📋 Key Information Summary
- Graves' disease is the most common cause of hyperthyroidism in Australia, accounting for 60–80% of cases; Hashimoto's thyroiditis is the leading cause of hypothyroidism.
- Anti-TSH receptor antibodies (TRAb/TSI) are pathognomonic for Graves' disease and distinguish it from other causes of thyrotoxicosis.
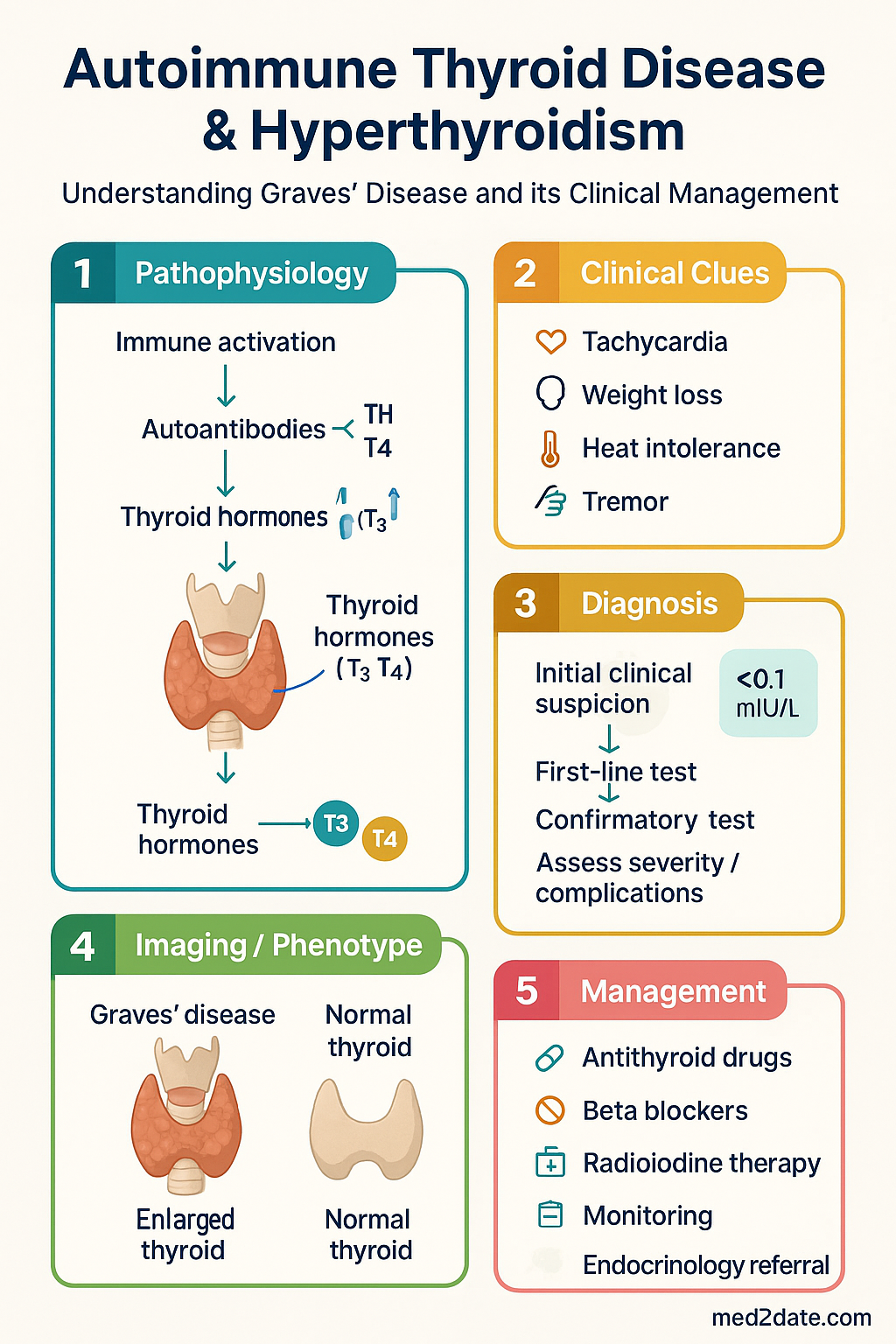
- Classic clinical features include weight loss, heat intolerance, tremor, tachycardia, anxiety, and diffuse goitre with or without Graves' orbitopathy.
