for guiding therapy.
Risk Stratification & Severity Scoring
Severity is assessed clinically and biochemically to determine urgency of treatment.
Management Overview
Treatment goals are to restore euthyroidism, manage symptoms, and select definitive therapy to prevent recurrence.
General Measures:
- Beta-blockers: Propranolol 20–40 mg PO 6–8 hourly (or long-acting 80–160 mg daily) for symptom control of adrenergic symptoms (palpitations, tremor, anxiety).
- Avoid iodine-rich contrast media and medications (e.g., amiodarone) where possible.
- Patient education on disease course, medication adherence, and warning signs of agranulocytosis and thyroid storm.
Antithyroid Drugs (Carbimazole/PTU)
Mechanism & Choice
ATDs inhibit thyroid hormone synthesis by blocking thyroid peroxidase. Carbimazole (converted to methimazole) is preferred due to once-daily dosing and lower hepatotoxicity risk. PTU has additional peripheral T4-to-T3 conversion inhibition.
Regimen Strategies
- Titration regimen: Start high, taper to lowest维持 dose. Most common in Australia.
- Block-and-replace: High-dose ATD + levothyroxine. Used for rapid control or unstable thyrotoxicosis. Not for routine Graves' disease.
Radioiodine Therapy (I-131)
Radioiodine (I-131) is a safe, effective, and commonly used definitive therapy for Graves' disease and toxic nodular goitre in Australia.
Indications & Contraindications
- Relapse after ATD therapy.
- ATD intolerance or non-adherence.
- Toxic multinodular goitre or toxic adenoma.
- Patient preference for definitive therapy.
- Pregnancy (absolute).
- Breastfeeding.
- Severe active Graves' ophthalmopathy (may exacerbate).
- Inability to comply with radiation safety precautions.
Procedure & Outcomes
- Pre-treatment: Discontinue ATDs (carbimazole 5–7 days, PTU 1–2 weeks) before therapy. Low-iodine diet may be advised.
- Dosing: Fixed dose (e.g., 400–600 MBq for Graves') or calculated based on gland size/uptake. Administered orally as a capsule.
- Post-therapy: Radiation safety precautions for 2–4 weeks (avoid prolonged close contact with children/pregnant women).
- Outcome: Hypothyroidism is the goal (≥50% at 1 year for Graves'). Requires lifelong levothyroxine replacement and monitoring.
Thyroidectomy
Surgery offers rapid, definitive treatment but carries operative risks. Performed by a high-volume endocrine surgeon for optimal outcomes.
Indications
- Large goitre with compressive symptoms (dysphagia, dyspnoea).
- Coexisting thyroid malignancy or suspicious nodule.
- Severe ophthalmopathy (preferred over radioiodine).
- Patient preference, especially in women planning future pregnancy.
- Failed or contraindicated ATD and radioiodine therapy.
Pre-operative, Operative & Post-operative Care
Special Circumstances (Pregnancy, Children)
Pregnancy
Management aims to control hyperthyroidism with minimal fetal exposure. Untreated hyperthyroidism increases risk of pre-eclampsia, preterm birth, and low birth weight.
- First trimester: PTU is first-line due to rare but serious carbimazole-associated fetal malformations (aplasia cutis, choanal atresia).
- Second & third trimester: Switch to carbimazole due to PTU-associated hepatotoxicity risk.
- Dosing: Use lowest possible维持 dose. Target fT4 at or just above the upper limit of normal.
- Monitoring: TFTs every 4 weeks. TRAb cross placenta; check at 18–22 weeks if high risk (previous surgery/RAI) to predict neonatal thyrotoxicosis.
- Definitive therapy: Surgery (if essential) in second trimester. Radioiodine is absolutely contraindicated.
Paediatric Hyperthyroidism
Graves' disease is the most common cause. Management differs from adults.
- First-line: ATD therapy (carbimazole preferred). Dose based on weight. Duration often longer than adults (3–5 years).
- Second-line: Total thyroidectomy if ATD failure, toxicity, or non-adherence. Requires experienced paediatric surgeon.
- Radioiodine: Generally avoided in children <10 years due to theoretical long-term malignancy risk. May be considered in older children after failed ATDs.
- Monitoring: Close supervision of growth, development, and school performance.
Monitoring
Regular monitoring is essential for safety and efficacy across all treatment modalities.
Every 4–6 weeks during initial titration. Once euthyroid, every 3–6 months. Check FBC and LFTs at baseline and if symptoms arise. Monitor for relapse after cessation.
TFTs 4–6 weeks post-treatment, then every 2–3 months in first year, then annually once hypothyroid on stable levothyroxine.
Check calcium 6–12 hours post-op and monitor for symptoms of hypocalcaemia. TFTs 4–6 weeks post-op to guide levothyroxine dose, then annually.
Other Special Populations
Thyroid disorders, including hyperthyroidism, are prevalent in Aboriginal and Torres Strait Islander peoples. Management must be culturally safe and address specific barriers.
📚 References
- 1. Australian Institute of Health and Welfare (AIHW). Thyroid disease in Australia. Cat. no. PHE 249. Canberra: AIHW; 2020.
- 2. The Royal Australian College of General Practitioners (RACGP). Thyroid disease: diagnosis and management. East Melbourne, Vic: RACGP; 2023.
- 3. Ross DS, Burch HB, Cooper DS, et al. 2016 American Thyroid Association Guidelines for Diagnosis and Management of Hyperthyroidism and Other Causes of Thyrotoxicosis. Thyroid. 2016;26(10):1343-1421.
- 4. Kahaly GJ, Bartalena L, Hegedüs L, et al. 2018 European Thyroid Association Guideline for the Management of Graves' Hyperthyroidism. Eur Thyroid J. 2018;7(4):167-186.
- 5. Australian Government Department of Health. PBS Online: Carbimazole, Propylthiouracil. Accessed 2024.
- 6. Endocrine Society of Australia (ESA). Position Statement: Management of Hyperthyroidism in Pregnancy. 2022.
- 7. National Health and Medical Research Council (NHMRC). National Statement on Ethical Conduct in Human Research. Canberra: NHMRC; 2023 (Updated).
- 8. Aboriginal and Torres Strait Islander Health Practice Board of Australia. Cultural safety framework. 2022.
- 9. Burch HB, Wartofsky L. Life-threatening thyrotoxicosis. Thyroid storm. Endocrinol Metab Clin North Am. 1993;22(2):263-277.
- 10. Smith TJ, Hegedüs L. Graves' Disease. N Engl J Med. 2016;375(16):1552-1565.
- 11. Australian Commission on Safety and Quality in Health Care (ACSQHC). Australian Atlas of Healthcare Variation. Sydney: ACSQHC; 2023.
- 12. Stagnaro-Green A, Abalovich M, Alexander E, et al. Guidelines of the American Thyroid Association for the diagnosis and management of thyroid disease during pregnancy and postpartum. Thyroid. 2011;21(10):1081-1125.