- First-line investigation: serum TSH, free T4, free T3 (MBS-rebated); TRAb confirms Graves' disease and may obviate isotope scanning.
- Carbimazole (Mazda®) is the preferred antithyroid drug in Australia; PTU is reserved for first trimester pregnancy and thyroid storm.
- Antithyroid drug therapy typically continues for 12–18 months; remission rate is ~50% after a first course.
- Radioactive iodine (I-131) is a definitive therapy widely available in Australia; lifelong hypothyroidism is expected in >80% of patients.
- Thyroid storm is a medical emergency with high mortality — treat with PTU, beta-blockers, iodine (Lugol's), glucocorticoids, and ICU admission.
- Agranulocytosis occurs in ~0.2–0.5% of patients on antithyroid drugs — instruct all patients to present urgently for FBC if sore throat or fever develops.
- Graves' orbitopathy requires multidisciplinary management; smoking cessation is the single most important modifiable risk factor.
- Pregnancy planning is essential — antithyroid drugs must be adjusted pre-conception; TRAb crosses the placenta and may cause neonatal thyrotoxicosis.
- Aboriginal and Torres Strait Islander peoples may have higher prevalence of autoimmune thyroid disease with barriers to specialist access in remote areas.
- Post-radioiodine or post-surgical hypothyroidism requires lifelong levothyroxine replacement with regular TSH monitoring.
🎧 Audio Brief
Introduction & Australian Epidemiology
Autoimmune thyroid disease encompasses a spectrum of organ-specific autoimmune disorders in which the immune system targets thyroid antigens, leading to either glandular destruction (Hashimoto's thyroiditis) or stimulation (Graves' disease). These conditions are among the most prevalent autoimmune disorders worldwide and represent a significant burden of disease in Australian primary care and specialist endocrinology practice.
Graves' disease is the most common cause of hyperthyroidism, responsible for 60–80% of thyrotoxicosis cases in iodine-replete populations such as Australia. It is caused by stimulatory autoantibodies directed against the thyroid-stimulating hormone (TSH) receptor. The incidence in Australia is estimated at 1–2 per 1,000 population per year, with a marked female predominance (female-to-male ratio approximately 5–10:1). Peak incidence occurs between ages 30–50 years.
Hashimoto's thyroiditis (chronic lymphocytic thyroiditis) is the most common cause of hypothyroidism in iodine-sufficient regions. It is characterised by antibodies against thyroid peroxidase (TPOAb) and thyroglobulin (TgAb), leading to gradual thyroid gland destruction. Prevalence of TPO antibodies in the Australian population is approximately 10–15% in women and 3–5% in men, though not all develop clinical hypothyroidism.
Australia's iodine status has improved following the mandatory iodisation of bread salt (2009), reducing iodine-deficiency-related thyroid disease. However, mild iodine insufficiency persists in some populations, particularly in Tasmania and parts of Victoria. Autoimmune thyroid disease remains the dominant thyroid disorder encountered in Australian clinical practice.
| Feature | Graves' Disease | Hashimoto's Thyroiditis |
|---|---|---|
| Thyroid function | Hyperthyroidism (typically) | Hypothyroidism (most common outcome) |
| Key autoantibodies | TRAb (TSI, TBII) | TPOAb, TgAb |
| Mechanism | Antibody-mediated TSH receptor stimulation | Lymphocytic infiltration and gland destruction |
| Goitre | Diffuse, often bruit present | Diffuse, firm, rubbery |
| Extrathyroidal features | Orbitopathy, pretibial myxoedema, acropachy | Associated with other autoimmune conditions |
| Australian prevalence | ~1–2% | ~5–10% (TPOAb positive) |
Pathophysiology & Autoantibodies
Graves' Disease — Immunopathogenesis
Graves' disease results from a breakdown in immune tolerance to thyroid self-antigens, predominantly the TSH receptor (TSHR). Pathogenic IgG autoantibodies (thyroid-stimulating immunoglobulins, TSI) bind to the TSHR on thyroid follicular cells, mimicking the action of TSH. This activates the Gsα–adenylyl cyclase–cAMP pathway, leading to:
- Increased iodine uptake and thyroid hormone synthesis (T4 and T3)
- Thyroid follicular cell hypertrophy and hyperplasia (goitre)
- Increased thyroid vascularity (bruit on auscultation)
Loss of immune tolerance involves genetic susceptibility (HLA-DR3, CTLA-4, PTPN22 polymorphisms), environmental triggers (stress, smoking, excess iodine, infection, postpartum immune rebound), and immune dysregulation including reduced regulatory T-cell function and Th1/Th17 skewing.
Hashimoto's Thyroiditis — Immunopathogenesis
Hashimoto's thyroiditis is characterised by CD4+ and CD8+ T-cell-mediated destruction of thyroid follicular cells, aided by complement-fixing anti-TPO antibodies. The gland undergoes progressive lymphocytic infiltration, germinal centre formation, follicular cell apoptosis, and fibrosis, ultimately leading to hypothyroidism. A transient thyrotoxic phase ("Hashitoxicosis") may occur during early gland destruction due to release of preformed thyroid hormone.
Key Autoantibodies in Clinical Practice
| Antibody | Target | Clinical Utility | Availability in Australia |
|---|---|---|---|
| TRAb (TSH Receptor Antibody) | TSH receptor | Confirms Graves' disease; predicts neonatal thyrotoxicosis; monitors relapse risk | Widely available (MBS item 66827). Third-generation assays (TBII) preferred. |
| TSI (Thyroid-Stimulating Immunoglobulin) | TSH receptor (stimulatory) | Bioassay; high sensitivity for Graves'. Less commonly requested than TRAb in Australia. | Refer to specialised laboratories |
| TPOAb (Thyroid Peroxidase Antibody) | Thyroid peroxidase | Present in ~95% Hashimoto's, ~75% Graves'. Predicts progression to hypothyroidism. | Widely available (MBS item 66826) |
| TgAb (Thyroglobulin Antibody) | Thyroglobulin | Complementary to TPOAb; important in thyroid cancer surveillance (interferes with Tg assay) | Widely available (MBS item 66826) |
Clinical Features of Hyperthyroidism
The clinical presentation of hyperthyroidism reflects the effects of excess thyroid hormone on virtually every organ system. Severity ranges from subclinical (suppressed TSH, normal free T4/T3) to life-threatening thyroid storm.
Systemic Manifestations
| System | Features |
|---|---|
| Metabolic | Weight loss despite increased appetite, heat intolerance, diaphoresis, increased basal metabolic rate |
| Cardiovascular | Sinus tachycardia, atrial fibrillation (10–25%), palpitations, systolic hypertension with widened pulse pressure, high-output cardiac failure |
| Neuropsychiatric | Anxiety, irritability, emotional lability, insomnia, fine tremor, hyperreflexia |
| Musculoskeletal | Proximal myopathy, osteoporosis (increased bone turnover), periodic paralysis (rare, more common in Asian males) |
| Gastrointestinal | Increased bowel frequency, hyperdefecation (not true diarrhoea) |
| Reproductive | Oligomenorrhoea, amenorrhoea, gynaecomastia (males), reduced fertility |
| Dermatological | Warm moist skin, onycholysis (Plummer's nails), hair thinning, pretibial myxoedema (Graves' specific) |
| Ophthalmological | Lid lag, lid retraction (sympathetic); Graves' orbitopathy — proptosis, periorbital oedema, diplopia, compressive optic neuropathy |
Graves'-Specific Features
- Diffuse goitre: Smooth, symmetrical enlargement, often with an audible bruit or palpable thrill due to increased vascularity.
- Graves' orbitopathy (GO): Present in 25–50% clinically (mild in most). Smoking is the strongest modifiable risk factor. Clinical Activity Score (CAS) guides management. Sight-threatening disease (dysthyroid optic neuropathy) occurs in <5%.
- Pretibial myxoedema: Localised non-pitting dermopathy over the pretibial area. Occurs in ~1–4% of Graves' patients.
- Thyroid acropachy: Rare (0.1–1%); clubbing, periosteal new bone formation, soft tissue swelling of digits.
Thyroid Storm — Medical Emergency
The Burch–Wartofsky Point Scale (BWPS) aids diagnosis:
Investigations
First-Line Thyroid Function Tests
Aetiological Investigations
Additional Investigations
- FBC: Baseline before antithyroid drug therapy (risk of agranulocytosis). Recheck if fever/sore throat during treatment.
- LFTs: Baseline — both hyperthyroidism and antithyroid drugs can cause hepatotoxicity.
- ECG: Assess for atrial fibrillation, which occurs in 10–25% of hyperthyroid patients.
- Bone density (DEXA): Consider in postmenopausal women or prolonged hyperthyroidism — risk of osteoporosis.
- Lipid profile: Hyperthyroidism causes low cholesterol; hypothyroidism causes elevated cholesterol.
Management of Graves' Disease
The three definitive treatment modalities for Graves' disease are antithyroid drug (ATD) therapy, radioactive iodine (RAI), and thyroidectomy. Treatment choice depends on disease severity, patient preference, presence of orbitopathy, age, comorbidities, and local expertise. All patients should be managed in collaboration with an endocrinologist.
Symptomatic Treatment (Initial — All Patients)
Beta-blockers provide rapid symptomatic relief while awaiting antithyroid drug effect.
Antithyroid Drug Therapy — Thionamides
Dosing Strategies
- Titrating regimen (preferred): Start with higher dose of carbimazole (15–30 mg), titrate down to lowest maintenance dose as T4 normalises. Lower rate of side effects than block-and-replace.
- Block-and-replace regimen: High-dose carbimazole (30–40 mg) plus levothyroxine (100–150 µg). Higher side-effect rate; reserved for difficult-to-control cases. Requires close monitoring.
Definitive Therapy
| Modality | Indications | Advantages | Disadvantages |
|---|---|---|---|
| Radioactive Iodine (I-131) | Relapsed Graves', large goitre, contraindication to surgery, patient preference. Widely available across Australia (Nuclear Medicine). | Definitive cure in >80%. Non-invasive. Cost-effective. Outpatient procedure. | Hypothyroidism in >80% (lifelong thyroxine). May worsen orbitopathy — avoid if active moderate-severe GO. Contraindicated in pregnancy/lactation (6-month washout). |
| Total Thyroidectomy | Large goitre, suspected malignancy, severe orbitopathy, patient preference, failed RAI. Endocrine surgeon preferred. | Immediate definitive cure. Avoids radiation. Preferred if coexistent thyroid cancer suspected. | Surgical risks: recurrent laryngeal nerve palsy (1–2%), hypoparathyroidism (1–3%), bleeding. Requires general anaesthesia. Lifelong thyroxine. |
Thyroid Storm Management (Emergency)
Graves' Orbitopathy — Multidisciplinary Approach
All patients with Graves' disease should be assessed for orbitopathy. Management requires collaboration between endocrinology, ophthalmology, and in severe cases, surgery.
- Smoking cessation: Single most important intervention. Smoking doubles the risk of orbitopathy and reduces treatment response.
- Mild GO (CAS <3): Selenium 100 µg PO BD (evidence from European trial), artificial tears, sunglasses, monitor.
- Moderate-to-severe active GO (CAS ≥3): IV methylprednisolone pulse therapy (evidence-based). Refer to ophthalmology/endocrinology. Consider orbital radiotherapy.
- Sight-threatening GO: Urgent IV pulse methylprednisolone. Surgical decompression if no response. This is an emergency.
- Teprotumumab (anti-IGF-1R monoclonal antibody) — not currently PBS-listed in Australia; available through clinical trials or private prescription.
Monitoring on Antithyroid Drugs
Relapse Prediction & Definitive Therapy Decision
| Factor | Lower Relapse Risk | Higher Relapse Risk |
|---|---|---|
| Goitre size | Small or no goitre | Large goitre |
| TRAb at withdrawal | Negative | Persistently positive / high titre |
| Severity at diagnosis | Mild thyrotoxicosis | Severe thyrotoxicosis |
| Smoking | Non-smoker | Current smoker |
| Duration to euthyroidism | <3 months | >6 months |
Special Populations
Aboriginal and Torres Strait Islander Health Considerations
📚 References
- 1. Ross DS, Burch HB, Cooper DS, et al. 2016 American Thyroid Association guidelines for diagnosis and management of hyperthyroidism and other causes of thyrotoxicosis. Thyroid. 2016;26(10):1343–1421.
- 2. Kahaly GJ, Bartalena L, Hegedüs L, et al. 2018 European Thyroid Association guideline for the management of Graves' hyperthyroidism. Eur Thyroid J. 2018;7(4):167–186.
- 3. Bartalena L, Baldeschi L, Boboridis K, et al. The 2016 European Thyroid Association/European Group on Graves' Orbitopathy guidelines for the management of Graves' orbitopathy. Eur Thyroid J. 2016;5(1):9–26.
- 4. Alexander EK, Pearce EN, Brent GA, et al. 2017 guidelines of the American Thyroid Association for the diagnosis and management of thyroid disease during pregnancy and the postpartum. Thyroid. 2017;27(3):315–389.
- 5. Australian Institute of Health and Welfare (AIHW). Thyroid disorders in Australia. Cat. no. PHE 252. Canberra: AIHW; 2020.
- 6. Liang J, Zeng W, Fang F, et al. Clinical analysis of Hashimoto thyroiditis coexistent with thyroid cancer in 139 cases. Int J Endocrinol. 2017;2017:2376834.
- 7. Burch HB, Wartofsky L. Life-threatening thyrotoxicosis: thyroid storm. Endocrinol Metab Clin North Am. 1993;22(2):263–277.
- 8. Smith TJ, Hegedüs L, Douglas RS. Role of insulin-like growth factor-1 (IGF-1) pathway in thyroid-associated ophthalmopathy. Pharmacol Ther. 2012;136(3):327–335.
- 9. Australian Government Department of Health. MBS Online — Medicare Benefits Schedule. Available at: www.mbsonline.gov.au. Accessed 2024.
- 10. National Health and Medical Research Council (NHMRC). Iodine supplementation for pregnant and breastfeeding women. NHMRC Public Statement. Canberra: NHMRC; 2010.
- 11. RACGP. Management of thyroid conditions in general practice. In: RACGP Red Book. Melbourne: RACGP; 2023.
- 12. Aboriginal and Torres Strait Islander Health Practice Board of Australia. Culturally safe health care. Melbourne: AHPRA; 2023.
- 13. Wémeau JL, Sadoul JL, d'Herbomez M, et al. Guidelines of the French Society of Endocrinology for the management of thyroid nodules. Ann Endocrinol (Paris). 2011;72(4):251–281.